Article of the month: Risk of metastatic disease on 68-gallium‐prostate‐specific membrane antigen PET/CT scan for primary staging of 1253 men at the diagnosis of PCa
Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial and a video prepared by the authors. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, it should be this one.
Risk of metastatic disease on 68Gallium‐prostate‐specific membrane antigen positron emission tomography/computed tomography scan for primary staging of 1253 men at the diagnosis of prostate cancer
John W. Yaxley*†‡, Sheliyan Raveenthiran†‡, François-Xavier Nouhaud‡§, Hemamali Samaratunga†¶, William J. Yaxley†‡, Geoff Coughlin*‡, Anna J. Yaxley**, Troy Gianduzzo††, Boon Kua‡‡, Louise McEwan‡‡ and David Wong‡‡
*Wesley Urology Clinic, †Department of Medicine, University of Queensland, ‡Royal Brisbane and Women’s Hospital, Brisbane, Queensland, Australia, §Department of Urology, Rouen University Hospital, Rouen, France, ¶Aquesta Uro-pathology, **School of Medicine, Griffith University, ††Brisbane Prostate Clinic, and ‡‡Wesley Medical Imaging, Brisbane, Queensland, Australia
Abstract
Objective
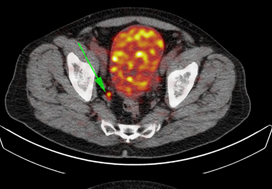
To determine the number of men with 68gallium‐prostate‐specific membrane antigen positron emission tomography/computed tomography (68Ga‐PSMA PET/CT) avid metastasis at diagnosis, as most data on 68Ga‐PSMA PET/CT are for the evaluation of recurrent disease after primary treatment and to our knowledge this study is the largest series of primary prostate cancer staging with 68Ga‐PSMA PET/CT.
Patients and Methods
A retrospective review conducted on 1253 consecutive men referred by urologists or radiation oncologists to our tertiary referral centre for 68Ga‐PSMA PET/CT scan for staging at the initial diagnosis of prostate cancer between July 2014 and June 2018.
The primary outcome measure was to determine the risk of metastasis based on 68Ga‐PSMA PET/CT. Patients were risk stratified based on histological biopsy International Society of Urological Pathology (ISUP) grade, prostate‐specific antigen (PSA) level, and staging with pre‐biopsy multiparametric magnetic resonance imaging (mpMRI). Univariate and multivariate logistic regression were used to analyse results.
Results
The median PSA level was 6.5 ng/mL and median ISUP grade was 3, with high‐risk disease in 49.7%. The prostate primary was PSMA avid in 91.7% of men. Metastatic disease was identified in 12.1% of men, including 8.2% with a PSA level of <10 ng/mL and 43% with a PSA level of >20 ng/mL. Metastases were identified in 6.4% with ISUP grade 2–3 and 21% with ISUP grade 4–5. Pre‐biopsy mpMRI identified metastasis in 8.1% of T2 disease, increasing to 42.4% of T3b. Lymph node metastases were suspected in 107 men, with 47.7% outside the boundaries of an extended pelvic lymph node dissection. Skeletal metastases were identified in 4.7%. In men with intermediate‐risk prostate cancer, metastases were identified in 5.2%, compared to 19.9% with high‐risk disease.
Conclusions
These results support the use of 68Ga‐PSMA PET/CT for primary staging of prostate cancer. Increasing PSA level, ISUP grade and radiological staging with mpMRI were all statistically significant prognostic factors for metastasis on both univariate and multivariate analysis.