Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorialwritten by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, it should be this one.
Pim J. van Leeuwen*, Maarten Donswijk†, Rohan Nandurkar‡, Phillip Stricker§¶, Bao Ho**, Stijn Heijmink††, Esther M.K. Wit*, Corinne Tillier*, Erik van Muilenkom*, Quoc Nguyen§, Henk G. van der Poel* and Louise Emmett‡§**
*Department of Urology, †Department of Nuclear Medicine, The Netherlands Cancer Institute, Amsterdam, The Netherlands, ‡Faculty of Medicine, University of New South Wales Sydney, §The Australian Prostate Cancer Research Centre-NSW, The Garvan Institute of Medical Research, ¶St Vincent’s Clinic, **Department of Theranostics and Nuclear Medicine, St Vincent’s Hospital Sydney, Sydney, New South Wales, Australia and ††Department of Radiology, The Netherlands Cancer Institute, Amsterdam, The Netherlands
To determine the value of gallium‐68‐prostate‐specific membrane antigen (68Ga‐PSMA)‐11 positron emission tomography (PET) /computed tomography (CT) in men with newly diagnosed prostate cancer.
Patients and methods
We analysed results of 140 men with intermediate‐ and high‐risk prostate cancer. All men underwent 68Ga‐PSMA‐11 PET/CT and multiparametric magnetic resonance imaging (mpMRI) before radical prostatectomy (RP) with extended pelvic lymph node (LN) dissection. For each patient, the clinical and pathological features were recorded. Prostate‐specific antigen (PSA) was documented at staging scan, and after RP, at a median (interquartile range) of 110 (49–132) days. A PSA level of ≥0.03 ng/mL was classified as biochemical persistence (BCP). Logistic regression was performed for association of clinical variables and BCP.
Results
In these 140 patients with intermediate‐ and high‐risk prostate cancer, 27.1% had PSMA PET/CT‐positive findings in the pelvic LNs. Sensitivity and specificity for detection of LN metastases were 53% and 88% (PSMA PET/CT) and 14% and 99% (mpMRI), respectively. The overall BCP rate was 25.7%. The BCP rate was 16.7% in men who were PSMA PET/CT LN‐negative compared to 50% in men who were PSMA PET/CT LN‐positive (P < 0.05). The presence of PSMA‐positive pelvic LNs was more predictive of BCP after RP than cT‐stage, PSA level, and the Gleason score, adjusted for surgical margins status.
Conclusions
68Ga‐PSMA‐11 PET/CT is highly predictive of BCP after RP, and should play an important role informing men with intermediate‐ or high‐risk prostate cancer.
While molecular imaging is not exactly a new technology (TIME Magazine named PET-CT as the medical invention of the year back in 2000), recent developments in radio-pharmacy have positioned the field at the forefront of innovations in cancer imaging and, tantalisingly, novel therapeutic approaches to cancer treatment.
Urologists have typically been forward thinking and innovative, and have been quick to acknowledge the value of molecular imaging as a tool to enhance the accuracy of the diagnostic process and improve patient outcomes. The recent development of radiotracers directed against prostate-specific-membrane-antigen (PSMA) has taken things to a new level; there is now a solid body of evidence for the performance of 68Ga-PSMA PET/CT in primary and secondary staging, with an ability to accurately detect small volume disease at far lower serum PSA levels – the use of 68Ga-PSMA PET/CT as a diagnostic adjunct is becoming increasingly mainstream in continental Europe and Australia.
Oxford PSMA Symposium 2018
It is in this context that, on 22 November 2018, the Nuffield Department of Surgical Sciences in Oxford hosted a symposium at the Old Road Campus Research Building focused on the utility of PSMA-related technologies. The symposium attracted an impressive array of attendees from across the UK, Europe and Australia.
The symposium was opened with comments by Professor Freddie Hamdy of Oxford, who welcomed all attendees and speakers, some of whom who had travelled more than 10,000 miles to attend the gathering.
Many uses for PSMA in specialist prostate cancer management
Liberal use of PSMA-PET down under
The first speaker, Professor Declan Murphy, from Melbourne’s Peter MacCallum Cancer Centre, shared comprehensive data and experience from Victoria in Australia, where access to 68Ga-PSMA PET/CT is seemingly unrestricted. Professor Murphy delivered a fascinating talk, expounding the gamut of PSMA PET applications in prostate cancer, from primary staging (promising data), to biochemical recurrence (there is definite evidence that PSMA PET accurately detects early recurrence and can guide salvage treatment options), right through to therapeutic uses of PSMA. In particular, he discussed the use of Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) as a treatment in men with CRPC, presenting the findings of their recent Lancet Oncology study led by Michael Hoffman. Although still in the early stages, the data here look very exciting and hale a potential revolution in the way we manage high risk and advanced prostate cancer.
Declan Murphy expounds the translational utility of PSMA imaging and theranostics
How easy is it to set up a PSMA imaging service in the UK?
The next speaker was Professor Jamshed Bomanji from the Institute of Nuclear Medicine, University College London (UCL), who presented an eye-opening talk that focussed on the challenges of setting up a PSMA-PET service within an NHS Trust in England. The effort he and his team put into developing their service in the face of significant practical resistance has been frankly heroic. Pleasingly, these efforts have been worthwhile as the team from UCL have clearly demonstrated that PSMA PET/CT has had a significant impact on the management of men with biochemical recurrence with the team contributing to guidelines drawn up to standardise use, keeping similar standards of testing as https://www.blinkhealth.com/zoloft. It is very disappointing that NHS England saw fit to withdraw funding for the gallium tracer required for PSMA-PET scanning in August 2018. This does seem rather short-sighted given the clear evidence favouring the utility of PSMA-PET over other modalities such as FDG or Choline-PET, both of which are still funded. All in all, Professor Bomanji’s talk was a sobering examination of the challenges we face in our commitment to delivering cutting edge, world-class cancer services whilst at the same time considering the financial implications to the NHS of providing such high-end services.
Associate Professor Bart Cornelissen along with Dr Rebekka Hueting who runs PROx (PET Radiopharmacy Oxford) presented their intentions for 68Ga-PSMA-PET imaging in Oxford, and the University’s imminent plan to install a cyclotron on site that will allow PET imaging with locally generated radioisotopes to increase dose efficiency – the half-life of gallium means that any requirement to transport the dose reduces the number of scans that can be performed at destination. This is particularly important given some recent negative press coverage.
Surgery for men with metastases?
Prasanna Sooriakumaran (PS) of University College London Hospital (UCLH) Department of Urology discussed the TRoMbone Study, a UK feasibility RCT that he has set up aimed at testing radical prostatectomy in men with oligometastatic prostate cancer. This interesting study promises to tease out the possible benefits of radical prostatectomy to men with low-volume metastatic disease. There are examples in other cancers whereby aggressive management of the primary tumour confers survival benefits in patients with low-burden metastatic disease and it is not unreasonable to think this may be the case for prostate cancer. Recruitment to such trials of ‘oligometastatic’ disease is contingent upon definitions of ‘low-volume’ disease, and accurate detection of such disease. PSMA-PET imaging is positively helping with this paradigm with its far superior sensitivity to conventional cross-sectional staging.
PSMA as a tool to improve surgery
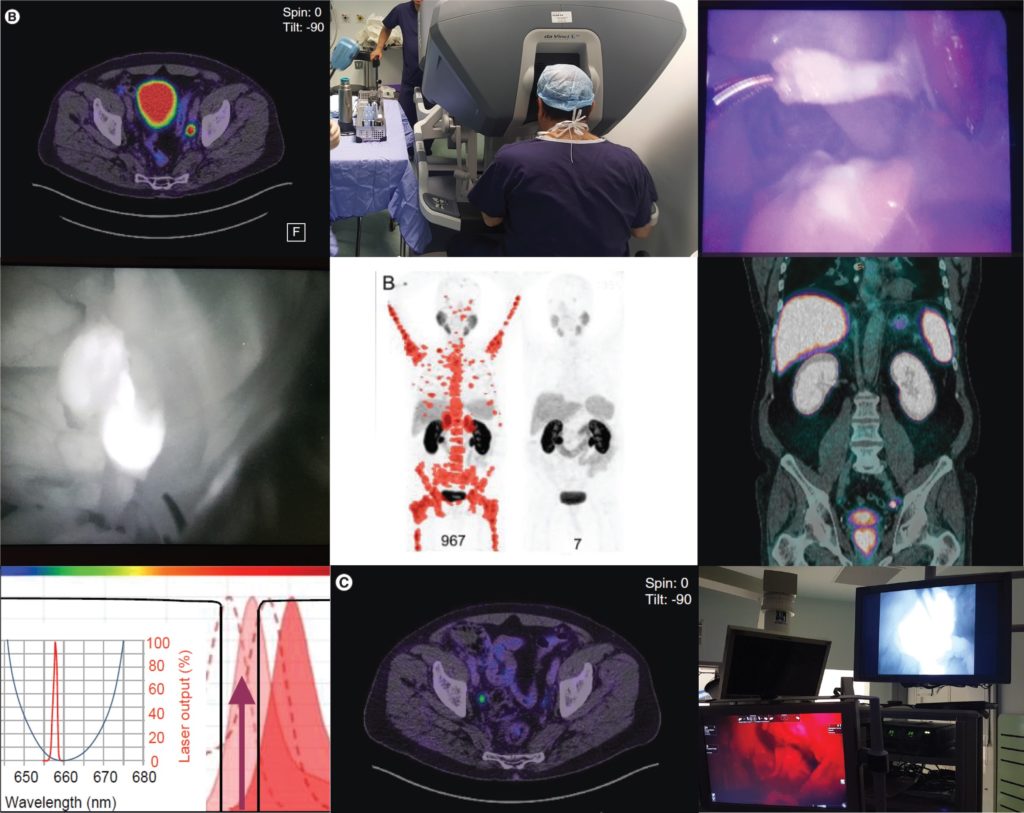
Pim van Leeuwen of the Netherlands Cancer Institute delivered an engaging talk entitled “PSMA intra-operative enhancement of lymph node dissection”, accompanied by some excellent video demonstrations. Next up were Boris Vojnovic and Alastair Lamb of Oxford who discussed fluorescence optics and intra-operative use of PSMA as part of the on-going ProMOTE study (Prostate Molecular Targeting to Enhance Surgery). We wish the investigators good luck as the study progresses and we eagerly look forward to seeing the data as they emerge.
Summary
In summary, the Oxford PSMA symposium 2018 brought together clinicians from around the globe who share a common enthusiasm for PSMA-related technologies that promise to revolutionise prostate cancer management in the near future. Common themes included the use of PSMA in staging, therapeutics and intra-operative guidance. The message from our overseas guests, both European and Antipodean, was that PSMA-based imaging is increasingly part of routine care in the management of prostate cancer and definite benefits are seen, particularly in regard to accurate staging and identification of very early recurrence. While we in the UK are a little behind the curve when it comes to adoption of this increasingly established technology, we are hopeful of increasing the use of this technology in the NHS in order to rationalise appropriate treatment, reduce futile expenditure and ensure gold-standard management of men with prostate cancer.
Conference dinner at Balliol College, Oxford, UK From Left: Alastair Lamb (Oxford), Declan Murphy (Melbourne), Freddie Hamdy (Oxford), Boris Vojnovic (Oxford), Prasanna Sooriakumaran (UCLH), Richard Bryant (Oxford), Ben Lamb (Cambridge)
Aaron Leiblich, Clinical Lecturer, Nuffield Department of Surgical Sciences; Alastair Lamb, Consultant Urologist, Churchill Hospital Cancer Centre; on behalf of the meeting faculty
Alastair Lamb is a Cancer Research UK Clinician Scientist, Senior Fellow in Robotic Surgery & Honorary Consultant Urologist at the Nuffield Department of Surgery, University of Oxford, and Oxford University Hospitals NHS Foundation Trust. Alastair is interested in delivering excellent and timely prostate cancer care, focussing on state-of-the-art diagnostics with multiparametric MRI and targeted transperineal biopsies, followed by robotic-radical prostatectomy (RARP) or active surveillance. He also has an interest in novel molecular imaging techniques such as 68Ga-PSMA PET/CT and their use in disease stratification and selection of patients for surgery. Alastair is a local investigator for the ProMOTE, PART and TRoMbone studies.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
11C-acetate positron-emission tomography/computed tomography imaging for detection of recurrent disease after radical prostatectomy or radiotherapy in patients with prostate cancer
To evaluate, in a prospective study, the effectiveness of computed tomography (CT)-matched 11C-acetate (AC) positron-emission tomography (PET) in patients with prostate cancer (PCa) who had prostate-specific antigen (PSA) relapse after radical prostatectomy (RP) or radiotherapy (RT).
Patients and Methods
In 103 relapsing patients after RP (n = 97) or RT (n = 6) AC-PET images and CT scans were obtained. In patients with AC-PET-positive results with localized PCa recurrence, detected lesions were resected and histologically verified or, after local RT, followed-up by PSA testing. Patients with distant disease on AC-PET were treated with androgen deprivation/chemotherapy.
Results
Of 103 patients, 42 were AC-PET-positive. PSA levels were <1.0, <2.0 and <4.0 ng/mL in six, 16 and 20 patients, respectively. In 25/42 patients AC-PET suggested lymph node metastases: 16/25 patients underwent surgery (10/16 metastasis, 6/16 inflammation); 9/25 patients underwent RT of lymph node metastases, which was followed by decreasing PSA level. In 17/42 patients who had distant disease, systemic treatment was commenced. Combining patients who underwent surgery and those who underwent RT, 19/25 patients were true-positive in terms of AC-PET (positive predictive value 76%). In 5/19 patients, PSA level was <2.0 ng/mL, in 2/19 patients it was <1.0 ng/mL and in 14/19 patients it was 5.4–23.1 ng/mL. In AC-PET-positive patients after surgery or RT (without androgen deprivation), median (range) time to renewed PSA increase was 6 (5–9) months.
Conclusions
Only a minority of patients with relapsing PCa appear to benefit from AC-PET for guiding potential local treatment. False-positive results show that factors other than tumour metabolism induce increased AC uptake. The time free of recurrence after local treatment was shorter than expected.
The search for the ideal imaging method to detect small metastatic deposits has largely remained elusive in the field of prostate cancer. However, functional positron emission tomography (PET)/CT is now guiding us in different directions. 11C-acetate PET/CT imaging was one of the first molecular imaging probes showing promise in clinical studies, along with 11C-choline, and more recently challenged by 68Ga-prostate-specific membrane antigen (PSMA) PET/CT [1-3]. So against this background, what does this new study by Esch et al. [4] presented here offer us?
Let us rewind and focus on where molecular imaging may have an impact in prostate cancer. In primary staging, the potential to accurately identify oligometastatic disease or even widespread metastatic disease before primary gland treatment is clearly advantageous. It can allow for wider treatment fields (extended lymphadenectomy or radiation fields), directed treatment of oligometastatic disease, placement into appropriate cytoreductive trials, and in some instances consideration of the use of earlier chemo-hormonal therapy. This study did not address this important clinical scenario [4]. Nor did it focus on primary diagnosis, another ‘holy grail’ for imaging more recently dominated by MRI [5].
The other group studied the detection of recurrent disease in men having undergone primary radiotherapy, although the numbers were low (six patients). We know this group of men are often undertreated for salvage treatment, and frequently placed on hormonal therapy. Again, early knowledge of locoregional or distant recurrence is required to allow best case selection and thus avoid futile salvage surgery, and also to know who may benefit from salvage lymphadenectomy and treatment of distant oligometastatic disease, if required.
The false-positive rate result for 11C-acetate PET/CT of 24% is notable and concerning. This may lead to unnecessary intervention, or even withholding prostate bed radiation that may have been of benefit. In contrast the false-positive rate for 11C-choline and 68Ga-PSMA PET/CT is far lower, although false-positive PSMA studies may occur in benign conditions and non-prostate cancer tumours.
It should be acknowledged that a strength of this study was comparative histology in a proportion of patients, allowing true sensitivity and specificity to be determined [4]. This is important information, as it guides correct decision-making, and such information is lacking for many other prostate cancer imaging probes, including 68Ga-PSMA, where these data are urgently required.
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
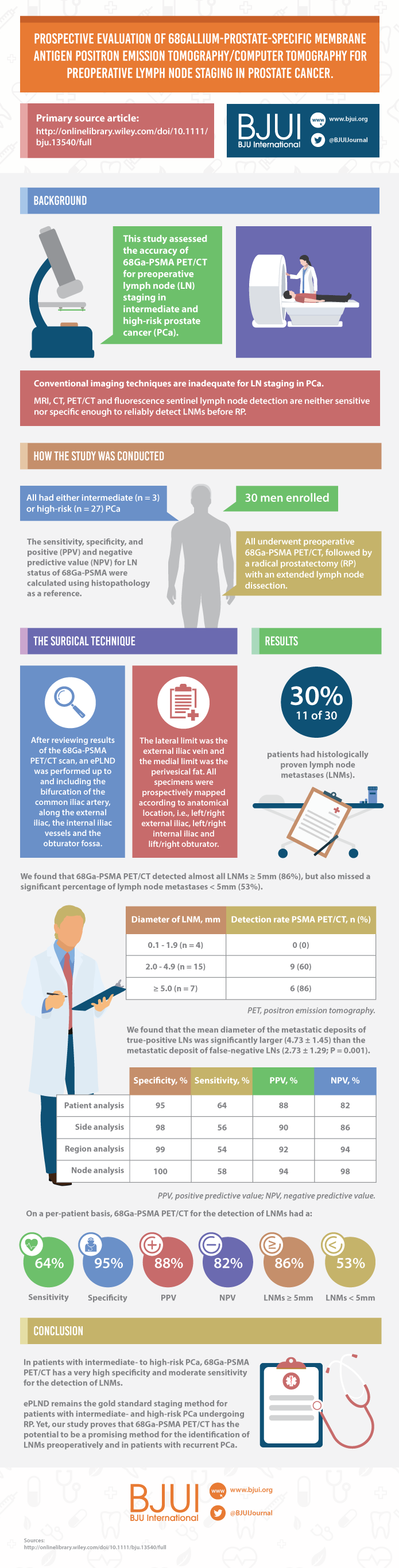
Prospective evaluation of 68Gallium-prostate-specific membrane antigen positron emission tomography/computed tomography for preoperative lymph node staging in prostate cancer
To assess the accuracy of 68Gallium-prostate-specific membrane antigen (68Ga-PSMA) positron emission tomography/computed tomography (PET/CT) for lymph node (LN) staging in intermediate- and high-risk prostate cancer (PCa).
Materials and Methods
From April to October 2015, 30 patients with intermediate- (n = 3) or high-risk (n = 27) PCa were prospectively enrolled. Patients underwent preoperative 68Ga-PSMA PET/CT. Both visual and semi-quantitative analyses were undertaken. Subsequently, all patients underwent radical prostatectomy (RP) with an extended pelvic lymph node dissection. The sensitivity, specificity, and positive (PPV) and negative predictive value (NPV) for LN status of 68Ga-PSMA were calculated using histopathology as reference.
Results
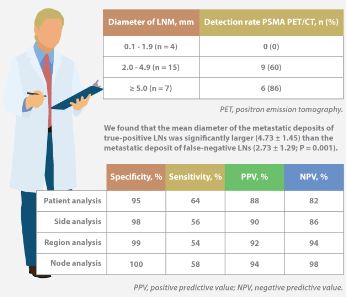
Eleven patients (37%) had lymph node metastases (LNMs); 26 LNMs were identified in the 11 patients. Patient analysis showed that 68Ga-PSMA PET/CT had a sensitivity of 64% for the detection of LNMs, its specificity was 95%, the PPV was 88%, and the NPV was 82%. In total, 180 LN fields were analysed. In the LN-region-based analysis, the sensitivity of 68Ga-PSMA PET/CT for detection of LNMs was 56%, the specificity was 98%, the PPV was 90% and the NPV was 94%. The mean size of missed LNMs was 2.7 mm. Receiver-operating characteristic curve analysis showed a high accuracy of maximum standardized uptake value (SUVmax) for the detection of LNMs, with an area under the curve of 0.915 (95% confidence interval 0.847–0.983); the optimum SUVmax was 2.0.
Conclusions
In patients with intermediate- to high-risk PCa, 68Ga-PSMA PET/CT had a high specificity and a moderate sensitivity for LNM detection. 68Ga-PSMA PET/CT had the potential to replace current imaging for LN staging of patients with PCa scheduled for RP.
The use of 68Ga-labelled prostate-specific membrane antigen (PSMA) positron-emission tomography (PET)/CT for staging prostate cancer in Australia has reached almost plague-like proportions. Despite what must be admitted is little high-level evidence to guide us in the accuracy or appropriateness of this imaging technique for either primary staging or prostate cancer recurrence, hundreds of these scans are being performed every week around Australia, and in many cases we simply do not know what to do with the results. We performed the first such scan at our centre in Melbourne in August 2014, and were soon receiving 10 requests per day, with patients waiting up to 3 months to be scanned. Fast-forward 2 years, and there are now eight centres offering PSMA PET/CT in Melbourne, a city of 4.5 million people. Scans can be obtained within 24 h of referral and costs have dropped to €500. A similar situation exists in Germany where this imaging method was pioneered [1], and interest is also growing in Belgium, Italy, India and a number of other countries (the USA being a notable exception). But do we really understand the impact of the decision to perform PSMA/PET scanning, and do we have enough evidence to guide us on the most appropriate setting for its use?
The current interest in PSMA PET/CT has been triggered by the development of small molecule ligands which bind to the extracellular domain of the PSMA molecule, leading to increased sensitivity and specificity when compared with conventional imaging [2]. Previously, the use of PET imaging for prostate cancer detection was greatly limited by the relatively poor performance characteristics of choline-based PET/CT, and limited availability and high costs associated with this type of imaging. The introduction of 68Ga-labelled PSMA PET/CT has addressed many of these concerns, although high-quality evidence is still lacking to help guide its most appropriate utility. The best data exist for identification of prostate recurrence in patients with biochemical recurrence (BCR) after previous definitive therapy. In our recent systematic review and meta-analysis of this topic, we reported pooled data on 1309 men with BCR undergoing PSMA PET/CT [3]. When stratified by PSA level post-radical prostatectomy, positive scans are reported in 42, 58, 76 and 95% of patients with PSA levels of 0–0.2, 0.2–1, 1–2, and >2 ng/mL, respectively. Fewer data exist for the role of PSMA PET/CT in the primary staging setting.
In this interesting paper from some of our Australian colleagues, van Leeuwen et al. [4] report their experience of PSMA PET/CT in the primary staging setting, in particular to evaluate the performance of PSMA PET/CT to evaluate lymph node positivity in patients with intermediate- and high-risk disease, scheduled for radical prostatectomy. A total of 30 patients underwent preoperative PSMA PET/CT, of which 27 were stratified as high risk, and all subsequently underwent radical prostatectomy and pelvic lymph node dissection. In total, 11 patients (37%) had histologically proven lymph node metastases. On a per-patient basis, PSMA PET had a sensitivity of 64%, specificity of 95%, positive predictive value of 88%, and negative predictive value of 82%. The average size of positive lymph nodes not detected by PSMA PET/CT was 2.7 mm; therefore, in this population of patients with predominately high-risk prostate cancer, PSMA PET/CT had very high specificity and moderate sensitivity for lymph node metastasis detection.
In a larger experience from Munich, Maurer et al. [5] compared pathology findings of 130 patients with intermediate- and high-risk disease who underwent radical prostatectomy and pelvic lymph node dissection, with preoperative PSMA PET/CT or PET/MRI findings. They reported similar sensitivity, specificity and accuracy of 65.9, 98.9 and 88.5%, respectively. On receiver-operating characteristic analysis, PSMA-PET performed significantly better than conventional imaging alone on patient and template-based analyses (P = 0.002 and <0.001, respectively).
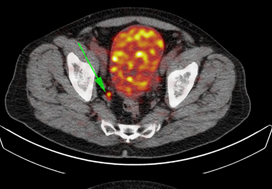
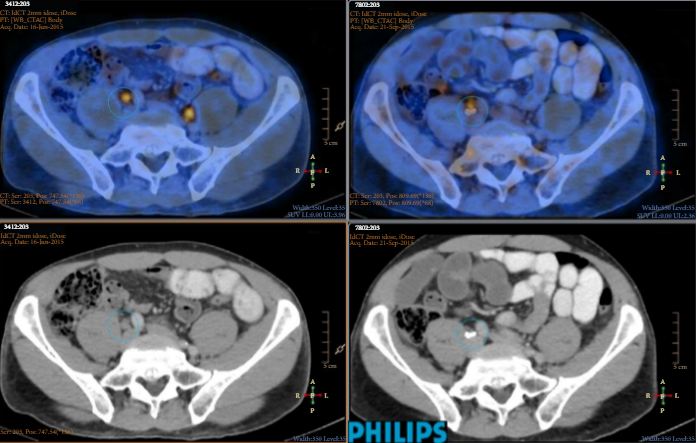
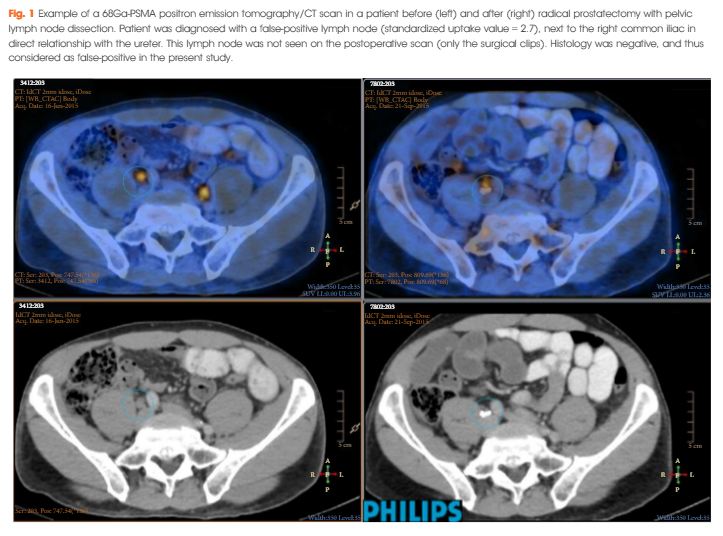
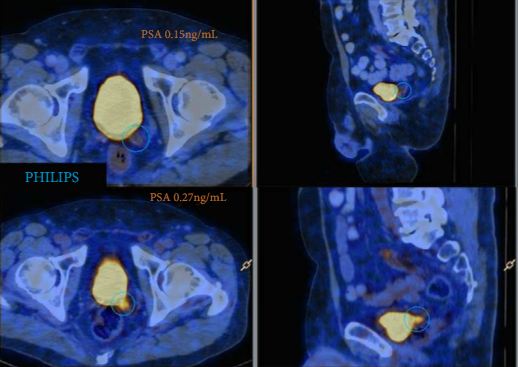
Just as there appears to be some clarity, however, in the role of PSMA PET/CT in patients with BCR, and in improving the detection of lymph node metastases preoperatively, there are many instances in which the high specificity of this scanning method leaves us in a decision-making quandary. As van Leeuwen et al. identified in their paper, and as we have frequently observed ourselves, PSMA PET/CT may identify prostate cancer in hitherto unidentified and unusual locations such as the mesorectum (Fig. 1). Disease may also be identified in quite distant locations despite relatively low PSA levels, thereby disrupting traditional management algorithms including the use of postoperative radiotherapy [6]. Should we alter patients’ management based on novel imaging, or should we assess the decision impact more formally in prospective studies? The answer should obviously be the latter, but the current plague of PSMA PET imaging means such decisions are already being taken in the absence of high-quality evidence.
Figure 1. 68Ga-labelled prostate-specific membrane antigen (PSMA) positron-emission tomography (PET)/CT in a 72-year-old man with biochemical recurrence after previous radical prostatectomy. His PSA level was 0.21 ng/mL and conventional staging including CT and bone scan showed no evidence of disease. PSMA PET/CT demonstrates intense avidity in an 11-mm mesorectal node near the recto-sigmoid junction on the left side. (a) CT demonstrates non-specific findings in area of subsequent avidity; (b) PSMA PET raw data demonstrating avidity in mesorectal node; (c) fused PSMA PET/CT image provides anatomical correlation; (d) coronal fused PET/CT image.
Nonetheless, PSMA PET imaging is here to stay, and will doubtless have a positive impact in improving decision-making in prostate cancer management as a result of the more accurate staging which it heralds. We must await more formal evaluation of the decision impact before defining the patient population who will benefit the most from this exciting imaging method.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
68Ga-PSMA has high detection rate of prostate cancer recurrence outside the prostatic fossa in patients being considered for salvage radiation treatment
To examine the detection rates of 68Ga-PSMA-positron emission tomography (PET)/computed tomography (CT) in patients with biochemical recurrence (BCR) after radical prostatectomy (RP), and also the impact on their management.
Materials and Methods
A total of 300 consecutive patients with prostate cancer (PCa) who underwent 68Ga-PSMA-PET/CT between February and July 2015 were prospectively included in the Prostate Cancer Imaging (ProCan-I) database. For the present analysis, we included patients with BCR (prostate-specific antigen [PSA] level ≥0.05 and <1.0 ng/mL) after RP, who were being considered for salvage radiation therapy (RT) according to the Faculty of Radiation Oncology Genito-Urinary Group (FROGG) guidelines. Two readers assessed each 68Ga-PSMA-PET/CT, and all positive lesions were assigned to an anatomical location. For each patient, the clinical and pathological features were recorded, their association with pathological 68Ga-PSMA uptake was investigated, and detection rates were determined according to PSA level.
Results
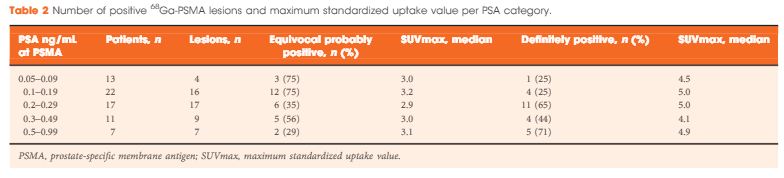
A total of 70 patients were included, and 53 positive 68Ga-PSMA lesions were detected in 38 (54%) patients. Among patients with PSA levels 0.05–0.09 ng/mL, 8% were definitely positive; the corresponding percentages for the other PSA ranges were as follows: PSA 0.1–0.19 ng/mL, 23%; PSA 0.2–0.29 ng/mL, 58%; PSA 0.3–0.49 ng/mL, 36%; and PSA 0.5–0.99 ng/mL, 57%. Eighteen of 70 patients (27%) had pathological 68Ga-PSMA uptake in the prostatic fossa, 11 (14.3%) in the pelvic nodes, and five (4.3%) in both the fossa and pelvic lymph nodes. Finally, there was uptake outside the pelvis with or without a lesion in the fossa or pelvic lymph nodes in four cases (8.6%). As a result of the 68Ga-PSMA findings there was a major management change in 20 (28.6%) patients.
Conclusions
68Ga-PSMA appears to be useful for re-staging of PCa in patients with rising PSA levels who are being considered for salvage RT even at PSA levels <0.5 ng/mL. These results underline the need for further prospective trials to evaluate the changes in RT volume or management attributable to 68Ga-PSMA findings.
In recent years there has been increasing interest in imaging recurrent or metastatic prostate cancer with positron-emission tomography (PET) radiotracers targeting prostate-specific membrane antigen (PSMA [1]). The majority of this work has been performed using urea-based small molecules labelled with gallium-68 (68Ga). Within this class of radiotracers, 68Ga-PSMA-11 (also known as 68Ga-PSMA-HBED-CC) has been the most widely studied. In this month’s edition of BJUI,van Leeuwen et al. [2] report on the clinical utility of 68Ga-PSMA-11 PET/CT in men with rising PSA levels after radical prostatectomy being considered for salvage radiation therapy. In their study, 70 patients with negative conventional imaging findings and a median PSA of 0.2 ng/mL (all <1 ng/mL) were imaged with 68Ga-PSMA-11 PET/CT prior to initiating treatment. On PSMA-targeted PET/CT, 53 lesions were detected in 38 (54%) patients. Perhaps most significant among their findings was that 28.6% of men had radiotracer uptake outside of the prostatic fossa leading to a major change in clinical management. In total, these data demonstrate the great potential of PSMA-targeted imaging, particularly in men with biochemically recurrent prostate cancer.
While a great deal of encouraging data with 68Ga-PSMA-11 has appeared in the medical literature, it is worth noting that several other small molecules that offer potential advantages over this agent have seen early clinical development. For example, PSMA-617 makes use of the DOTA chelation moiety in place of HBED-CC, allowing for a scaffold that can accommodate both diagnostic 68Ga and therapeutic lutetium-177 (177Lu) [3]. Additionally, our group has focused on fluorine-18 (18F)-labelled urea-based small molecules targeting PSMA, most recently 18F-DCFPyL [4]. 18F-labelled small molecules offer several potential advantages over those labelled with 68Ga. These include more favourable dosimetry allowing for higher injected radiotracer doses and lower-energy emitted positrons that have shorter path lengths to annihilation and therefore higher intrinsic spatial resolution [5]. Notably, a recent direct comparison of 68Ga-PSMA-11 and 18F-DCFPyL performed by Dietlein et al. [6] seems to confirm these advantages, having observed a higher rate of lesion detection as well as superior mean tumour-to-background ratios with the radiofluorinated compound. An additional advantage of 18F-labelled compounds is related to their longer half-life for radionuclide decay (109 vs 68 min for 68Ga). Given this difference, agents incorporating 68Ga typically require an on-site generator for radiotracer production, whereas 18F-based radiotracers can be produced en masse at a central site with a cyclotron and then delivered to remote locations via pre-existing distribution infrastructure (e.g. PETNET in the USA). Table 1 summarizes several relevant differences in the physical properties of 68Ga and 18F.
In summary, these are exceptionally exciting times for the study of PSMA-targeted imaging of prostate cancer. With continued radiotracer development and accompanying well-designed clinical trials, there is no doubt we can drastically improve the care of men with prostate cancer.
#BAUS15 started to gain momentum from as early as the 26th June 2014 and by the time we entered the Manchester Central Convention Complex well over 100 tweets had been made. Of course it wasn’t just Twitter that started early with a group of keen urologists cycling 210 miles to conference in order to raise money for The Urology Foundation.
Monday 15th June 2015
By the time the cyclists arrived conference was well under way with the andrology, FNUU and academic section meetings taking place on Monday morning:
The BJU International Prize for the Best Academic Paper was awarded to Richard Bryant from the University of Oxford for his work on epithelial-to-mesenchymal transition changes found within the extraprostatic extension component of locally invasive prostate cancers.
Donna Daly from the University of Sheffield received the BJUI John Blandy prize for her work on Botox, demonstrating reductions in afferent bladder signaling and urothelial ATP release.
Professor Reisman’s talk on ‘Porn, Paint and Piercing’ as expected drew in the crowds and due to a staggering 44% complication rate with genital piercings it is important for us to try to manage these without necessarily removing the offending article as this will only serve to prevent those in need from seeking medical attention.
With the worsening worldwide catastrophe of antibiotic resistance, the cycling of antibiotics for prevention of recurrent UTIs is no longer recommended. Instead, Tharani Nitkunan provided convincing evidence for the use of probiotics and D-Mannose.
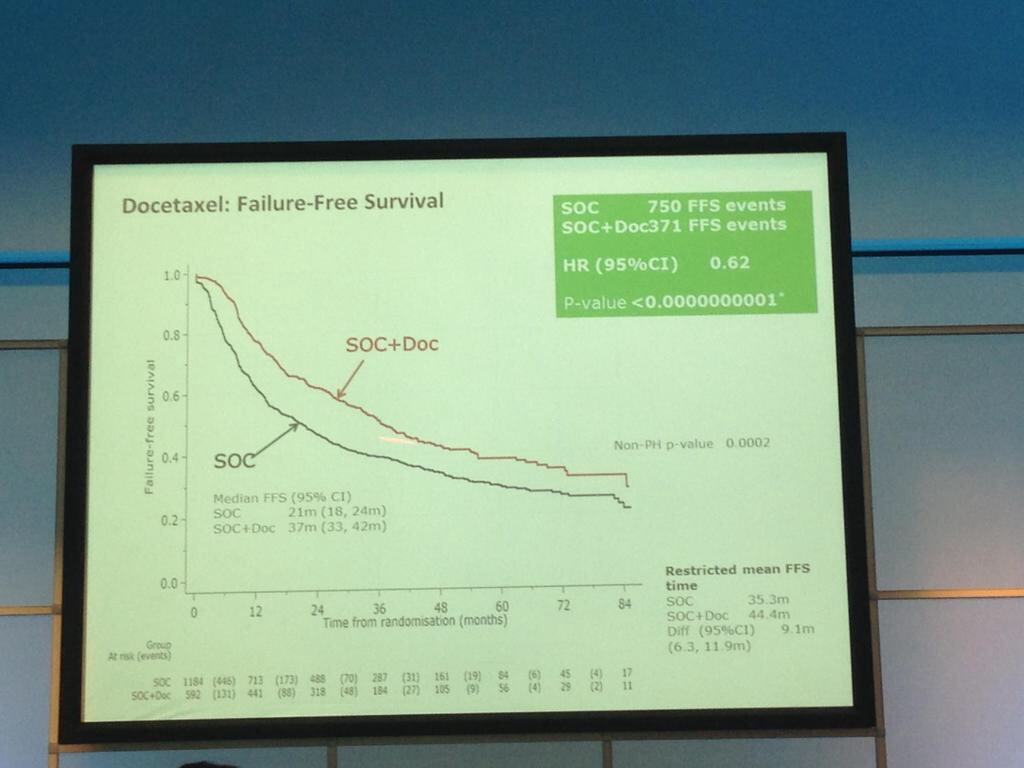
The afternoon was dominated by the joint oncology and academic session with Professor Noel Clarke presenting the current data from the STAMPEDE trial. Zolendronic acid conferred no survival benefit over hormones alone and consequently has been removed from the trial (stampede 1). However, Docetaxal plus hormones has shown benefit, demonstrated significantly in M1 patients with disease-free survival of 65 months vs. 43 months on hormones alone (Hazard ratio 0.73) (stampede 2). This means that the control arm of M1 patients who are fit for chemotherapy will now need to be started on this treatment as the trial continues to recruit in enzalutamide, abiraterone and metformin arms.
The evening was rounded off with the annual BAUS football tournament won this year by team Manchester (obviously a rigged competition!), whilst some donned the
lycra and set out for a competition at the National Cycle Centre. For those of us not quite so energetic, it was fantastic to catch up with old friends at the welcome drinks reception.
Tuesday 16th June 2015
Tuesday kicked off bright and early with Professor John Kelly presenting results from the BOXIT clinical trial, which has shown some benefit over standard treatment of non-muscle invasive bladder cancer, but with significant cardiovascular toxicity.
The new NICE bladder cancer guidelines were presented with concerns voiced by Professor Marek Babjuk over discharging low-risk bladder cancer at 12 months given a quoted 30-50% five-year recurrence risk. Accurate risk stratification, it would seem, is going to be key.
The President’s address followed along with the presentation of the St. Peter’s medal for notable contribution to the advancement of urology, which was presented to Pat Malone from Southampton General Hospital. Other medal winners included Adrian Joyce who received the BAUS Gold Medal, and the St. Paul’s medal went to Mark Soloway.
A plethora of other sessions ensued but with the help of the new ‘native’ BAUS app my programme was already conveniently arranged in advance:
‘Heartsink Conditions’ included pelvic and testicular pain and a fascinating talk by Dr Gareth Greenslade highlighted the importance of early and motivational referral to pain management services once no cause has been established and our treatments have been exhausted. The patient’s recovery will only start once we have said no to further tests: ‘Fix the thinking’
Poster sessions are now presented as ‘e-posters’, abolishing the need to fiddle with those little pieces of Velcro and allowing for an interactive review of the posters.
Pravisha Ravindra from Nottingham demonstrated that compliance with periodic imaging of patients with asymptomatic small renal calculi (n=147) in primary care is poor, and indeed, these patients may be better managed with symptomatic imaging and re-referral as no patients required intervention based on radiograph changes alone.
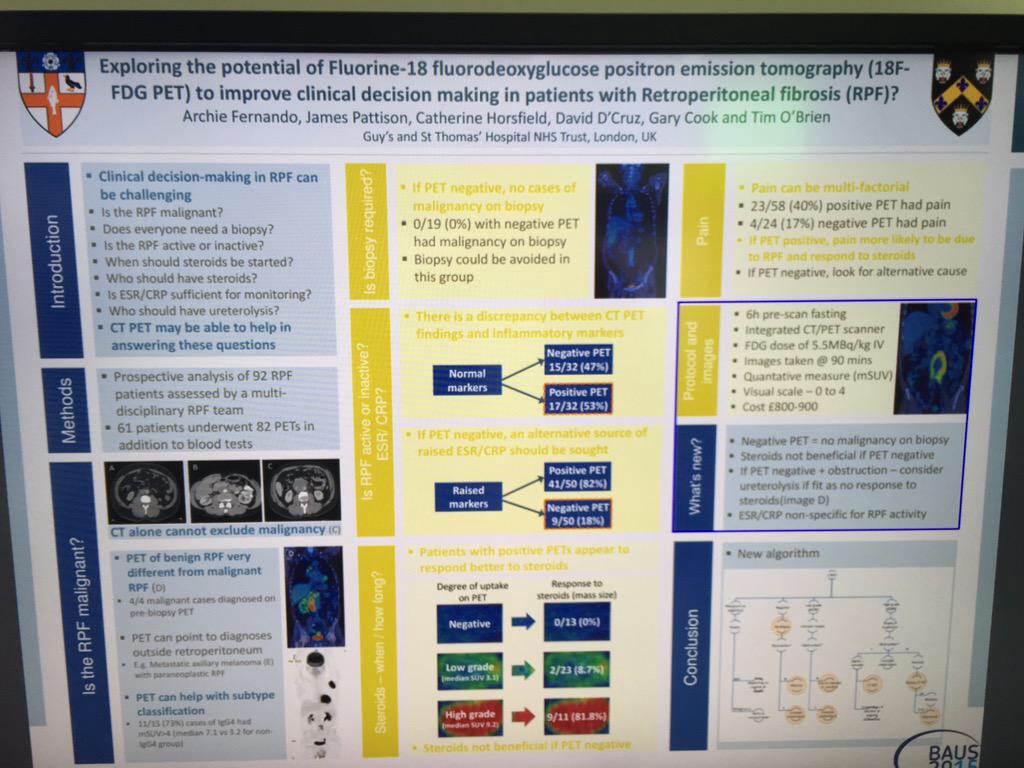
Archana Fernando from Guy’s presented a prospective study demonstrating the value of CTPET in the diagnosis of malignancy in patients with retroperitoneal fibrosis (n=35), as well as demonstrating that those with positive PET are twice as likely to respond to steroids.
Wednesday 17th June 2015
Another new addition to the programme this year was the Section of Endourology ‘as live surgery’ sessions. This was extremely well received and allowed delegates to benefit from observing operating sessions from experts in the field whilst removing the stressful environment and potential for risk to patient associated with live surgery. This also meant that the surgeon was present in the room to answer questions and talk through various steps of the operation allowing for a truly interactive session.
Wednesday saw multiple international speakers dominating the Exchange Auditorium:
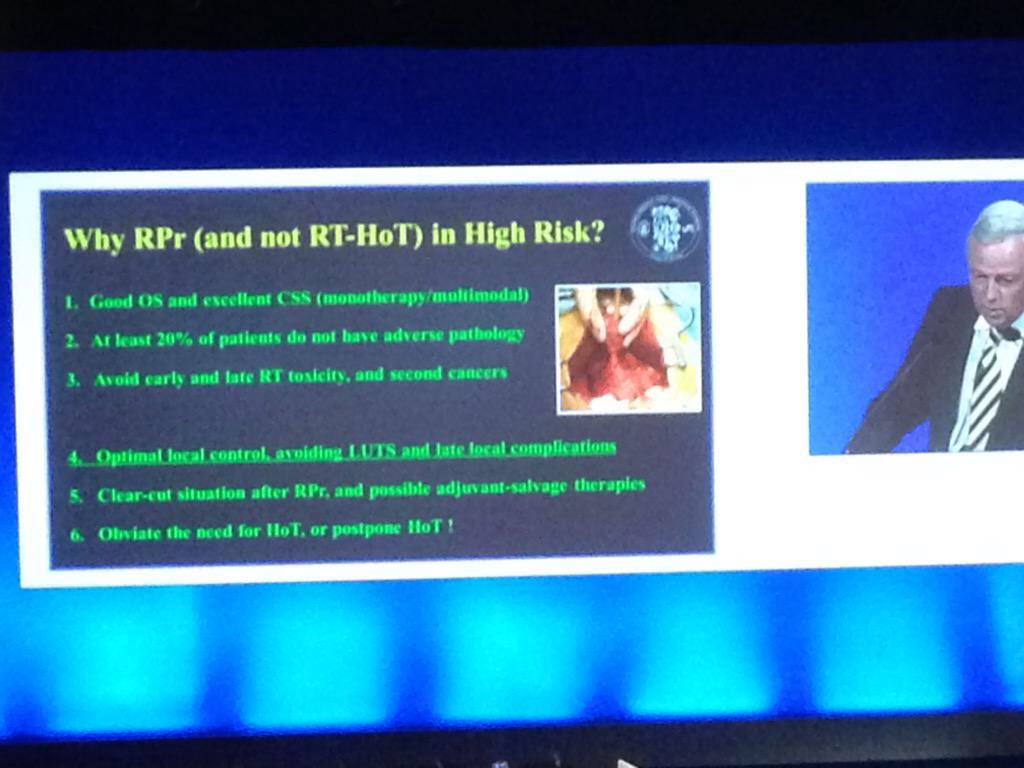
The BJU International guest lecture was given by Professor Hendrik Van Poppel: a heartfelt presentation describing what he believes to be the superiority of surgery over radiotherapy for high-risk localised prostate cancer.
The Urology Foundation presented the Research Scholar Medal to Ashwin Sachdeva from Freeman Hospital, Newcastle for his work on the ‘Role of mitochondrial DNA mutations in prostate carcinogenesis’. This was followed by an inspiring guest lecture by Inderbir Gill on ‘Robotic Urologic Oncology: the best is yet to come’ with the tag line ‘the only thing that should be open in 2015 is our minds’
Robotic Surgery in UK Urology: Clinical & Commissioning Priorities was a real highlight in the programme with talks from Jim Adshead and Professor Jens-Uwe Stolzenburg focussing on the fact that only 40% of T1a tumours in the UK were treated with partial (as opposed to radical) nephrectomy, and that the robot really is the ‘game-changer’ for this procedure. Inderbir Gill again took to the stage to stress that all current randomised trials into open vs. robotic cystectomy have used extracorporeal reconstruction and so do not reflect the true benefits of the robotic procedure as the dominant driver of complications is in the open reconstruction.
These lectures were heard by James Palmer, Clinical Director of Specialised Commissioning for NHS England who then discussed difficulties in making decisions to provide new technologies, controlling roll out and removing them if they show no benefit. Clinical commissioning policies are currently being drafted for robotic surgery in kidney and bladder cancer. This led to a lively debate with Professor Alan McNeill having the last word as he pointed out that what urologists spend on the robot to potentially cure cancer is a drop in the ocean compared with what the oncologists spend to palliate!
Thursday 18th June 2015
The BJU International session on evidence-based urology highlighted the need for high-quality evidence, especially in convincing commissioners to spend in a cash-strapped NHS. Professor Philipp Dahm presented a recent review in the Journal of Urology indicated that the quality of systematic reviews in four major urological journals was sub-standard. Assistant Professor Alessandro Volpe then reviewed the current evidence behind partial nephrectomy and different approaches to this procedure.
Another fantastic technology, which BAUS adopted this year, was the BOD-POD which allowed delegates to catch-up on sessions in the two main auditoria that they may have missed due to perhaps being in one of the 21 well designed teaching courses that were available this year. Many of these will soon be live on the BAUS website for members to view.
The IBUS and BAUS joint session included a lecture from Manoj Monga from The Cleveland Clinic, which led to the question being posed on Twitter: ‘Are you a duster or a basketer?’The audience was also advised to always stent a patient after using an access sheath unless the patient was pre-stented.
The updates session is always valuable especially for those studying for the FRCS (Urol) exam with far too many headlines to completely cover:
Endourology: The SUSPEND trial published earlier this year was a large multi-centre RCT that showed no difference in terms of rates of spontaneous passage of ureteric stone, time to stone passage or analgesic use between placebo, tamsulosin and nifedipine. There was a hot debate on this: should we be waiting for the meta-analysis or should a trial of this size and design be enough to change practice?
Oncology-Prostate: The Klotz et al., paper showed active surveillance can avoid over treatment, with 98% prostate cancer survival at 10 years.
Oncology-Kidney: Ellimah Mensah’s team from Imperial College London (presented at BAUS earlier in the week) demonstrated that over a 14-year period there were a higher number of cardiovascular-related admissions to hospital in patients who have had T1 renal tumours resected than the general population, but no difference between those who have had partial or radical nephrectomy.
Oncology-Bladder: Arends’s team presented at EAU in March on the favourable results of hyperthermic mitomycin C vs. BCG in the treatment of intermediate- and high-risk bladder cancer.
Female and BPH: The BESIDE study has demonstrated increased efficacy with combination solifenacin and mirabegron.
Andrology: Currently recruiting in the UK is the MASTER RCT to evaluate synthetic sling vs. artificial sphincter in men with post-prostatectomy urinary incontinence.
Overall BAUS yet again put on a varied and enjoyable meeting. The atmosphere was fantastic and the organisers should be proud of the new additions in terms of allowing delegates to engage with new technologies, making for a memorable week. See you all in Liverpool!
Rebecca Tregunna, Urological Trainee, West Midlands Deanery @rebeccatregunna