Editorial: Predicting outcome: role of gene signatures
Pathological assessments, such as Gleason grading, which is a strong clinical predictor of prostate cancer progression [1], have a role to play in predicting the outcome of a patient’s response to therapy. The addition of PSA and TNM staging are further used to inform appropriate treatment strategies in patients who are at low, intermediate and high risk of disease progression. Unfortunately, approximately 30% of men with intermediate-risk prostate cancer will fail to be cured by surgery or radiation therapy approaches. This is not surprising as primary prostate cancer represents a complex heterogeneous disease that is clearly not fully explained by the current clinical prognostic factors, and further molecular characterization is required. There is now significant emerging evidence that the molecular characterization of tumours is important to enable us to stratify prostate cancer patients by their response to primary therapy and to identify the next appropriate steps in their treatment pathway.
Long et al. [2] have identified gene signatures that can define different genomic subtypes of prostate cancer and are predictive of biochemical recurrence. Erho et al. [3] discovered and validated a 22-gene signature, which they termed a genomic classifier for the prediction of early metastasis after radical prostatectomy, while Penny et al. [4] have identified an mRNA expression signature of Gleason grade which is predictive of lethal prostate cancer.
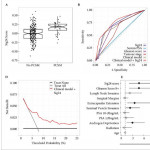
Long et al. [2] identified a 24-gene signature, which they discovered through RNA sequencing analysis of 100 formalin-fixed paraffin-embedded prostatectomy samples. They went on to validate their findings in a publically available independent gene expression microarray dataset of 140 patients. This 24-gene signature forms the basis of the present study by Pellegrini et al. [5], who refer to this gene signature as Sig24. In their study, they firstly undertook to determine if Sig24 was associated with pathological Gleason score as a marker of tumour aggressiveness, and then if it had prognostic value for the identification of patients at risk of metastasis or prostate cancer-specific mortality after radical prostatectomy. The Gleason score association study was carried out using the data from three independent case–control sets, including 182 patients from the Cleveland Clinic and two cohorts (cohort I, n = 545; cohort II, n = 235) from the Mayo Clinic, for which gene expression analysis had previously been conducted by Genome Dx using the Affymetrix Human 1.0 ST Genechip platform. The Sig24 score was calculated for each patient and higher Gleason score was associated with significantly higher Sig24 scores. The association studies for metastatic disease and prostate cancer-specific mortality, however, were only carried out in the Mayo Clinic cohort II. For both clinical endpoints the Sig24 score combined with the clinical model outperformed the clinical model alone of PSA, Gleason score and tumour stage. For metastatic disease the area under the curve for the clinical model alone was 0.69 (0.62–0.77) compared with 0.73 (0.66–0.78) for the clinical model combined with Sig24. For the prostate cancer-specific mortality endpoint, the area under the curve for the clinical model alone was 0.69 (0.67–0.87) compared with 0.74 (0.63–0.85) for the clinical model combined with Sig24.
These gene signatures have significant potential for predicting the progression of disease rather than waiting for PSA relapse, which is currently used to identify disease recurrence, with interval to biochemical failure being the best univariate factor predicting prostate cancer mortality and overall survival [6]. This would allow the initiation of additional therapies before recurrence and a better outcome for the patient. This concept has been demonstrated in a study in which the use of the Decipher gene signature was shown to improve the identification of patients who could benefit from adjuvant radiotherapy and thus only these patients were targeted for therapy [7].
Incorporating these gene signatures in robust clinical assays and integrating them into clinical decision-making is the next essential step in order for these strategies to have an impact on patient outcomes.
References