
Podcast: Survival following cytoreductive nephrectomy: a comparison of existing prognostic models
Part of the BURST/BJUI Podcast Series
Mr Kenneth MacKenzie MBChB, FRCS (Urol) is a ST7 in Urology in North East England and BURST committee member.

Mr Kenneth MacKenzie MBChB, FRCS (Urol) is a ST7 in Urology in North East England and BURST committee member.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Clément-Zhao, A., Auvray, M., Aboudagga, H., Blanc-Durand, F., Angelergues, A., Vano, Y. A., Mercier, F., El Awadly, N., Verret, B., Thibault, C. and Oudard, S. (2018), Safety and efficacy of 2-weekly cabazitaxel in metastatic castration-resistant prostate cancer. BJU International, 121: 203–208. doi: 10.1111/bju.13855
To evaluate the safety and efficacy of a 2-weekly cabazitaxel schedule in patients with metastatic castration-resistant prostate cancer (mCRPC).
During the period October 2013 to February 2016, 43 patients with mCRPC were treated with cabazitaxel (16 mg/m2, on days 1 and 15 of a 4-week cycle) together with prophylactic granulocyte colony-stimulating factor (G-CSF). The safety profile and efficacy (prostate-specific antigen [PSA] response; biological, clinical or radiological progression-free survival [PFS] and overall survival [OS]) of the treatment were analysed.
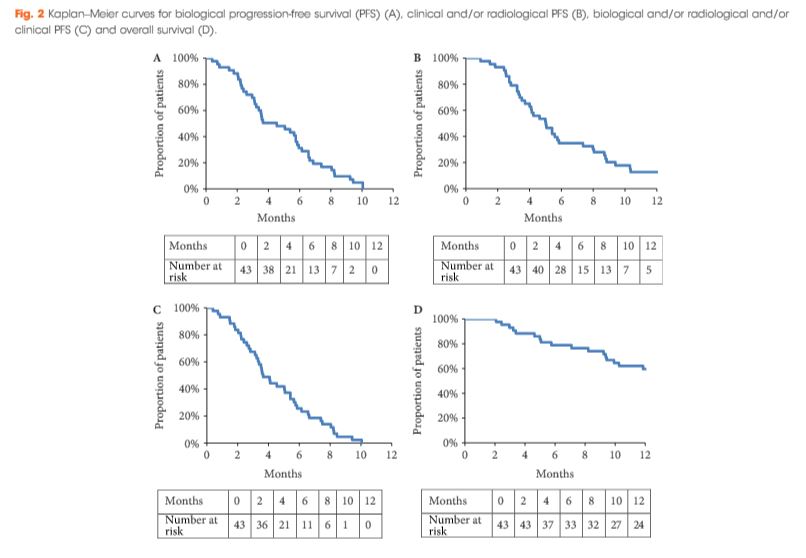
All patients had received prior docetaxel and 79.1% abiraterone acetate. At inclusion, 46.5% were aged >70 years and 27.9% had an Eastern Cooperative Oncology Group performance status ≥2. Six patients stopped treatment because of toxicity. Grade ≥3 toxicities were: asthenia (16.3%); neutropenia (11.6%); thrombocytopenia (9.3%); diarrhoea (7%), anaemia (4.7%), febrile neutropenia (4.7%) and haematuria (2.3%). In all, 52.4% achieved a ≥30% PSA response and 40.5% had a ≥50% PSA response. The median OS was 15.2 months.
This prospective pilot study suggests that cabazitaxel 16 mg/m² given 2-weekly has a manageable toxicity profile in docetaxel- and abiraterone acetate-pretreated patients with mCRPC. A prospective phase III trial comparing this regimen with the standard cabazitaxel regimen is planned to confirm these results.
In the present issue of BJUI, Clèment-Zhao et al. [1] have evaluated the safety profile of a 2-weekly regime of cabazitaxel (CBZ) at a dose of 16 mg/m2 in 43 patients with progressing, metastatic castration-resistant prostate cancer (mCRPC). Treatment was planned to have been delivered for a total of six cycles, with each cycle consisting of two 2-weekly applications of CBZ. The majority of patients had already received two life-extending systemic therapies, such as docetaxel and abiraterone acetate. Despite the prophylactic use of granulocyte colony-stimulating factor (G-CSF), 11.6% and 4.7% of patients developed grade ≥3 neutropenia or febrile neutropenia, respectively, and one patient even died from treatment-related toxicities. Only 75% of the scheduled six cycles could be delivered, although dose reduction of 20% was carried out in 37.2% of the patients. The authors recommend this type of treatment for elderly and frail patients and they provide the reader with the impression that the delivery of such a toxic regime in elderly and frail patients is accordance with the guidelines [2].
Based on the International Society of Geriatric Oncology (SIOG) guidelines [2], it is evident that the term ‘frailty’ requires a dedicated and sophisticated geriatric assessment using, for example, the G8 questionnaire. If a score <14 is calculated on this questionnaire, and the patients have been identified as having irreversible impairment, an intensive geriatric intervention might be undertaken to correct the underlying comorbidities. Only in the presence of correctable comorbidities should an adapted cancer therapy be initiated, while in their absence best supportive care seems to be the optimal approach. Of the 43 patients in the present phase II trial, none underwent a geriatric assessment and three-quarters of the patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1; therefore, only a minority of the treated patients represented frail patients, and conclusions should be drawn with great caution, also considering the relatively low number of patients recruited.
The frequency of 11.6% and 4.7% of grade 3/4 neutropenia and neutropenic fever, respectively, and an overall frequency of 34.9% grade 3/4 treatment-emergent adverse events is still quite high compared with the data from studies on the German Early-Access Programme (EAP) and the European EAP on CBZ, which included 111 and 746 patients with similar disease characteristics, of whom 7.2% and 15%, respectively, developed grade ≥3 neutropenia, despite non-regular use of G-CSF [3, 4].
Several factors might have contributed to the relatively high frequency of treatment-emergent adverse events in the present study. Firstly, the cumulative CBZ dose was 144 mg/m2 in the present study as compared with 100 mg/m2 in the European EAP and 162.5 mg/m2 in the German EAP, so that there was not a significant reduction in dose despite the lower dose delivered at each cycle. This might have contributed to impairment of bone marrow function over time. Secondly, bone marrow reserve appeared to differ among treated patients: ~50% of patients already had neutrophil counts below the normal values. As we have shown recently, neutrophil counts <4 000/mm3 were associated with an odds ratio of 1.73 (95% CI 1.25–2.39; P < 0.001) for developing grade 3/4 neutropenia [4]. Thirdly, age ≥75 years, but not age <75 years or ECOG performance status ≥2, was associated with a 1.66-fold (95% CI 1.09–5.52; P = 0.018) increased risk of significant neutropenia in the above-mentioned studies [3, 4]; however, it is unclear how many patients were aged >75 years in the present study.
As a result of these factors, it is still necessary to carefully select elderly patients with mCRPC prior to the recommendation of cytotoxic CBZ therapy, even at a reduced dose. Despite the fact that there is some weak evidence that severe neutropenia might be associated with a survival benefit, we need to bear in mind that this evidence is from post hoc analysis of fit and non-elderly patients recruited in the TROPIC trial [5]. We have no meaningfuldata from a cohort of elderly and vulnerable/frail patients and we have no data at all on quality of life in these patients; therefore, we should not overtreat and we should only consider frail and elderly patients with mCRPC for CBZ treatment if they have undergone geriatric assessment that has shown correctable comorbidities. Otherwise, there are numerous other treatment options in addition to chemotherapy, including best supportive care [6].
With regard to therapeutic efficacy, we always find it difficult to report median overall survival times of 15.2 months when the median follow-up time is only 12.9 months.
Every Month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Won Sik Jang, Myung Soo Kim, Won Sik Jeong, Ki Don Chang, Kang Su Cho, Won Sik Ham, Koon Ho Rha, Sung Joon Hong and Young Deuk Choi
Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea
To investigate the peri-operative and oncological outcomes of robot-assisted radical prostatectomy (RARP) in patients with oligometastatic prostate cancer (PCa).
We retrospectively reviewed the records of 79 patients with oligometastatic PCa treated with RARP or androgen deprivation therapy (ADT) between 2005 and 2015 at our institution. Of these 79 patients, 38 were treated with RARP and 41 were treated with ADT without local therapy. Oligometastatic disease was defined as the presence of five or fewer hot spots detected by preoperative bone scan. We evaluated peri-operative outcomes, progression-free survival (PFS), and cancer-specific survival (CSS). We analysed data using Kaplan–Meier methods, with log-rank tests and multivariate Cox regression models.
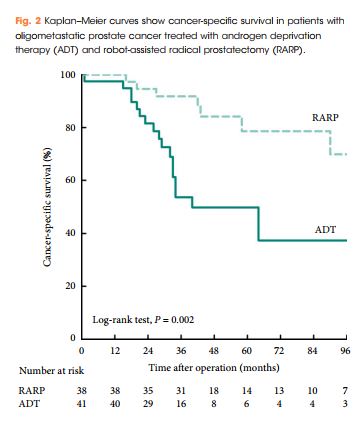
Patients treated with RARP experienced similar postoperative complications to those previously reported in RP-treated patients, and fewer urinary complications than ADT-treated patients. PFS and CSS were longer in RARP-treated compared with ADT-treated patients (median PFS: 75 vs 28 months, P = 0.008; median CSS: not reached vs 40 months, P = 0.002). Multivariate analysis further identified RARP as a significant predictor of PFS and CSS (PFS: hazard ratio [HR] 0.388, P = 0.003; CSS: HR 0.264, P = 0.004).
We showed that RARP in the setting of oligometastatic PCa is a safe and feasible procedure which improves oncological outcomes in terms of PFS and CSS. In addition, our data suggest that RARP effectively prevents urinary tract complications from PCa. The study highlights results from expert surgeons and highly selected patients that cannot be extrapolated to all patients with oligometastatic PCa; to confirm our findings, large, prospective, multicentre studies are required.
In this issue of BJU International, Jang et al. [1] investigate the perioperative and oncological outcomes of robot-assisted radical prostatectomy (RARP) in oligometastatic prostate cancer. The authors evaluated a retrospective cohort of 79 patients with oligometastatic prostate cancer, defined as up to five bony metastases on bone scan without visceral metastasis on conventional CT, treated either with RARP (n = 38, 48%) or androgen-deprivation therapy (ADT: n = 41, 52%). They found that cytoreductive RARP was associated with longer progression-free survival (PFS) and cancer-specific survival (CSS) relative to the ADT cohort at a median follow-up of 40 months.
The authors exclusively use the robotic approach for RP in the metastatic prostate cancer setting. Overall, they should be commended for demonstrating the feasibility of RARP in the metastatic setting, with a median operating room time of 147 min and complication rate of ~15%. This is in the same range as the 164 min operative time and 20% complication rate reported in a recent multi-institutional cytoreductive RP (cRP) series, consisting of both open and robotic approaches [2]. However, it is important to note that Jang et al. [1] had a 79% positive margin rate compared to 54% for Sooriakumaran et al. [2]. Furthermore, Jang et al. [1] had a median hospital stay of 5 days compared to 2–3 days in the USA centres [2]. These findings underscore the significant difficulty often encountered in metastatic cases, despite robotic assistance. Thus, we believe the age-old debate of open vs robotic prostatectomy is perhaps less relevant in the cytoreductive setting, where surgeon experience and expertise may be more critical drivers of outcome.
Although there is some evidence in favour of cRP compared to the standard of care, selection bias, limited collection and analysis of much clinical data, and short follow-up often plague most series. Understandably, the current manuscript by Jang et al. [1] also suffers from some of these limitations and leaves some questions unanswered. For instance, did the number of bone metastases, PSA doubling time at diagnosis, and distribution of lymphadenopathy (pelvic vs extra-pelvic) differ between cRP and ADT groups and thus confound the impact of cRP on survival? In addition, the authors may wish to report overall survival, so that their series can be more readily compared to the existing literature. Moreover, the median CSS was only 40 months in the ADT group, whereas it was not even reached in the low-volume arm of the ChemoHormonal Therapy Versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer (CHAARTED) [3], suggesting that the control group in the current manuscript may have had higher volume metastatic disease. Lastly, there is no evaluation of the impact of adjuvant ADT and radiation therapy on CSS, and further studies may wish to explore if such multi-modal approaches may yield a benefit in the cytoreductive setting.
The existing literature on cRP remains in the nascent stage and is conflicting. The first large studies to suggest a benefit for cRP were retrospective series based on large cancer databases. Subsequently, Heidenreich et al. [4] explored the role of cRP in a case-control study, which found a significantly longer PFS and CSS in a group of 23 men undergoing neoadjuvant ADT + cRP compared to 38 men treated with ADT alone. On the other hand, a prospective investigation comparing 43 men with low-volume bone metastasis treated with cRP to 38 men treated with ADT did not show a benefit for time-to-castration-resistance or overall survival [5]. Moschini et al. [6] also found no survival benefit for cRP with 5-years of follow-up relative to a cohort of ADT patients with CSS more consistent with randomised data from the CHAARTED [3]. The present study by Jang et al. [1] adds to the growing body of retrospective series advocating cRP in select patients.
Whilst a full discussion of the putative biological mechanisms proposed to explain a potential survival benefit of cRP is beyond this editorial, they can be broadly grouped into the following: removal of the primary source of circulating tumour cells, reducing the number of cells that can develop resistant mechanisms for systemic therapy, removal of immunosuppressive cytokines, abscopal effects, and decreasing tumour-growth promoting factors. Ultimately, the ‘proof is in the pudding’, and the results of several randomised trials (Testing radical prostatectomy in men with oligometastatic prostate cancer that has spread to the bone [TRoMbone], NCT01751438, and NCT02454543) are eagerly awaited to determine if cRP can benefit patients.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Jon Rees discussing his paper.
If you only have time to read one article this week, it should be this one.
TRC105 is a chimeric immunoglobulin G1 monoclonal antibody that binds endoglin (CD105). This phase I open-label study evaluated the safety, pharmacokinetics and pharmacodynamics of TRC105 in patients with metastatic castration-resistant prostate cancer (mCRPC).
Patients with mCRPC received escalating doses of i.v. TRC105 until unacceptable toxicity or disease progression, up to a predetermined dose level, using a standard 3 + 3 phase I design.
A total of 20 patients were treated. The top dose level studied, 20 mg/kg every 2 weeks, was the maximum tolerated dose. Common adverse effects included infusion-related reaction (90%), low grade headache (67%), anaemia (48%), epistaxis (43%) and fever (43%). Ten patients had stable disease on study and eight patients had declines in prostate specific antigen (PSA). Significant plasma CD105 reduction was observed at the higher dose levels. In an exploratory analysis, vascular endothelial growth factor (VEGF) was increased after treatment with TRC105 and VEGF levels were associated with CD105 reduction.
TRC105 was tolerated at 20 mg/kg every other week with a safety profile distinct from that of VEGF inhibitors. A significant induction of plasma VEGF was associated with CD105 reduction, suggesting anti-angiogenic activity of TRC105. An exploratory analysis showed a tentative correlation between the reduction of CD105 and a decrease in PSA velocity, suggestive of potential activity of TRC105 in the patients with mCRPC. The data from this exploratory analysis suggest that rising VEGF level is a possible compensatory mechanism for TRC105-induced anti-angiogenic activity.

In this issue of BJU International, Karzai et al. [1] report the results of a phase I study of the anti-endoglin antibody TRC105 in patients with metastatic castration-resistant prostate cancer (mCRPC). This is a new anti-angiogenic compound with a unique mechanism of action.
Since the introduction of the concept of angiogenesis as a requirement for tumour growth and survival of solid cancers, a substantial body of research has emerged, establishing inhibition of angiogenic pathways as an important part of the armamentarium in several tumour types [2]. The idea of dynamic tumour angiogenic factors that are able to mediate neovascularisation has also been associated with tumour growth, progression and metastases in prostate cancer [1].
Some studies have revealed that microvessel density, a histological measurement of tumour angiogenesis assessed by immunohistochemical CD105 (endoglin), correlates with higher Gleason score and may predict disease progression, as well as poorer survival outcomes in patients with mCRPC. Accordingly, angiogenesis is considered an attractive target for therapeutic intervention in this disease and anti-angiogenic strategies have been studied in several clinical settings. Unfortunately, well established anti-angiogenic therapies have failed to improve survival outcomes in advanced prostate cancer. Bevacizumab or afilbercept, both combined with docetaxel, were evaluated in phase III clinical trials and no survival benefit was observed over docetaxel alone. Similarly, sunitinib was no better than placebo after chemotherapy treatment. Moreover, the recent COMET-1 trial failed to show survival benefit with cabozantinib, a dual vascular endothelial growth factor (VEGF) and MET inhibitor, in patients with mCRPC and, as a consequence, enrolment in other studies evaluating this agent has been discontinued. Strikingly, although no survival benefit has been reported, progression-free survival benefit has been observed in all of these trials.
Other anti-angionenic therapies have been investigated in patients with mCRPC. A phase II study combining thalidomide and bevacizumab with docetaxel plus prednisone showed that this is an active combination in this subset of patients. Unfortunately, the combination resulted in significant neurotoxicity and myelotoxicity, limiting its clinical use [3]. Lenalidomide was developed to have a more favourable toxicity profile compared with thalidomide and has shown activity as a single agent in patients with non-metastatic, biochemically-relapsed prostate cancer. Again, the large randomised phase III trial comparing docetaxel plus lenalidomide vs docetaxel plus placebo failed to show improvement in overall survival with the addition of this agent [4]. Finally, tasquinimod, another compound targeting angiogenesis, is under evaluation and the final results have not yet been reported. A phase III placebo-controlled study (NCT01234311), designed based on promising phase II data, is ongoing in men with mCRPC with bone metastases and is powered to detect an improvement in overall survival.
Overall, limited activity have been reported with the available agents and, until the results of the tasquinimod trial become available, additional investigations with better-targeted therapies and tools for patient selection are needed to define how this class of agents can improve survival outcome in mCRPC. In this setting, CD105 (endoglin), a homodimeric cell membrane glycoprotein that was initially identified as a human leukaemia-associated antigen, and later also found on endothelial cells, might serve as a reasonable reference point to continue research in this direction. CD105 is a TGFβ co-receptor that is essential for angiogenesis and is selectively expressed on proliferating endothelial cells of tumour vessels. All these properties make CD105 an attractive target for drug development, as targeting the vasculature of the tumour may be more effective than conventional anti-angiogenic therapy, such as anti-VEGF therapy [5].
TRC105, an antibody to CD105, caused a overall reduction in angiogenic biomarkers and reduced tumour burden in a phase I study of advanced solid tumours at doses that were well tolerated. Karzai et al. [1] report the results of a phase I study of TRC105 in patients with mCRPC. This study was designed to define the maximum tolerated dose and to access the safety and tumour activity of TRC105 in a small cohort of patients with mCRPC. Of note, given that TRC105 has a unique mechanism of action, the toxicity profile was not similar with those commonly associated with VEGF inhibition and, at 20 mg/kg, the drug was well tolerated. Although evaluating a small number of patients, the tumour activity of this agent seems to be similar to that of the other anti-angiogenic therapies, and the potential benefit will most likely be seen when combined with other therapies. In addition, exploratory analyses have identified changes in plasma VEGF and CD105 staining on endothelial cells of tumour vessels after treatment with TRC105. These findings suggest that higher levels of VEGF are a possible compensatory mechanism for TRC105-induced anti-angiogenic activity, providing a rationale for TRC105 combination with other anti-VEGF therapies.
It has been hypothesised that endoglin-expressing vessels resist treatment, with antibody targeting the VEGF receptor by allowing continued growth of human tumour xenografts. Therefore, combining anti-angiogenic strategies with agents having different mechanisms of action may be an option to overcome resistance and produce anti-tumour responses [6]. Results from the combination of TRC105 with axitinib in patients with metastatic RCC may support this concept and are now under evaluation (NCT01806064).
Over the last 5 years, treatment of mCRPC has evolved rapidly. Immunotherapy agents (sipuleucel-T), androgen inhibitors (abiraterone acetate and enzalutamide), radioisotope (Radium-223) and cytotoxic chemotherapy (cabazitaxel) have been shown to improve overall survival in randomised phase III clinical trials. However, despite these recent advances, disease progression remains a major cause of morbidity and mortality and new therapies or combinations are required to improve patient care offering them a higher chance of achieving long-term survival.
Anti-angiogenic agents are active in certain settings of prostate cancer and some significant responses have been reported. However, a deeper understanding of the biology of mCRPC is required to characterise the complex angiogenic pathways and to elucidate mechanisms of resistance to this class of agents. This, together with the development of biomarkers to predict responses to anti-angiogenic therapies, might assist in guiding novel treatment combinations and optimising clinical benefit based on patient selection.

TRC105 is a chimeric immunoglobulin G1 monoclonal antibody that binds endoglin (CD105). This phase I open-label study evaluated the safety, pharmacokinetics and pharmacodynamics of TRC105 in patients with metastatic castration-resistant prostate cancer (mCRPC).
Patients with mCRPC received escalating doses of i.v. TRC105 until unacceptable toxicity or disease progression, up to a predetermined dose level, using a standard 3 + 3 phase I design.
A total of 20 patients were treated. The top dose level studied, 20 mg/kg every 2 weeks, was the maximum tolerated dose. Common adverse effects included infusion-related reaction (90%), low grade headache (67%), anaemia (48%), epistaxis (43%) and fever (43%). Ten patients had stable disease on study and eight patients had declines in prostate specific antigen (PSA). Significant plasma CD105 reduction was observed at the higher dose levels. In an exploratory analysis, vascular endothelial growth factor (VEGF) was increased after treatment with TRC105 and VEGF levels were associated with CD105 reduction.
TRC105 was tolerated at 20 mg/kg every other week with a safety profile distinct from that of VEGF inhibitors. A significant induction of plasma VEGF was associated with CD105 reduction, suggesting anti-angiogenic activity of TRC105. An exploratory analysis showed a tentative correlation between the reduction of CD105 and a decrease in PSA velocity, suggestive of potential activity of TRC105 in the patients with mCRPC. The data from this exploratory analysis suggest that rising VEGF level is a possible compensatory mechanism for TRC105-induced anti-angiogenic activity.

 This year’s final #urojc concluded with intense discussions on the role of local treatment (LT) in metastatic prostate cancer. One study author, @mbwilliams95 joined the conversation to provide valuable insights.
This year’s final #urojc concluded with intense discussions on the role of local treatment (LT) in metastatic prostate cancer. One study author, @mbwilliams95 joined the conversation to provide valuable insights.

Despite the fact only a small number of Stage IV patients had LT between 2004-2010 (post docetaxel era), this population based study revealed statistically significant differences between overall survival (OS) and disease specific survival (DSS).
| Treatment | Patient number | 5 yr OS (%) | DSS (%) |
| Radical prostatectomy (RP) |
245 | 67.4 | 75.8 |
| Brachytherapy(BT) | 129 | 52.6 | 61.3 |
| No surgery or radiation (NSR) | 7811 | 22.5 | 48.7 |
So, can this be the start of a paradigm shift?

We may need to question our conventional approach.

Although some would consider performing RP in this population,


Others disagreed

Tzelepi et al (J Clin Oncol 2011 Jun 20;29(18):2574-81) suggested that potentially lethal cancers persist in the primary tumor and may contribute to progression. This is a possible explanation for this study’s findings, which echoed earlier results by Swanson et al (J Urol. 2006 Oct;176: 1292-8) and Shao et al (Eur Urol 2013 May 21. [Epub ahead of print]). However, SEER lacks information regarding the extent of bony metastasis, an entity that undoubtedly influences patient survival. Furthermore, patients treated with RP were 10 yrs younger than the NSR group (62 vs 72), and had a higher proportion of those with PSA <20.

To reduce bias produced by significant comorbidities, authors excluded those dying within a year of diagnosis and found the 5-yr OS continued to be higher in patients undergoing RP (76.5%) or BT (58.2%). However, patients with three or more of: age ≥70 yr, cT4 disease, PSA ≥20 ng/ml, high-grade disease, and pelvic lymphadenopathy had a 5-yr OS survival (38.2%) and a DSS probability (50.1%) similar to NSR patients.
Several contributors identified that Will Rogers phenomenon may be at play


Ultimately, the jury is still out on what is the most effective treatment of significant prostate cancer

Studies (in addition to the follow-on cohort study arising from this review), are underway



To conclude, it has been


In spite of the global participation, much of the banter involved our US urological colleagues. On this basis, the Best Tweet Prize has been awarded to a provocative tweet from our UK colleague Ben Challacombe (@benchallacombe).

Thank you to European Urology (@EUPlatinum) for allow open access to the article discussed this month. Thank you to Nature Reviews Urology for supporting the Best Tweet prize, which is a complimentary 12 months on-line subscription to the journal.
We look forward to seeing you at the January #urojc.
Dr Janice Cheng is an Australian Urology Trainee, currently based at Western Hospital. She has an interest in teaching, and enjoys laparoscopies, endoscopies, as well as male/female incontinence management. Twitter @JustUro
Authors: Gupta, Chaitali; Kumar, Rajeev
Corresponding Author: Shailesh Sahay, All India Institute of Medical Sciences, Urology, New Delhi, India. Email: [email protected]

Date added to bjui.org: 24/06/2011
DOI: 10.1002/BJUIw-2011-029-web