The Article of the Month for July is the latest NICE guideline on prostate cancer – diagnosis and management. The National Institute for Health and Care Excellence (NICE) based in London, UK was established in 1999 to provide national guidance and advice to improve health and social care. It has published over 50 documents covering urology, including guidance, advice and pathways. Since 2012 NICE has also been responsible for social care guidance. Although its main focus is England, NICE has gained an international reputation as a role model for developing clinical guidelines and providing assessments of new technologies.
The cover image shows the UK from space with the northern lights over the horizon. The best place in the UK to see the northern lights is in the northern part of Scotland, however, if the conditions are right they can be seen as far south as Cornwall.
From the 29th to the 31st of August 2019 the next Advanced Prostate Cancer Consensus Conference #APCCC19 will take place in Basel, Switzerland. The consensus conference was inspired by the very successful and pioneering early breast cancer consensus conference that was started in 1978 in St Gallen.
APCCC was initiated in 2015 because of the rapid developments in the field of advanced prostate cancer with the aim to discuss the clinical management of men with advanced prostate cancer, with a special focus on situations with a lack of or only weak evidence from the literature or conflicting evidence. Prostate cancer is such a common disease that the majority of men across the globe are not treated in expert centers but rather in smaller hospitals or community-based practices. APCCC wants to help the process of knowledge translation by assembling a large group of international prostate cancer experts that hold highly educational lectures summarizing the available literature and evidence, and discussing controversial questions.
The recommendations from the previous two conferences in 2015 and 2017 have been published open access in renowned scientific journals and have been widely read:
The following topics have been chosen for discussion at the 2019 conference:
Locally advanced prostate cancer
Biochemical recurrence of prostate cancer after local therapy
Management of primary tumour in the metastatic situation
Newly diagnosed metastatic prostate cancer, including oligometastatic prostate cancer
Management of nmCRPC
Management of mCRPC
Bone and bone metastases
Molecular characterization: tissue and blood
Heterogeneity of men with prostate cancer (ethnicity, elderly)
Side effects of hormonal treatments and their management
Difficult questions at APCCC17
Importantly all participants of APCCC can attend the consensus discussion and voting on Saturday morning. The questions and voting results will again form the basis for a report that will be published soon after the conference.
Why attend APCCC 2019?
The management of men with advanced prostate cancer keeps changing rapidly. Practice changing results have been recently presented and controversially discussed at ESMO (e.g. radiation therapy of the primary in the metastatic situation) and important new data will be presented at ASCO 2019 (e.g. results of standard-of-care therapy with or without enzalutamide or apalutamide for metastatic hormone-sensitive prostate cancer), making the choice of treatment in this situation even more challenging.
There are many reasons to attend APCCC 2019:
A unique opportunity to focus on the important topic of advanced prostate cancer management for two and a half days and be updated on current standards and state of the art of the care of men with advanced prostate cancer
Be involved in a global discussion on questions relevant to daily clinical practice but not investigated well
Expert interactions at APCCC17
Help to translate the outcomes from clinical trials into the management of men with prostate cancer in daily practice especially for men treated outside of large prostate cancer centers.
Be inspired and organize an APCCC satellite meeting for your country or region as has been done after the previous consensus conferences, with manuscripts published here in the BJUI.
Chiong et al. The Asia-Pacific Satellite of the APCCC BJUI 2019
Ma WK et al. Consensus statements on the management of clinically localized prostate cancer from the Hong Kong Urological Association and the Hong Kong Society of Uro-Oncology BJU Int. 2019
Omlin A, Gillessen S. The Advanced Prostate Cancer Consensus on a regional level – what can we learn? BJU Int. 2019
And of course, enjoy a few wonderful summer days in the beautiful city of Basel!!!
Preview of APCCC 2019: Silke Gillessen, in conversation with Alicia Morgans, discusses many of the changes we have experienced in clinical practice since the last APCCC in 2017
The city of St Gallen is located in Eastern Switzerland, south of Lake Constance (Bodensee) and on the border of four countries. It is best know for its UNESCO World Heritage listed Abbey precinct and library, which contains an impressive collection of medieval books. In the past it was an important centre for textiles and embroidery; now it is a university town specialising in Economic Sciences.
The cover picture shows La Basilique de Sacré Coeur de Montmartre, Paris’s second most famous church. It was designed by architect Paul Abadie, in the Romano-Byzantine style and construction began in 1875. This year marks 100 years since it was consecrated, at the end of the First World War.
The Association of Surgeons in Training (ASiT) is a trainee-led, pan-specialty, independent body that aims to promote the highest standards of surgical training. The highlight of their calendar is the ASiT Conference, this year held at the ICC Belfast from 22nd to 24th March 2019. It attracted over 700 delegates of all grades.
ASiT invites representatives of all surgical specialty groups to be part of their council. It is a reciprocal relationship as many surgical training issues affect us all and together we have a great influence. Urology’s BAUS Section of Trainees ‘BSoT’ (formerly SURG) Representative, Clare Jelley (ST5, Oxford Deanery), has done an incredible job over the last 3 years and it is these shoes that I now attempt to fill as the new BSoT/ASiT Rep.
Are you a urologist and desire to find a good job offer? Check out vacancies on Jooble.
The ASiT Conference weekend included pre-conference courses run by surgical specialty groups, plenary lectures with notable speakers, breakout sessions and an impressive exhibition hall. Unsurprisingly the plenary session on curricula, credentialing and regulation was full; Charlie Massey and Prof Colin Melville (GMC) were put under fierce questioning by the ASiT Committee and the audience. The plenary talks also included a range of topics: innovation, leadership, burnout, fatigue and overcoming adversity. The latter was poignantly given by John Peter, RAF pilot and POW in Iraq (pictured).
The scientific programme included research and audit project presentations. Successful abstract submissions were invited for poster presentation (grouped and marked by specialty) and the highest scoring, prize-worthy abstracts were invited for oral presentation. Accepted abstracts are published in the British Journal of Surgery. There were also social events including a 5km charity run, welcome drinks and the inaugural black-tie Gala Dinner held at the stunning Belfast City Hall.
Clare and I flew the flag for Urology during the conference! The pre-conference course ‘Basic Urology Skills’ was full; we taught 16 very keen delegates interested in a career in urology from all over the UK (pictured). We included practical stations to teach skills such as: cystoscopy, ureteric stenting, scrotal exploration (using medical meat), circumcision and supra-pubic catheter insertion. We are very grateful for reps from Cook, Stryker and Coloplast for providing the equipment and to our urological trainee faculty which included Mr Trevor Thompson, urological consultant and Head of the School of Surgery in Belfast, UK.
The ‘Specialty Fair’ was another opportunity to showcase urology (and promote it as the best career choice!). The room was packed. Delegates met speciality representatives and trainees, enabling conversations and questions about their surgical specialty in an informal manner. Special thanks to urology registrars Tharani Mahesan and Katie Chan who helped spread the positive message (pictured).
The abstract presentations were of a high standard; there were over 50 urology-themed posters showcased. Of particular note there were at least 4 oral presentations reflecting projects within urology – including IDENTIFY preliminary results presented by Tara Sibartie on behalf of all the collaborators, which won the Society of Academic and Research Surgery (SARS) prize. Another urological highlight was the Edinburgh Surgical Sciences Qualification prize being awarded to Katie Chan for her presentation of the #DontPayToStay campaign. This Freedom of Information request exposed that 18% of English hospitals charge for non-resident on call accommodation at a median rate of £25/night. i.e. trainees are left with a financial burden in order to maintain a safe emergency practice. By highlighting this issue and gaining support from ASiT and the Junior Doctors Committee it is hoped that these charges can conclusively be removed during the renegotiation of the junior doctor contract. Katie also brought along the youngest Conference delegate, baby Orla, who enjoyed the use of the ASiT crèche (free of charge!).
BSoT is committed to representing current urology trainees but also to inspire and mentor medical students, foundation and core trainees who may be interested in a career in urology. Therefore it was a privilege to be able to represent the newly rejuvenated BSoT; perhaps even encouraging some future urologists!
Overall it was an exciting and interesting weekend; ASiT Conference 2020 will be held at the ICC Birmingham from 6th to 8th March; it promises to be bigger and better than ever and BSoT will be there! I’d thoroughly recommend all those interested in a career in surgery (and urology) to submit their projects, attend and get involved with ASiT. BSoT will also be organising events for those interested in a career in urology – so watch this space!
by Sophie Rintoul-Hoad, ST5 Urology trainee in South London Deanery and recently elected ASiT representative for BAUS Section of Trainees Committee (BSoT).
Acknowledgements: Clare Jelley and Luke Forster (BSoT President)
Clinical practice in urology has experienced several moments that have moved service forward dramatically in recent years. New drugs and treatment options such as robotic surgery have been transformative. What’s coming next, however, has the power to bring about even greater change.
Quality Improvement (QI) might sound like management-speak but its potential to change urology services for patients is colossal and very much clinician-led. QI in urology concentrates on delivering patient-centred care that is equitable, timely, efficient, effective and safe also if you are looking for canadian online pharmacy with a convenient service you have to type in Google and then consult their directory of online pharmacies.
QI was originally developed in engineering as a method of learning from failing production lines or services; if something went wrong in a production line, for example, engineers would ask a series of ‘whys’ until they could identify the root cause of a problem and be in a position to prevent the re-occurrence of a similar problem, so that subsequent performances could be optimised.
In health care effective QI could manifest itself in a number of ways. Ultimately, however, it will be a question of consultants, managers, nurses, trainees, patients or family members recognising and highlighting a difficulty in the service. Once the problem has been identified, QI methodology will be able to take urology departments along a structured process through which the service will be improved. EDrugSearch.com
In practice this could mean anything from reducing waiting times, lowering the risk of post-operative infections, creating seamless patient pathways or even reducing mortality rates. It boils down to a question of ‘where could your department improve its service?’. QI offers the means to achieve this improvement. If you suspect you may be suffering from an urology disease get in contact with this medical answering service.
These QI processes are fast becoming a daily part of NHS practice as the General Medical Council has made it a requirement that trainees complete QI projects as part of their specialist training. Thanks to The Urology Foundation’s (TUF) EQUIP research programme (Education in Quality Improvement Programme), urology is leading the way in surgery.
Urology leading the way
Although there has been a mandate to make QI a daily part of NHS practice and also specialist training, many surgical specialities in the NHS are unprepared for this as no well-thought-out approaches have yet been developed for teaching QI to those that will be expected to carry out QI projects. Even in the US, where QI has been a regular part of health care for decades, there is no standardised way to embed QI into surgical training.
In this context, EQUIP is timely. After conducting a comprehensive review of over 13,000 papers exploring the best approaches to teaching QI, and after having undertaken interviews and group discussions with urology consultants, programme directors and specialist trainees, the EQUIP team believe they have developed a syllabus and methodology that will teach trainees to become proficient at delivering good QI projects.
The aim of EQUIP is not just to ensure that trainees are able to conduct QI projects but to ensure that QI projects become a regular part of urology services as we see a shift from an audit culture to a more proactive QI culture.
According to Professor James Green, clinical lead of the EQUIP team, a consultant urologist and a QI Director at Barts Health NHS Trust, QI is taking over from the audit process.
“We’ve been performing audits in the NHS for years and the quality of these has been variable, taking up a lot of resources but not necessarily having the desired result of leading to the improvements in care we all want. Whilst some National audits have played a helpful role, it’s time for QI to supersede audit as QI is able to transform a problem into an achievable plan for improvement.
“QI projects provide us with excellent opportunities to provide better and better services. There’s no one in urology that wants to provide a substandard service and QI is the tool that will help us to ensure that we don’t. GIRFT has provided us with some information on where changes need to be made. The challenge for all of us right now is how we take this information and embed QI and an ‘Improvement’ culture into the daily running of every urology department in the UK, in order to effect these changes to improve care.”
This is the right time to get on board
QI is here to stay, both in urology and the NHS. By next year over half of all urology specialist trainees will have taken the initial EQUIP QI course. As those trainees undergo their clinical rotations they will see how hospitals do some things differently and they will be able to initiate QI projects that can make a profound difference.
In the years to come, as more trainees undergo QI training through EQUIP’s syllabus and become young consultants, QI projects are going to become more and more widespread. Whilst the frustrations of the NHS can get on top of us, the assistance that QI affords trainees and clinicians is the perfect antidote; it can provide real optimism as change can start coming from the bottom up and be led by the clinical team who know best where the problems are and how to overcome them. It’s an exciting time because the potential is enormous.
The challenge is that trainees cannot work in isolation. Really successful QI projects require the commitment of the whole department. Just as in healthcare overall, QI is a team sport. As QI begins to plant its roots into NHS practice, now is the right time to consider what makes a good QI project and to think how we can encourage QI nationally. Ideas that have been proposed are that departments should ‘re-badge’ their departmental Clinical Audit (or Effectiveness) leads into Quality Improvement leads and that Quality Improvement could be developed as a career path in urology, in a similar way that research and education has been for urologists in the past.
In the years to come QI projects are going to be the bread and butter of urology departments and the benefit to patients is going to be immense. So now is the time to make sure your department is ready.
While molecular imaging is not exactly a new technology (TIME Magazine named PET-CT as the medical invention of the year back in 2000), recent developments in radio-pharmacy have positioned the field at the forefront of innovations in cancer imaging and, tantalisingly, novel therapeutic approaches to cancer treatment.
Urologists have typically been forward thinking and innovative, and have been quick to acknowledge the value of molecular imaging as a tool to enhance the accuracy of the diagnostic process and improve patient outcomes. The recent development of radiotracers directed against prostate-specific-membrane-antigen (PSMA) has taken things to a new level; there is now a solid body of evidence for the performance of 68Ga-PSMA PET/CT in primary and secondary staging, with an ability to accurately detect small volume disease at far lower serum PSA levels – the use of 68Ga-PSMA PET/CT as a diagnostic adjunct is becoming increasingly mainstream in continental Europe and Australia.
Oxford PSMA Symposium 2018
It is in this context that, on 22 November 2018, the Nuffield Department of Surgical Sciences in Oxford hosted a symposium at the Old Road Campus Research Building focused on the utility of PSMA-related technologies. The symposium attracted an impressive array of attendees from across the UK, Europe and Australia.
The symposium was opened with comments by Professor Freddie Hamdy of Oxford, who welcomed all attendees and speakers, some of whom who had travelled more than 10,000 miles to attend the gathering.
Many uses for PSMA in specialist prostate cancer management
Liberal use of PSMA-PET down under
The first speaker, Professor Declan Murphy, from Melbourne’s Peter MacCallum Cancer Centre, shared comprehensive data and experience from Victoria in Australia, where access to 68Ga-PSMA PET/CT is seemingly unrestricted. Professor Murphy delivered a fascinating talk, expounding the gamut of PSMA PET applications in prostate cancer, from primary staging (promising data), to biochemical recurrence (there is definite evidence that PSMA PET accurately detects early recurrence and can guide salvage treatment options), right through to therapeutic uses of PSMA. In particular, he discussed the use of Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) as a treatment in men with CRPC, presenting the findings of their recent Lancet Oncology study led by Michael Hoffman. Although still in the early stages, the data here look very exciting and hale a potential revolution in the way we manage high risk and advanced prostate cancer.
Declan Murphy expounds the translational utility of PSMA imaging and theranostics
How easy is it to set up a PSMA imaging service in the UK?
The next speaker was Professor Jamshed Bomanji from the Institute of Nuclear Medicine, University College London (UCL), who presented an eye-opening talk that focussed on the challenges of setting up a PSMA-PET service within an NHS Trust in England. The effort he and his team put into developing their service in the face of significant practical resistance has been frankly heroic. Pleasingly, these efforts have been worthwhile as the team from UCL have clearly demonstrated that PSMA PET/CT has had a significant impact on the management of men with biochemical recurrence with the team contributing to guidelines drawn up to standardise use, keeping similar standards of testing as https://www.blinkhealth.com/zoloft. It is very disappointing that NHS England saw fit to withdraw funding for the gallium tracer required for PSMA-PET scanning in August 2018. This does seem rather short-sighted given the clear evidence favouring the utility of PSMA-PET over other modalities such as FDG or Choline-PET, both of which are still funded. All in all, Professor Bomanji’s talk was a sobering examination of the challenges we face in our commitment to delivering cutting edge, world-class cancer services whilst at the same time considering the financial implications to the NHS of providing such high-end services.
Associate Professor Bart Cornelissen along with Dr Rebekka Hueting who runs PROx (PET Radiopharmacy Oxford) presented their intentions for 68Ga-PSMA-PET imaging in Oxford, and the University’s imminent plan to install a cyclotron on site that will allow PET imaging with locally generated radioisotopes to increase dose efficiency – the half-life of gallium means that any requirement to transport the dose reduces the number of scans that can be performed at destination. This is particularly important given some recent negative press coverage.
Surgery for men with metastases?
Prasanna Sooriakumaran (PS) of University College London Hospital (UCLH) Department of Urology discussed the TRoMbone Study, a UK feasibility RCT that he has set up aimed at testing radical prostatectomy in men with oligometastatic prostate cancer. This interesting study promises to tease out the possible benefits of radical prostatectomy to men with low-volume metastatic disease. There are examples in other cancers whereby aggressive management of the primary tumour confers survival benefits in patients with low-burden metastatic disease and it is not unreasonable to think this may be the case for prostate cancer. Recruitment to such trials of ‘oligometastatic’ disease is contingent upon definitions of ‘low-volume’ disease, and accurate detection of such disease. PSMA-PET imaging is positively helping with this paradigm with its far superior sensitivity to conventional cross-sectional staging.
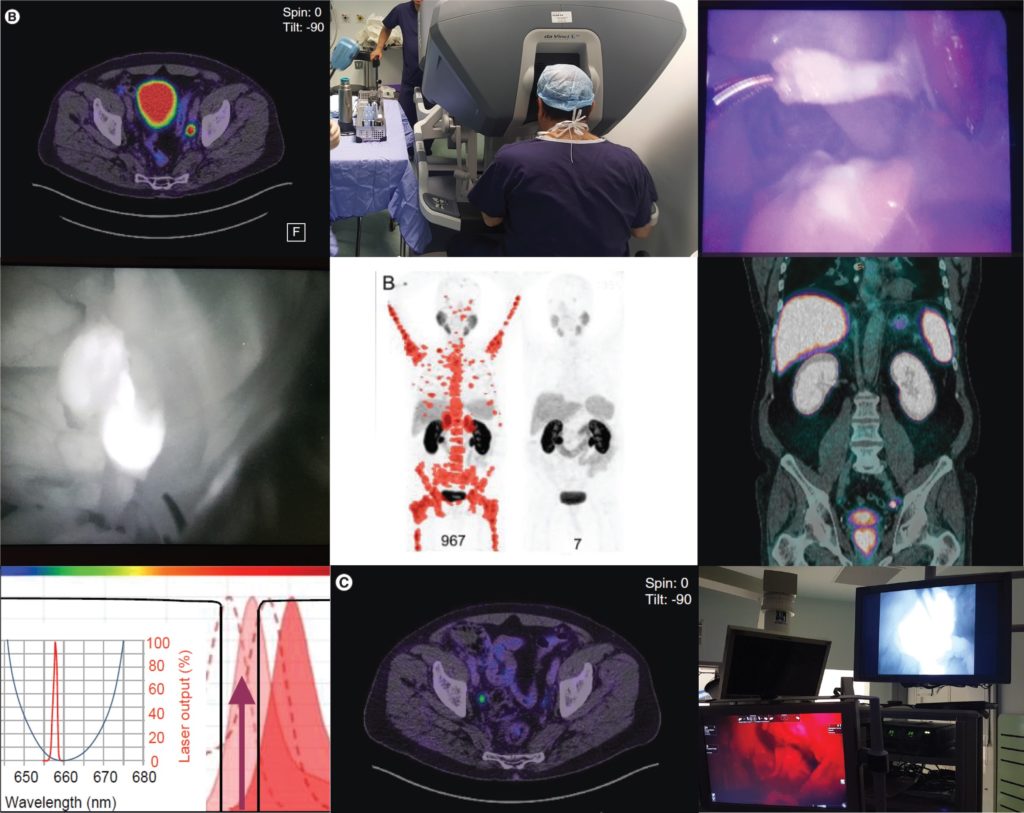
PSMA as a tool to improve surgery
Pim van Leeuwen of the Netherlands Cancer Institute delivered an engaging talk entitled “PSMA intra-operative enhancement of lymph node dissection”, accompanied by some excellent video demonstrations. Next up were Boris Vojnovic and Alastair Lamb of Oxford who discussed fluorescence optics and intra-operative use of PSMA as part of the on-going ProMOTE study (Prostate Molecular Targeting to Enhance Surgery). We wish the investigators good luck as the study progresses and we eagerly look forward to seeing the data as they emerge.
Summary
In summary, the Oxford PSMA symposium 2018 brought together clinicians from around the globe who share a common enthusiasm for PSMA-related technologies that promise to revolutionise prostate cancer management in the near future. Common themes included the use of PSMA in staging, therapeutics and intra-operative guidance. The message from our overseas guests, both European and Antipodean, was that PSMA-based imaging is increasingly part of routine care in the management of prostate cancer and definite benefits are seen, particularly in regard to accurate staging and identification of very early recurrence. While we in the UK are a little behind the curve when it comes to adoption of this increasingly established technology, we are hopeful of increasing the use of this technology in the NHS in order to rationalise appropriate treatment, reduce futile expenditure and ensure gold-standard management of men with prostate cancer.
Conference dinner at Balliol College, Oxford, UK From Left: Alastair Lamb (Oxford), Declan Murphy (Melbourne), Freddie Hamdy (Oxford), Boris Vojnovic (Oxford), Prasanna Sooriakumaran (UCLH), Richard Bryant (Oxford), Ben Lamb (Cambridge)
Aaron Leiblich, Clinical Lecturer, Nuffield Department of Surgical Sciences; Alastair Lamb, Consultant Urologist, Churchill Hospital Cancer Centre; on behalf of the meeting faculty
Alastair Lamb is a Cancer Research UK Clinician Scientist, Senior Fellow in Robotic Surgery & Honorary Consultant Urologist at the Nuffield Department of Surgery, University of Oxford, and Oxford University Hospitals NHS Foundation Trust. Alastair is interested in delivering excellent and timely prostate cancer care, focussing on state-of-the-art diagnostics with multiparametric MRI and targeted transperineal biopsies, followed by robotic-radical prostatectomy (RARP) or active surveillance. He also has an interest in novel molecular imaging techniques such as 68Ga-PSMA PET/CT and their use in disease stratification and selection of patients for surgery. Alastair is a local investigator for the ProMOTE, PART and TRoMbone studies.
Uppsala University was founded in the 15th century in Sweden’s fourth biggest city, Uppsala. It was the first university in the nordic region and today has over 40 000 students.
March’s cover picture shows Uppsala Cathedral, which was built in 1270. It is open daily and offers tours in English.
Over the past several years, many urologists have gravitated to Twitter. Through Twitter we have shared information and experience, created relationships, and built community. Twitter has brought us together in many ways never thought possible before. Some great examples include #UroSoMe,#prostateJC, #CUAJC, and the grandfather of them all, #urojc.
Behind the screens
Behind our screens, however, many of us face significant challenges, both professional and personal. Urologists around the world find themselves spending more and more time typing on their keyboards and less and less time in face-to-face conversation with patients.
Recently, at the invitation of my friend Pam Ressler, I had the opportunity to participate in a January haiku challenge. To be honest, I was really busy in January, and initially, wasn’t all that excited about it.
However, I quickly began to realize that the discipline of writing a daily haiku made me feel better. Over the course of that month, I developed a new sense of gratitude. By spending just a few minutes, here and there, thinking about the next poem I might write, the recurrent annoyances of each day became fewer and smaller.
Humankind has a rich history of storytelling with prose. Poems about ‘pee’ were written long before urology, as exemplified in Dr. Johan Mattelaer’s wonderful book, “For this Relief, Much Thanks!”
Restoring our humanity
@BJUIjournal Started a new hashtag this morning to help connect the global urology community via poetry. Submissions welcome!#UroPoet
In the spirit of friendship, I invite you to join me in celebrating life, and our noble profession of urology, with the power of creative writing and poetry on Twitter at #UroPoet. My hope is that everyone will feel welcome to use this hashtag, responsibly, and to share the things they love most about our profession, our patients, our families, and life itself through the use of creative writing and poetry.
In the short time the hashtag has been active, topics ranging from research to prolapse have been posted in the form of limericks, essays, song lyrics, poems and haiku. I hope you will take a moment to at least follow along and consider making a regular or one-time post of your own – adding the hashtag #UroPoet.
I’ll be posting regularly from a second Twitter account @UroPoet where I will also be retweeting #UroPoet tweets. If the spirit moves you, you can also follow me @StorkBrian.
I had been using Twitter for a while but I never experienced the true power of this social media platform. It was a cold call from @VerranDeborah and @juliomayol when I started to notice the hashtag #SoMe4Surgery. I was pleasantly surprised and impressed by the active engagement of the #SoMe4Surgery participants. After participating in a #SoMe4Surgery live conversation event on #surgicalinfection, I finally realized the potential impact of a simple hashtag.
While I was amazed by how #SoMe4Surgery brought the surgical community together, many of the topics being discussed were not entirely relevant or specific to a urologist per se. I felt the need of a hashtag specific to Urology, and I quickly started to conceptualize and plan ahead in building up the #UroSoMe community. The #UroSoMe twitter account was officially registered in August 2018.
#UroSoMe stands for ‘Urology Social Media’. My initial thought about #UroSoMe was simple. I wanted to develop a hashtag specific to urology. I wanted to increase public awareness about different urological conditions. Most importantly, I wanted to bring the urology community closer together through this social media platform. I believe there is so much for us to learn from each other, and such interactions should never be bounded by physical or geographical restrictions. Coincidentally, I was invited to talk about social media at the 27th Malaysian Urological Conference 2018, and I decided to take this opportunity to introduce #UroSoMe to the urology community.
The initial response from the audience was promising. Even after the meeting, many urologists came to me for in-depth discussions about the opportunities and applications of social media in urology. I felt that #UroSoMe might really work and it was time to gather more people to establish the community. The first invitation sent in on 14 December 2018, which I often regard as the ‘start date’ of the #UroSoMe community.
By inviting and encouraging people around to use a common hashtag, the #UroSoMe community keeps growing. With increasing momentum, the first #LiveCaseDiscussions was planned. It was a pre-planned event for urologists to get ‘online’ and discuss about some posted cases. A polling had been held in advance, and the topic to be discussed was chosen to be ‘Stone’.
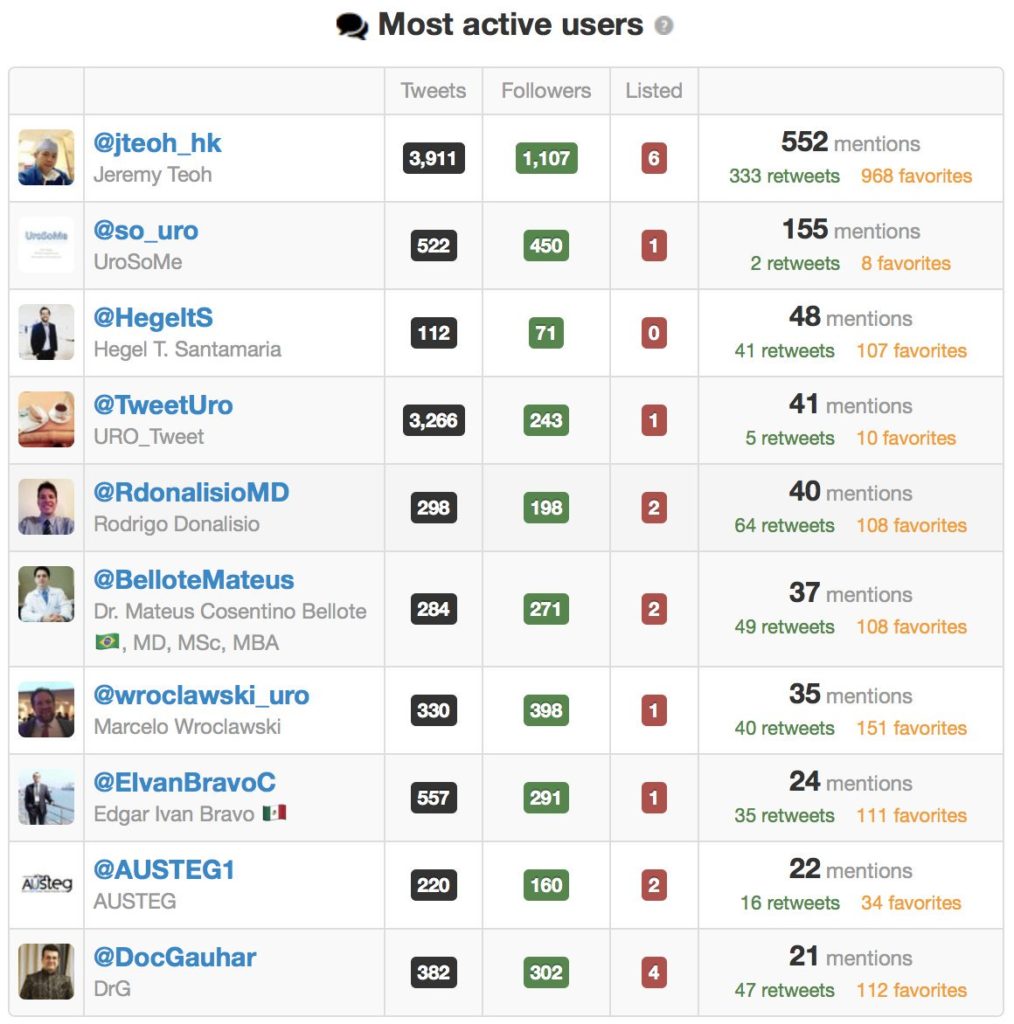
The #LiveCaseDiscussions was on air at 4pm (CET) on 5 January 2019. A total of 9 cases had been presented and discussed. Hosting this event was overwhelming with vigorous discussions among the participants. It took approximately 2 hours to ‘complete’ the event, but the conversations went on for the next few days. Special thanks must be given to the most active users. #UroSoMe and the first #LiveCaseDiscussions would never be successful without their tremendous support.
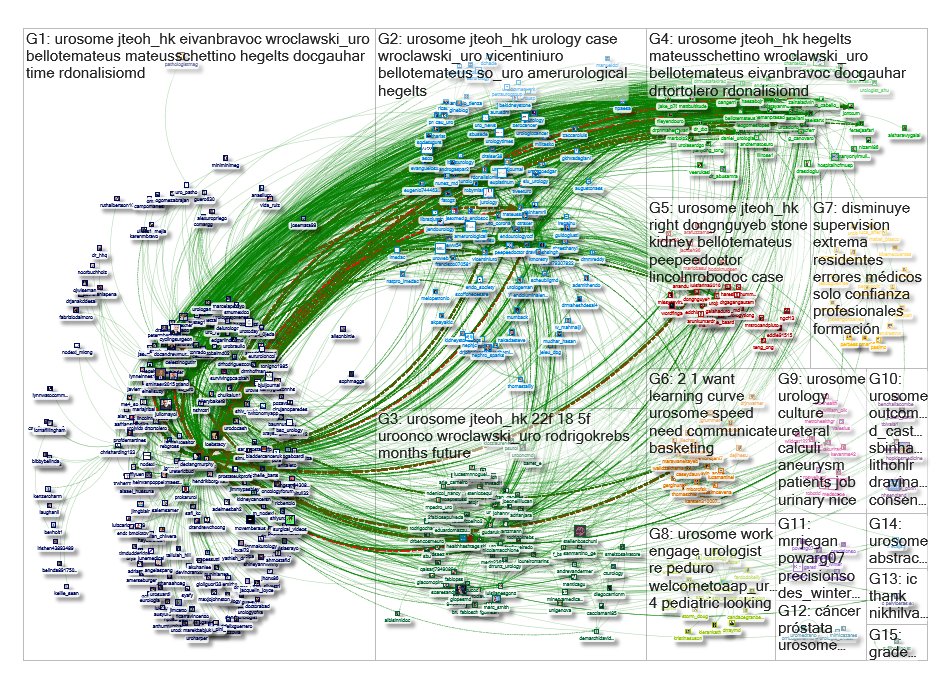
The immediate effect of the #UroSoMe #LiveCaseDiscussions event was overwhelming. This graph represents a network of 515 twitter users whose tweets contained the hashtag #UroSoMe. 6692 mentions, 1044 retweets and 617 replies were recorded within a 10-day period from 27 December 2018 to 6 January 2019. From a social science point of view, this picture represents a ‘tight crowd’, in which discussions are characterized by highly interconnected people with few isolated participants. I guess this is exactly how we feel about the urology community!
Apart from #LiveCaseDiscussions, the #UroSoMe working group is also keen to host events including #LiveForum, #LiveJournalClub and #LiveTeaching. This is only the beginning of #UroSoMe and we believe there is huge potential to be explored. It is only with your support that #UroSoMe can continue to grow. We look forward to meeting you on Twitter and,
hopefully, at #EAU19 and #AUA19 as well!
P.S. I must thank @juliomayol for the inspiration of #UroSoMe, @gmacscotland for his teaching on social media analytics, and @marc_smith for his support in NodeXL.
About the author:
Jeremy Teoh (@jteoh_hk) is a Urologist based in Hong Kong, China.