Stone disease is a highly prevalent condition that unites all countries around the world, although surgical management will depend on many factors including availability of different technologies. However, percutaneous nephrolithotomy (PCNL) remains the cornerstone for the management of larger renal stones in all parts of the world, and Rizvi et al. [1] report on a huge cohort of PCNL procedures – 3 402 to be precise from Karachi. This is a single-centre series, over an 18-year period, reporting real-life data and showing a stone clearance rate of ~80%, as assessed by plain abdominal radiograph of the kidneys, ureters and bladder, and ultrasonography (US). Whilst the definition of stone-free and imaging modality used to judge it remains a contentious issue, this paper reflects the excellence of high-volume surgery in specialist centres.
Recently, the BJUI became the affiliated journal for the International Alliance of Urolithiasis (IAU), whose annual meeting takes place in Shaoxing this month. To celebrate this, we are proud to publish a ‘Best of Urolithiasis’ issue, which features some of the top stone papers published in the BJUI over the last few years [2]. Choosing articles for this was quite a task given the quality and whilst we have attempted to recognise submissions that potentially change practice, the geographical diversity of the work shows not only the global nature of stone disease but also the excellent research that is being done worldwide and in different healthcare systems to improve care and outcomes. Of particular importance are randomised trials that are often lacking in surgical areas. One such paper from China addressed the question of US vs fluoroscopy for PCNL access during mini-PCNL [3]. Whilst the truth is that surgeons should use whatever gives the best outcomes, the authors in a very high-volume centre were able to demonstrate the effectiveness of US-only punctures, although a combination may be better in complex stone burdens. Another randomised controlled trial (RCT) of clinical importance was from the USA, where the authors conducted a good quality double-blind RCT of NSAID use before ureteric stent removal under local anaesthesia [4]. Whilst a small study, the incidence of severe pain in the 24 h after stent removal was 55% in the placebo group vs 0% in the NSAID group – as such this simple study should have changed practice for all who perform this procedure.
I hope you take the time to check out the virtual issue on urolithiasis and read the other papers I could not mention here. Please continue to send your high-quality stone papers to the BJUI and maybe your submission will feature in our next ‘Best of Urolithiasis’ issue.
Last year I introduced Publons via a BJUI Blog . It is pleasing that Wiley, the publishers of the BJUI, have now partnered with Publons to make digital archiving and verification of reviewer (and editorial) work easily accessible with a mouse click once a review is completed.
So, what is Publons again? Perhaps a brief reminder: Just as PubMed collates publications, Publons collates peer reviews you have performed and verifies you did them. With one hyperlink you may go to all of your reviews listed by date and under sections of journals. In addition, Publons also allows you to showcase to what editorial boards you belong. It also now allows editorial board work to be collated and rewarded.
I can do this all myself, can’t I? Well yes you can but this service is free and offers third party verification of peer reviews. This is important in the era of fake news. You also find out when an article you reviewed is published.
Publons is important because until now it has been difficult to track and quantify the hard work done by reviewers that is all pro bono. Getting credit for reviews is important and this website finally acknowledges that fact. Finally you can compete with other colleagues (all friendly of course). For those with editorial roles for journals the handling of manuscripts can also be collated to again get credit. A final side point is that making your reviews public is possible should you choose to do so (and gets your more points) but that is an individual (and sometimes journal) decision.
Reminder how to access and use Publons:
1) The journal may be aligned with Publons (as BJUI now is) so just click the box at time of review (see example here):
2) Simply forward your official thank-you receipt email as below to [email protected] and they will do the rest (example here):
3) I can’t find the emails- is there any way of back tracking to reviews done over the years? Yes- take screen shots of your “Official Journal Dashboard “like this de-identified one below and send to reviews@publons (I have done this and it works quite well but you may need to take more than one screen shot per page to make it more easily digestible)
4) You can ask a journal to email you a summary and provided they send enough detail Publons will look at it and probably accept it (I have not done this but heard it may work)
So there you have it. The variety of methods is straightforward. A new Publons dashboard will be created and is easy and documents well which journals you have reviewed for and when.
What are the Publons awards? We can see here in the example of Prof Henry Woo (urologist, Australia) whom has reviewed many papers (see his total score and review numbers). Publons also ranks overall reviewer status and within different reviewers topic sections. It also gives “awards” each quarter to the best reviewer overall, best from your university etc. The value of such awards is likely to rise each year as more people use the Publons platform.
Are there other benefits? Well for Editors and Publishers to be able to tap into key reviewers will be extraordinary moving forward.
So its easy and free to join and benefit from Publons and the earlier you start the easier it is to track your digital online CV. Get credit and build your online presence (it allows a photo and short biography and links to your ORCID identification) and gain a sense of accomplishment by being a peer reviewer- without whom journals would not exist. It is also quite fun to see how your colleagues are ranked (or others from your country, specialty and university) and also the ridiculous number of reviews people from different fields has done.
Nathan Lawrentschuk PhD MBBS FRACS
Associate Editor BJU International/Editor USANZ BJU International Supplement
Olá! The 37th Congress of the Société d’Urologie (SIU) was held in Lisbon, a beautiful, historic city (19th-22nd October 2017). It is the first time the congress has been held here. We were told by the co-hosts during the opening ceremony that Portugal has a history of finding new routes and building bridges to other cultures, which they hoped to emulate at the Congress. The iconic 24 de Abril Bridge, the largest in Europe, was visible from the Congress Centre serving as a visual reminder of bridges being made during this congress.
The SIU is unique as it is a truly international association with no country or continent affiliation; it has 7000 members from 130 countries and 24 directors from every continent. Therefore the congress brings urologists from all over the world together. The words “Together, United, Stronger” said during the opening ceremony resonated as the ethos of the conference; and is especially pertinent in the current worldwide political climate. Furthermore, that the educational, global and philanthropic aspects of being part of such a society was highlighted as ways we can all help each other.
SIU 2017 had an engaging scientific programme providing a valuable educational experience to attendees over the four days. It covered the breadth of urology and we were honoured to listen to such notable speakers. The navigable congress centre (as well as the congress being a smaller meeting, as compared to EAU, AUA) meant delegates could easily attend whatever took their interest. The Scientific Programme included Plenary sessions, Master Classes, debates, ‘controversies’ sessions, instructional courses, poster presentations, the SIU Nurses’ Symposium and hosted urological organisation meetings. There were also Industry supported sessions and an Exhibition Hall.
The social programme allowed relaxation and networking amongst colleagues; plus sampling local Portuguese wines, food and an insight into Portuguese culture. The opening ceremony included a Fado performance. The SIU night held at Pátio da Galé in the PraÇa do Comércio was the pinnacle of the social aspect of the conference. The refreshments were plentiful and delicious, there were gelato stands as well as enough Pastel de Nata to feed a small army! A typical brass band, ceramic station, football net and DJ kept people entertained until we were told to leave. The SIU President’s Dinner held in the Queluz Palace was an amazing night in impressive surroundings for invited guests.
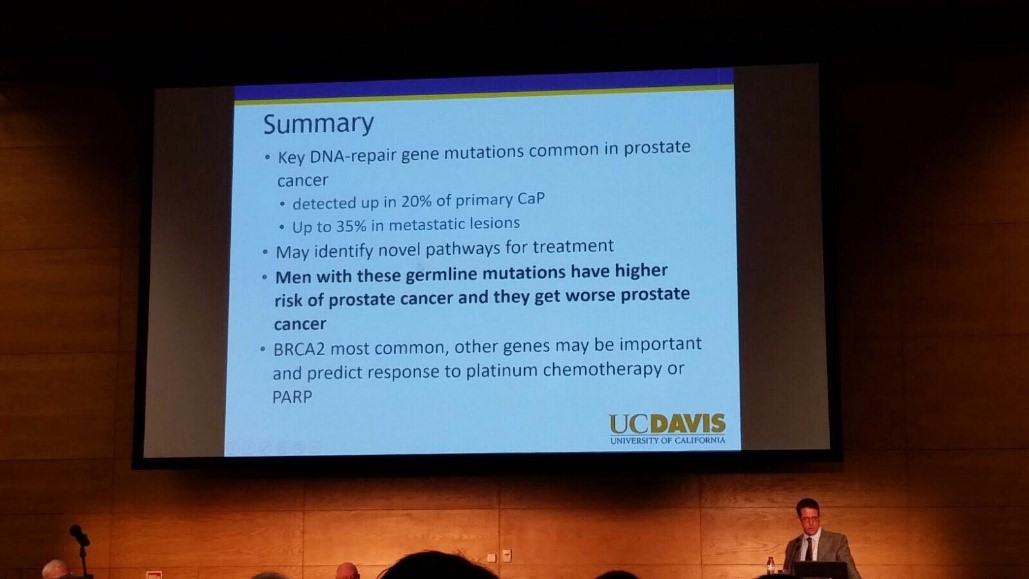
The fully attended WUOF session on the first day brought experts in the field of Urological cancers to provide their views on the changing paradigms and new treatments. All talks provided succinct, expert opinion. The presentation by Marc Dall’Era on the genetics of prostate cancer and link with the BRACA gene was particularly informative; especially as these men get worse cancer: pictured. Genetic counselling of patients diagnosed with prostate cancer may need to increase in the future. Genomics was discussed in other cancer sessions too; it’s growing availability, reducing costs and correlation with difference in outcomes between patients must surely strengthen the argument for more personalised medicine.
I also particularly enjoyed the presentation by Tony Finelli who unraveled the notion of ‘surgical outcome’ which is often used to analyse the quality of surgery; this is then used in arguments for high volume centres. He suggested instead that assessing quality needs Quality Indicators and one alone isn’t sufficient. His group in Canada used their national database to propose 32 Quality Indicators, which are valid, reliable, feasible and useable; they found that higher quality had lower mortality and morbidity. Patient centred care, patient selection, high quality surgery and recovery was a common theme in other sessions too.
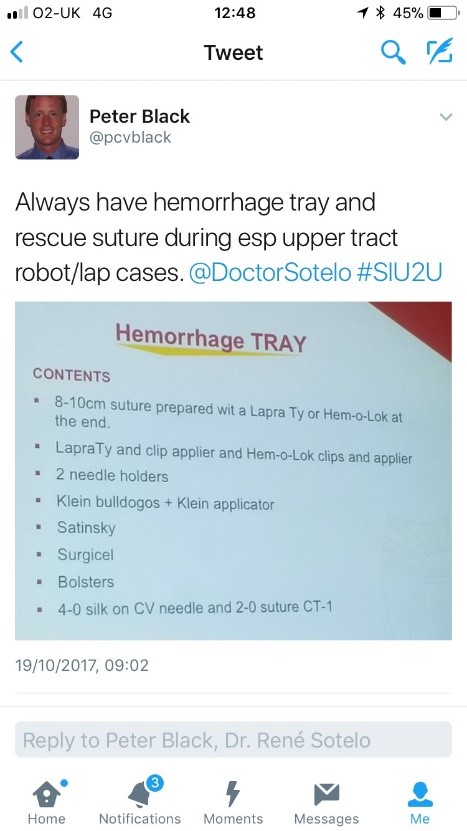
The SIU Innovators Symposium didn’t disappoint; highlights included Dr Sotelo’s presentation of ‘sticky situations’ in robotic surgery. His operative videos showed all the things you really don’t want to see whilst operating, however he and the panel provided tips in order to avoid or correct these operative mistakes. Dr Sotelo’s advice regarding having a ‘haemorrhage tray’ present was ingenious and useful: pictured. Thank you to Dr Sotelo and Dr Knudsen who shared their operative videos with us in order to provide this learning; mistakes in surgery should be shared to avoid others making the same mistakes. The symposium also invited two influential leaders, Professor Prokar Dasgupta, editor BJUI, and Professor Arnulf Stenzl to give their approach on leadership. Prof Stenzl suggested it was easier to explain how not to be a bad leader as he has learnt more from his mistakes than from successes. Prof Dasgupta suggested his leadership style was to be collaborative, trusting team members to deliver, democratic and transformative; also that he, as a leader, wanted to “help other people do well”.
SIU had a strong presence of trainees; many attending to present their academic work during the moderated poster sessions, listen to worldwide experts and of course network with others from around the world and generating future collaborations. One session ‘Sage Advice from the Wise’ was particularly aimed at trainees’ where Urological trainees met 10 experts (all wise, but certainly not old!). We were able to discuss career plans, ask questions about fellowships and talk about the advantages of academia alongside clinical practice. There was also a Residents Rapid Fire Q&A which was won by Dr Avinash Odugoudar: pictured.
Urological cancer treatment featured heavily on the programme. One particularly inspiring talk on advanced testicular cancer by one of the leading surgeons in Europe, Axel Heidenreich, really expanded our horizons of just what can be achieved operatively for patients with metastatic disease, including aortic resection and Whipple’s procedure. It proves that big, open surgery does exist in urology for the right patients; requiring expertise and courageous surgical skills but offering patients treatment despite disseminated disease. One session included debating the use of routine radiation for positive surgical margins in prostate cancer. The presentations by Dr Dall’Ezra and Dr Briganti actually came to very similar conclusions. Both wanted to avoid over treatment and championed a risk stratified approach with emphasis on patient selection; as not all those with positive margins recur. It was suggested that choosing those at greatest risk of recurrence for example the site(s) of positive margin, high Gleason score, early rise in PSA (even if remains less than 0.5) and ultra-sensitive PSA can help to stratify need for adjuvant radiotherapy; or alternatively monitor with option for salvage treatment.
Robotic assisted surgery for prostatectomy, cystectomy and nephrectomy was debated freely throughout the congress. Most quoted recent evidence that there is no clear advantage with regards to blood loss, LOS, long term outcomes and survival; but very different costs. Dr Mihir Desai argued that if you already had the robot you should encourage high volume surgery, but that departments have a responsibility to put the robot to good use; not for simple cases, but rather be reserved for difficult operations so the real advantages of robotic assisted surgery will be better appreciated. Criticism was made of RCTs not being the right research method for comparing surgical techniques as it leads to comparison of individuals not techniques. We eagerly anticipate the iROC study. An important point made regarding robotic cystectomy was that it must include intra-corporeal bladder formation, otherwise many of the advantages of the minimally invasive part are lost. Laparoscopic surgery was argued as not old fashioned; but rather an efficient and cost effective method of minimal access surgery without compromising on outcomes. However open surgery is still an option in many hospitals worldwide; a question from the audience included the dilemma faced by departments whose similar outcomes between open and laparoscopic procedures do not justify the switch to laparoscopy.
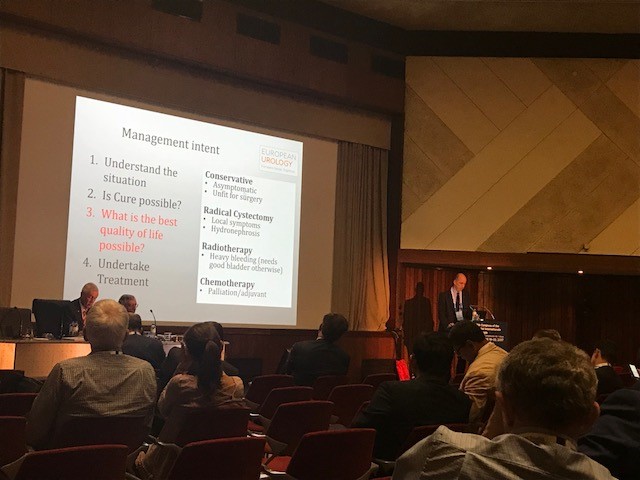
Prof Catto, editor of European Journal of urology delivered a compelling presentation of the advantages of radical cystectomy over radiotherapy for locally advanced bladder cancer. He also mentioned the importance of surgical planning and management intent: pictured. In some cases he does pre-operative MRI, however a PET scan when organised, doesn’t necessarily change his management. He also presented a plenary lecture on risk factors for upper tract TCC which confirmed smoking as the number one risk as well as occupation. However combustion occupations and amine-relate occupations show a difference in cancer aggression suggesting the biology of the cancer is different. Like others, he wanted to aim for personalised treatment of cancer with specific treatments according to genotype.
Debating the merits of surgery was a common theme in several sessions, perhaps unsurprisingly. However a particular highlight was the debate of medical vs surgical theory for lichen sclerosis (LS). The clear and compelling argument by Bradley Erickson for medical treatment rested on 10 points, which included: that LS is an inflammatory condition and these are not necessarily managed by surgery, the dermatologist and gynaecologist manage LS without surgery, LS in the urethra demonstrates squamous change which is reversible and lastly that we don’t really fully understand this disease yet.
Female urology was the first plenary session of the congress and the use of mesh unsurprisingly featured in other sessions, included one entitled ‘controversies in urology’. The clear message from Dr Badlani was to know the anatomy and not to ‘have a go’ at continence surgery, it needs expertise. He and his panel presented difficult cases including mesh seen at cystoscopy, operative video of hydro-dissection and an image of compete extrusion which led the audience to wonder if it had even been placed correctly in the first place!?
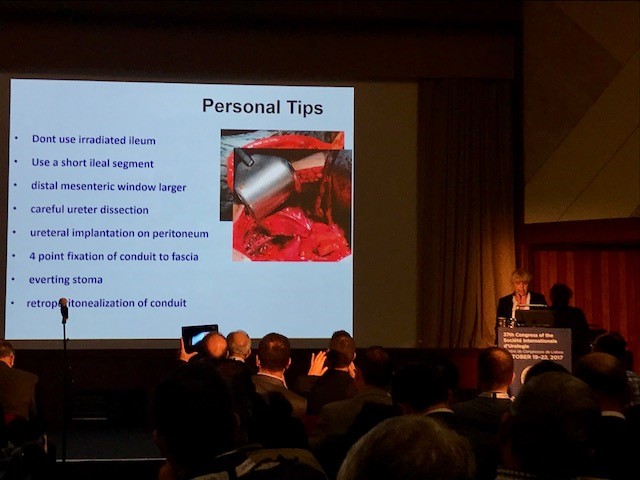
In the joint SIU-GURS meeting panel members each presented a challenging case from their experience of reconstructive surgery and ileal conduit formation; then this was discussed amongst the panel. There was an amazing X-ray of a huge stone in an ileal conduit due to stasis of urine, confirming the need to avoid long conduits. A fear held by many was early failure of the anastomosis; when debating when to re-operate, I particularly liked the phrase “three months to let the belly cool down” said with an American drawl. Margit Fisch shared her top tips of surgery: pictured. An insight into managing continence in patients with Spina Bifida was succinctly presented by Sean P. Elliot; he advised that the patients needed to be ‘proud of their stoma’ and that each needed an individual surgical plan but holistic approach.
Endourology and stone sessions were well attended and each explored different treatment modalities for stone management. Plus the congress offered masterclasses for ureteroscopic techniques, the joint SIU-Endourology session, poster sessions and a ‘controversies session’ debating URS vs Mini-perc. There was also an instructional course on lasers and flexible ureteroscopic technique. Experienced surgeons from across the globe argued for and against the role of ESWL vs RIRS vs PCNL in modern practice. Aside from patient and stone factors there was an appreciable point made of the importance of surgeon experience and available resources of the institution. Non-surgical aspects of stones were also presented, such as diet and hydration in stone disease. Advances in stone surgery, including a robotic assisted ureteroscope was particular enlightening and futuristic; however brought up the inevitable dilemma of clinical need for such technology at a time of financial restraint facing many healthcare systems.
Andrology sessions included a joint SIU-ISSM session, a master class on urethral stricture disease, video session on male reconstruction and poster session on sexual function and dysfunction. There was a debate on the role of the urologist in the management of male infertility and improving sperm. The (interesting) use of an acronym F.A.S.T was described by host urologist from Portugal Dr Pedro Vendeira: pictured. This is in relation to the follow up of non-responders to PDE-5 inhibitors, of which non responders were those who had tried these medications more than eight times. He described a 50% drop out of the use of these drugs due to cost, side effects and co-morbidities. The difficulty of treating Peyronies was discussed by Dr Moncada who confirmed the absence of the role for medical therapies, except use of PDE-5 inhibitors to strengthen erections. There was a role for ‘ penile rehabilitation’ which included a (peculiar) traction device. He presented his and the EAU indications for surgery and he stressed the importance of managing patient expectation and informed consent.
In conclusion, the SIU Congress was both informative and enjoyable. Our co-hosts promises: of warmth, friendship and the Portuguese tradition of sharing wine were delivered alongside a beneficial education programme. Those that did not attend can access abstracts and lectures online via the SIU@U platform.
SIU are also increasing their activities with the following initiatives: ‘B2B’ bench to bedside, ‘Uro-Technology’ training and ‘U-care’ a global urological research collaboration. SIU also wants to build on the opportunities for global education and global health; plus help colleagues without same level of resources.
Thank you to the SIU organisers for a successful congress! Thank you to the presenters and speakers for their expertise and dedication to academia in urology; and congratulations to all the prize winners. I’m sure the next SIU Congress 2018 in South Korea will be equally successful.
To describe the technique of robot-assisted high-extended salvage retroperitoneal and pelvic lymphadenectomy (sRPLND+PLND) for ‘node-only’ recurrent prostate cancer.
Patients and Methods
In all, 10 patients underwent robot-assisted sRPLND+PLND (09/2015–03/2016) for ‘node-only’ recurrent prostate cancer, as identified by 11C-acetate positron emission tomography/computed tomography imaging. Our anatomical template extends from bilateral renal artery/vein cranially up to Cloquet’s node caudally, completely excising lymphatic-fatty tissue from aorto-caval and iliac vascular trees; RPLND precedes PLND. Meticulous node-mapping assessed nodes at four prospectively assigned anatomical zones.
Results
The median operative time was 4.8 h, estimated blood loss 100 mL and hospital stay 1 day. No patient had an intraoperative complication, open conversion or blood transfusion. Three patients had spontaneously resolving Clavien–Dindo grade II postoperative complications. The mean (range) number of nodes excised per patient was 83 (41–132) and mean (range) number of positive nodes per patient was 23 (0–109). Seven patients (70%) had positive nodes on final pathology. Node-positive rates per anatomical level I, II, III and IV were 28%, 32%, 33% and 33%, respectively. In patients with positive nodes, the median PSA level had decreased by 83% at the 2-month follow-up.
Conclusion
The initial series of robot-assisted sRPLND+PLND is presented, wherein we duplicate open surgery with superior nodal counts and decreased morbidity. Robot-assisted technical details for an anatomical LND template up to the renal vessels are presented. Longer follow-up is necessary to assess oncological outcomes.
It’s hard to believe that we have been doing the BJUI Social Media Awards for five years now! I recall vividly our inaugural BJUI Social Media Awards in 2013, as the burgeoning social media community in urology gathered in the back of an Irish Bar in San Diego to celebrate all things social. At that time, many of us had only got to know each other through Twitter, and it was certainly fun going around the room putting faces with twitter handles for the first time. That spirit continues today as the “uro-twitterati” continues to grow, and the BJUI Awards, (or the “Cult” Awards as our Editor-in-Chief likes to call them), remains a fun annual focus for the social-active urology community to meet up in person.
As you may know, we alternate the Awards between the annual congresses of the American Urological Association (AUA) and of the European Association of Urology (EAU). Last year, we descended on Munich, Germany to join the 13,000 or so other delegates attending the EAU Annual Meeting and to enjoy all the wonderful Bavarian hospitality on offer. This year, we set sail for the #AUA17 Annual Congress in Boston, MA, along with over 16,000 delegates from 100 different countries. What a great few days in beautiful Boston and a most welcome return for the AUA to this historic city. Hopefully it will have a regular spot on the calendar, especially with the welcome dumping of Anaheim and Orlando as venues for the Annual Meeting.
Awards
On therefore to the Awards. These took place on Saturday 13th May 2017 in the City Bar of the Westin Waterfront Boston. Over 80 of the most prominent uro-twitterati from all over the world turned up to enjoy the hospitality of the BJUI and to hear who would be recognised in the 2017 BJUI Social Media Awards. We actually had to shut the doors when we reached capacity so apologies to those who couldn’t get in! Individuals and organisations were recognised across 12 categories including the top gong, TheBJUI Social Media Award 2017, awarded to an individual, organization, innovation or initiative who has made an outstanding contribution to social media in urology in the preceding year. The 2013 Award was won by the outstanding Urology Match portal, followed in 2014 by Dr Stacy Loeb for her outstanding individual contributions, and in 2015 by the #UroJC twitter-based journal club. Last year’s award went to the #ilooklikeaurologist social media campaign which we continue to promote.
This year our Awards Committee consisted of members of the BJUI Editorial Board – Declan Murphy, Prokar Dasgupta, Matt Bultitude, Stacy Loeb, John Davis, as well as BJUI Managing Editor Scott Millar whose team in London (Max and Clare) drive the content across our social platforms. The Committee reviewed a huge range of materials and activity before reaching their final conclusions.
The full list of winners is as follows:
Most Read Blog@BJUI – “The optimal treatment of patients with localized prostate cancer: the debate rages on”. Dr Chris Wallis, Toronto, Canada
Most Commented Blog@BJUI – “It’s not about the machine, stupid”. Dr Declan Murphy, Melbourne, Australia
Most Social Paper – “Novel use of Twitter to disseminate and evaluate adherence to clinical guidelines by the European Association of Urology”. Accepted by Stacy Loeb on behalf of herself and her colleagues.
Best BJUI Tube Video – “Combined mpMRI Fusion and Systematic Biopsies Predict the Final Tumour Grading after Radical Prostatectomy”. Dr Angela Borkowetz, Dresden, Germany
Best Urology Conference for Social Media – #USANZ17 – The Annual Scientific Meeting of the Urological Association of Australia & New Zealand (USANZ) 2017. Accepted by Dr Peter Heathcote, Brisbane, Australia. President of USANZ.
Best Urology App – The EAU Guidelines App. Accepted by Dr Maria Ribal, Barcelona, Spain, on behalf of the EAU.
Innovation Award – BJUI Urology Ontology Hashtags keywords. Accepted by Dr Matthew Bultitude, London, UK, on behalf of the BJUI.
#UroJC Award – Dr Brian Stork, Michigan, USA. Accepted by Dr Henry Woo of Brian’s behalf.
Most Social Trainee – Dr Chris Wallis, Toronto, Canada
Best Urology Journal for Social Media –Journal of Urology/Urology Practice. Accepted by Dr Angie Smith, Chapel Hill, USA, on behalf of the AUA Publications Committee.
Best Urology Organisation – Canadian Urological Association. Accepted by Dr Mike Leveridge, Vice-President of Communications for CUA.
The BJUI Social Media Award 2017 – The Urology Green List, accepted by Dr Henry Woo, Sydney, Australia.
All the Award winners (except Dr Brian Stork who had to get home to work), were present to collect their awards themselves. A wonderful spread of socially-active urology folk from all over the world, pictured here with BJUI Editor-in-Chief, Prokar Dasgupta.
A special thanks to our outstanding BJUI team at BJUI in London, Scott Millar, Max Cobb and Clare Dunne, who manage our social media and website activity as well as the day-to-day running of our busy journal.
See you all in Copenhagen for #EUA18 where we will present the 6th BJUI Social Media Awards ceremony!
Declan Murphy
Peter MacCallum Cancer Centre, Melbourne, Australia
Major foci for clinically oriented specialty journals are systematic reviews and meta-analyses. Systematic reviews have a preeminent role in guiding the practice of evidence medicine by addressing focused clinical questions in a systematic, transparent and reproducible manner. Defining criteria of a high-quality systematic review include: an a priori registered protocol, a comprehensive search of multiple sources including unpublished studies (to avoid publication bias), an assessment of the quality of evidence that goes beyond study design alone, and a thoughtful interpretation of the findings. Systematic reviews inform clinicians and patients at the point of care, form the foundation of evidence-based clinical practice guidelines, and help shape health policy [3]. They also find frequent citation and can raise a journal’s impact factor. There is therefore more than one good reason for journals to care about the quality of systematic reviews.
The authors [4] surveyed four major urological journals and compared the periods 2013–2015 to 2009–2012 and 1998–2008. Despite a dramatic increase in the number of systematic reviews published each year, methodological quality has stagnated with mean AMSTAR scores ± standard deviations of 4.8 ± 2.4 (2013–2015; n =125), 5.4 ± 2.3 (2009–2012; n =113) and 4.8 ± 2.0 (1998–2008; n =57). The average systematic review therefore has deficits in over half the 11 AMSTAR criteria and is of only modest quality thereby undermining our confidence in their results. Although the mean AMSTAR score of 5.6 ± 2.9 for 25 systematic reviews published in the BJUI in 2013–2015 compared favourably to similar studies in other leading urology journals, the difference was not statistically significant.
What are we going to do about it? Inspired by these findings, the BJUI is launching a new initiative to raise awareness for the issue of methodological quality of systematic reviews among its readership and raise the bars for its contributors. Future systematic review authors will be asked to submit an AMSTAR-based checklist to provide enhanced transparency about its methods that will be reviewed as part of the editorial review process. These include documentation of an a priori written protocol and ideally, registration of the systematic review through the Cochrane Collaboration or the Prospective Register of Systematic Reviews (PROSPERO). Such a protocol should outline all important steps of the review process including the definition of outcomes, study inclusion and exclusion criteria, details about the literature search, study selection and data abstraction process, analytical approach including planned sensitivity and subgroup analyses. Authors should also rate the quality of evidence looking beyond study limitation alone by using an approach such as the Grading of Recommendations Assessment, Development, and Evaluation (GRADE), which recognises such additional domains such as imprecision, inconsistency, indirectness and publication bias [6]. Critical steps of the systematic review process should be completed in duplicate to guard against random and systematic error and authors should provide readers with the information about who funded the studies included in the review, as well as their own potential conflicts of interests. To guard against publication bias, systematic review authors should also search for ongoing trials and unpublished studies through registries and abstract proceedings.
It is understood that the methodological handiwork that goes into the planning, execution and reporting of a systematic review do not assure clinical relevance or newsworthiness, nor does it address any issues surrounding the limited quality of studies that the review may be summarising. However, it is nevertheless a sine quae no to assure readers that they can be confident of the results. The new BJUI initiative will raise awareness for the issue of systematic review quality by providing a summary AMSTAR score to accompany each article. We hope that with this initiative we will provide a beacon for other specialty journals to follow, with the goal of raising the bar for all published systematic reviews and ultimately leading to improved patient care.
The articles beneath headlines in the media relating to medicine rarely contain anything truly revolutionary or even anything particularly new despite what the headlines might have suggested. We have all seen headlines promising a new cure for cancer, condemning an individuals practice and suggesting they are a charlatan and articles suggesting doctors are under-treating patients and depriving them of life changing care or over-treating patients and wasting and misusing limited resources. More often than not the hyperbole of the headlines fail to truly represent the truth. What is claimed to be new turns out to be old news, cures for cancer never show the results that were promised, and the extremes of over or under treatment are never quite as extreme as suggested.
A week or two ago we have seen the newspapers filled with headlines about a list of 40 treatments or tests that form part of current practice that are deemed unnecessary. This list was originated from the ChoosingWisely group, an American group now established in the UK. This organisation encourages both patients and clinicians to question what they are doing and whether certain processes or interventions are wise, necessary and appropriate resource efficient.
Much of the recommendations on these lists in these sites are undoubtedly true and worth looking at to make sure your practice is mainstream although much of the advice is old and well established. The AUA has 10 recommendations on the US based Choosingwisely.org website the vast majority of which are simply current practice (don’t do a bone scan in men with low risk prostate cancer), however one or two make me feel uncomfortable and one or two differ on the UK and US websites.
The recent headlines were predictable – ‘40 common treatments and tests that doctors say aren’t necessary‘ & ‘Senior doctors condemn 40 treatments and tests as being of little or no use‘. Among the advice that reached the headlines obtained from the UK site (choosingwisely.co.uk) was the statement ‘Unless a patient is at risk of prostate cancer because of race or family history, PSA based screening does not lead to a longer life’. The UK site has also commented on the use of chemotherapy in ‘advanced’ cancer saying it may not be appropriate – also evidently true. The US site includes the recommendation that creatinine is not measured in men with benign prostate disease and minor lower urinary tract symptoms.
One particular problem with these public health, committee lead recommendations and advice is that treating populations is easy. Populations don’t sue public organisations, individual patients sue individual practitioners and therein lies the nub. What may be right as an idea – not measuring creatinine in men with low grade LUTS – is fine until the chap who has significant renal impairment walks in to your clinic and asks you why you didn’t measure his creatinine when he saw you a year ago. Not measuring a PSA seems fine until the patient with missed prostate cancer reappears and suggests he asked you about testing his PSA, but as he had no family history and wasn’t black you told him it wasn’t necessary; you showed him a website and explained to him we’d be wasting resources if you tested his PSA. He may not understand that the delay may not have impacted on his survival. Patients don’t hear that if they perceive there has been a delay in establishing a diagnosis.
Treating individuals, caring for the person across the table from you is very different from making pronouncements about populations. It’s easy to recommend that chemotherapy is not used, until you are the one being offered a chance, if only small, of being offered some hope and a chance of survival.
I recognise that resources are not endless and that it is right for clinicians and healthcare workers in all sectors to think about how resources are used. The problem however is that the user of healthcare resource – the patient – wants their care to be lowest risk, independent of cost, and increasingly they are resorting to using legal channels if they perceive that care has been anything other than perfect.
Of the men on those panels not recommending use of PSA, I wonder how many of them would refuse to have it checked, or indeed would refuse chemotherapy if it was their only, if slim, hope?