
Article of the week: Dutch GPs influenced by ERSPC PSA study
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video of Miss van der Meer and Dr Blanker discussing their article.
If you only have time to read one article this week, it should be this one.
Impact of the European Randomized Study of Screening for Prostate Cancer (ERSPC) on prostate-specific antigen (PSA) testing by Dutch general practitioners
Saskia Van der Meer, Boudewijn J. Kollen*, Willem H. Hirdes, Martijn G. Steffens, Josette E.H.M. Hoekstra-Weebers†, Rien M. Nijman‡ and Marco H. Blanker*
Department of Urology, Isala Clinics, Zwolle, and Departments of *General Practice, †Psychosocial services and ‡Urology, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands
OBJECTIVE
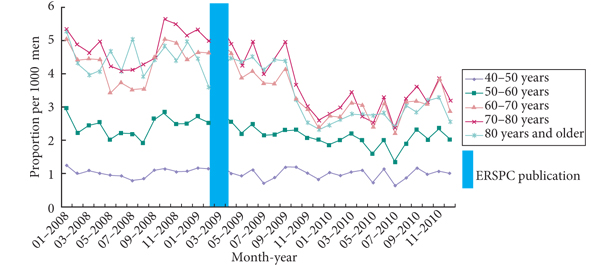
• To determine the impact of the European Randomized Study of Screening for Prostate Cancer (ERSPC) publication in 2009 on prostate-specific antigen (PSA) level testing by Dutch general practitioners (GPs) in men aged ≥40 years.
MATERIALS AND METHODS
• Retrospective study with a Dutch insurance company database (containing PSA test claims) and a large district hospital-laboratory database (containing PSA-test results).
• The difference in primary PSA-testing rate as well as follow-up testing before and after the ERSPC was tested using the chi-square test with statistical significance at P < 0.05.
RESULTS
• Decline in PSA tests 4 months after ERSPC publication, especially for men aged ≥60 years.
• Primary testing as well as follow-up testing decreased, both for PSA levels of <4 ng/mL as well as for PSA levels of 4–10 ng/mL.
• Follow-up testing after a PSA level result of >10 ng/mL moderately increased (P = 0.171).
• Referral to a urologist after a PSA level result of >4 ng/mL decreased slightly after the ERSPC publication (P = 0.044).
CONCLUSIONS
• After the ERSPC publication primary PSA testing as well as follow-up testing decreased.
• Follow-up testing seemed not to be adequate after an abnormal PSA result. The reasons for this remain unclear.
Read Previous Articles of the Week


We promised Quality – here it is again. This article and the editorial from Fritz Schroder are must reads for all urologists. I wonder how Bal Carter’s AUA guideline is going to affect the picture further. Wait for that article to cause further debate in the BJUI (it is in the pipeline). The blog during the AUA led to a heated online discussion led by Tony Costello who was our Visiting Professor from Australia at Guy’s last week. May I request our readers to join this important discussion.
Prokar
Congratulations on a very intriguing article. Despite showing that PSA screening definitely saves some lives the reaction of the Dutch seems to be that it doesn’t save enough to keep PSA testing levels high in the community.
It is difficult to know what the effect on PSA testing in the UK will be over the same time period as different countries tend to have separate social and cultural views on this. I would think that UK PSA testing wouldn’t have changed much in this time period. The ERSPC was not really known about by GPs in the UK whereas it was mainstream in this area of Holland. Our UK PSA testing level is i believe only 5-10% depending on the geographical area so quite low to start with..
Definitely food for thought though.
Not only urologist, nurse practitioners and physician assistants can benefit from these studies. Thank you Fritz Schröder!
This is an important article and a fantastic editorial. I wonder how many UK GPs would even be aware that PSA screening studies exist and have reported. My experience from a recent GP educational session I ran was that PSA, causes lots of anxiety both in patients and in GPs. They don’t have the time to read details guidance on everything they receive they look for ‘headlines.’ It would appear here that perhaps the headline was misinterpreted by the Dutch GPs. My concern is that re-testing after a raised PSA (4-10) reduced, some men with clinically significant prostate cancer will therefore not necessarily know that their PSA is increasing and may have been falsely reassured.
As mentioned in our response to the editorial comment of professor Schröder, we also encounter thoughts of GPs that PSA testing is wrong. This was not the message of the Dutch College of GPs (NHG). In the communication of the college send with the publication of the ERSPC findings, reluctance towards screening was advocated, based on the very large number needed to screen/treat. Nowhere, however, did the college state that increased PSA levels need no follow-up. In the 2004 GP-guideline it was, however, unclear what the policy for mildly increased levels should be. In the renewed guideline (published in March 2013) the advices for follow up were clarified.
We believe that if a patient requests for prostate cancer screening and is informed about the pros and cons of PSA testing, increased levels should prompt further analyse (which is the current clear statement in the GP guideline). Otherwise, the test should not have been done in the first place. With this policy (in which all patients with a PSA level > 4 ng/ml should be referred to an urologist), it is known that the majority of these patients will appear not to have prostate cancer. It might be that this knowledge influences final decisions for referral, both for GPs and for patients. We hope to elucidate these reasons for not performing any follow-up in these patients in our further study.
Thanks Marco. This additional information is very helpful for readers of the BJUI. I hope that you will consider submitting your further study to us in due course.
Great work. Congratulations!!