Editorial: Impact of warm ischaemia time during partial nephrectomy on renal function – is it really a matter of time?
In the latest edition of the BJUI, Lee et al. [1] have revisited the question of defining the ideal limit of warm ischaemia time (WIT) and its impact on postoperative renal function in patients undergoing partial nephrectomy (PN).
Partial nephrectomy has replaced radical nephrectomy as the preferred treatment for T1 renal masses. This publication challenges the theory that ischaemic nephropathy is inevitable if the renal vessels are clamped beyond 30 min, leading to a long-term decline in renal function.
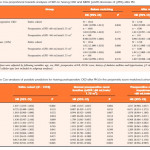
The authors in this series are to be commended for analysing a prospectively collected database on 1 816 patients in two institutions who underwent PN for clinical T1 renal tumours. Their primary endpoint was to investigate the impact of prolonged WIT on long-term renal function focusing on two clinical endpoints; chronic kidney disease, as estimated by an estimated GFR of <60 mL/min/1.73 m2, and major renal function deterioration defined as an increase in creatinine of >25% of the preoperative value.
Warm ischaemia time using a threshold of 30 min created two comparative groups. Patients were followed for up to 40 months after surgery. In addition to this, patients were further sub-stratified into five subgroups, critiquing the effect of WIT up to 50 min. A key feature of this paper [1] is the use of propensity score matching to adjust for any potential preoperative confounders affecting postoperative renal function, a technique also allowing matching of the two groups.
The authors correctly emphasise the direct relationship between tumour size and duration of WIT, with larger tumours requiring excision of more renal parenchyma and adding to ‘on-clamp’ time. Tumour size and renal function are vital determinants of suitability for PN [2]. This publication [1] clearly demonstrates that although large tumour size equated with prolonged clamp time, this was not the sole determinant of impaired long-term renal function.
The importance of other independent variables such as preoperative renal function, patient age and preserved renal parenchyma have been highlighted here as potentially playing a greater role than was previously appreciated.
The second and possibly more remarkable finding from this paper is that ischaemic time was not an independent predictor of ultimate renal function after PN. This contrasts with most other reports to date. Although not recommending using a WIT of up to 50 min, the results here suggest this may not be relevant to future renal function. It appears that long-term renal function after PN is primarily determined by the quantity and quality of renal parenchyma preserved, although the type and duration of ischaemia remain the most important modifiable factors, and warrant further evaluation [3].
When discussing this topic, it is interesting to refer to the initial bench work on this issue. The current approach to WIT is extrapolated from data derived from the histological changes occurring in nephrons during operative stone cases. From the data presented in this and other studies, it seems more relevant than ever to conduct clinical trials to assess this appropriately. Traditionally the time threshold for WIT is taken as 30 min, an arbitrarily placed time-point based on the above laboratory data. Beyond this value in the setting of room temperature renal ischaemia creates an array of injury centred on cellular adaptations beginning ~20 min after clamping and persisting beyond 60 min. This indicates that the traditional 30-min limit of WIT is a somewhat subjective time point and was not based on clinical outcomes.
Previous evidence suggests a 5% increase in risk for acute renal failure for every additional minute of WIT [4]. It is hard to ignore such data in exchange for this a contemporary study when so much is at stake for patient longevity. Advocators of zero-ischaemia PN have shown that those who benefit most from a zero-ischaemia technique are those with the poorest baseline renal function [5]. Most of these studies have shown that the renal functional outcomes are either equivalent or superior in zero-ischaemia cases involving small renal tumours [6].
On balance, the authors are to be credited with tackling such a controversial matter and highlighting the lack of good quality laboratory data. Clearly, factors other than WIT contribute to postoperative renal function but for now we must conclude that every minute ‘on-clamp’ does count.
References