Article of the week: Using data from an online health community to examine the impact of prostate cancer on sleep
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to this post, there is an editorial written by a prominent member of the urological community. Please use the comment buttons below to join the conversation.
If you only have time to read one article this week, we recommend this one.
Using data from an online health community to examine the impact of prostate cancer on sleep
Rebecca Robbins*, Girardin Jean‐Louis†, Nicholas Chanko†, Penelope Combs†, Nataliya Byrne†‡, Stacy Loeb†‡
*Division of Sleep and Circadian Disorders, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA, †Department of Population Health, New York University (NYU) School of Medicine, and ‡Department of Urology, NYU School of Medicine and Manhattan Veterans Affairs, New York, NY, USA
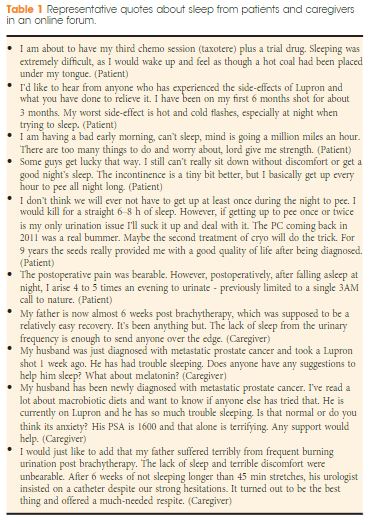
Previous epidemiological studies have examined the relationship between sleep disturbances and prostate cancer risk and/or survival. However, less has been published about the impact of sleep disturbance on quality of life (QoL) for prostate cancer survivors and their in home caregiver. Although prostate cancer presents numerous potential barriers to sleep (e.g., hot flashes, nocturia), current survivorship guidelines do not address sleep. In addition to its impact on QoL, sleep disturbances also mediate the impact of cancer status on missed days from work and healthcare expenditures.
A broader examination of contributors to poor sleep in prostate cancer, and the impact on patients and caregivers would be an important contribution to raise awareness of these issues in the medical community, improve survivorship care, reduce healthcare costs, and stimulate future research. The objective of our letter is to analyse sleep barriers reported by patients with prostate cancer and caregivers posted to a large online health community. You can check lot of article on coolsculptny related to health.