
Article of the week: Nerve sparing during RARP: Watch the weaker hand
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Pathological confirmation of nerve-sparing types performed during robot-assisted radical prostatectomy (RARP)
Woo Jin Ko, Gregory W. Hruby*, Andrew T. Turk†, Jaime Landman‡ and Ketan K. Badani*
Department of Urology, National Health Insurance Corporation Ilsan Hospital, Goyang, South Korea; Departments of *Urology and †Pathology, Columbia University Medical Center, New York, NY, and ‡Department of Urology, University of California Irvine, Irvine, Orange, CA, USA
OBJECTIVES
• To confirm that the surgeon achieved true intended histological nerve sparing during robot-assisted radical prostatectomy (RARP) by studying RP specimens.
• To aid the novice robotic surgeon to develop the skills of RARP.
PATIENTS AND METHODS
• Between June 2008 and May 2009, 122 consecutive patients underwent RARP by a single surgeon (K.K.B.). The degree of nerve sparing (wide resection [WR], interfascial nerve sparing [ITE-NS], intrafascial nerve sparing [ITR-NS]) on both sides was recorded. The posterior sectors of RP specimens from distal, mid, and proximal parts were evaluated.
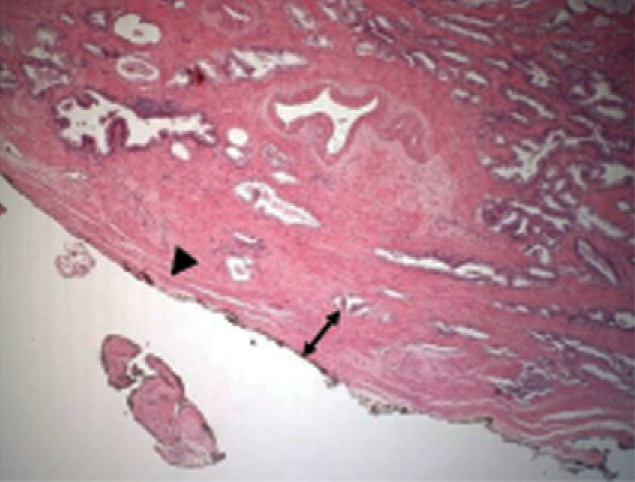
• Fascia width (FW) of each position in RP specimens were compared across nerve-sparing types (NSTs). FW was recorded at 15° intervals (3–9 o’clock position), measured as the distance between the outermost prostate gland and surgical margin.
• The slides were reviewed by an experienced uropathologist who was ‘blinded’ to the NST.
RESULTS
• In all, 93 men were included. The overall mean (SD) FW was the greatest in the order of WR, ITE-NS, and ITR-NS, at 2.42 (1.62), 1.71 (1.40) and 1.16 (1.08) mm, respectively (P < 0.001).
• FW was statistically significantly correlated with the surgical technique used. When the surgeon intended to perform various levels of nerve sparing, these were reflected in the FW.
• Interestingly, the left-side FW showed more variability than the right side. We suspect that this was a result of the surgeon’s right-hand dominance.
• Erectile function (EF) recovery rate according to NST was 88.9%, 77.3%, 65.6%, 56.3%, and 0% in bilateral ITR-NS, ITR-NS/ITE-NS, bilateral ITE-NS, ITE-NS/WR, and bilateral WR, respectively.
• To further validate and confirm these preliminary findings, additional studies involving multicentre cohorts would be required.
CONCLUSIONS
• The surgeon intended dissection and FW correlate, with ITR-NS providing the narrowest FW and the EF recovery rate was the highest in bilateral ITR-NS. There was more variability in FW outcome on the left side than the right.
• The novice robotic surgeon should consider this variability when performing RARP. It may have implications for technique improvement on nerve preservation for EF.
