Editorial: A urologists’ guide to the multi-parametric magnetic resonance imaging (mpMRI)-galaxy
The rise of multi-parametric MRI (mpMRI) for the assessment of patients with suspicion of prostate cancer has led to an enormous shift in the practice of every urologist dealing with frontline diagnostics [1].
At the same time, researchers and industry have identified acres of fruitful soil to place the seeds of their respective interests, sometimes in collaboration with each other producing valuable contributions to this shift in practice, sometimes taking benefits by merely assimilating themselves or their product to this development.
Both, the speed of change and the extent of proliferation, make it almost impossible for by-standing clinicians to keep up and filter the evidence-based essence for their local practice.
There are three important issues that need to be considered:
1 The Quality of mpMRI
The development of mpMRI for prostate assessment occurred over the last decade with well-known leaders pushing the frontiers. Their research benefitted from their individual experience of interpreting and reporting MRIs. This is then reflected in their outcomes in form of cancer detection rates and accuracy. More recently we have identified that achieving these results must involve standardisation of MRI protocols and reading [2-4], systematic training in validated courses and a significant learning curve [5]. The latter is only possible to achieve if the practice is embedded in a collaborative team of radiologists, pathologists and urologists. But even then it may be impossible for local teams to deliver the published accuracy, and the urologists and radiologists need to be mindful of that when counselling patients using mpMRI in their local environment.
2 The Technical and Clinical Validity of MRI-Based Biopsies
Transperineal vs transrectal, targeted alone vs targeted with systematic, cognitive vs fusion biopsies – these are the key debates surrounding the application of mpMRI into the urologists’ armamentarium. For none of them there is or will be a unified answer.
Transrectal approaches suit office-based provision of primary diagnostics in many European and USA health economies; although purists can say that the increasing risk of sepsis from antibiotic-resistant bacteria is not acceptable. But, favouring the less infection-prone transperineal approaches will have impact on theatre capacities even in a hospital-based health system like the UK.
Considering the current real-time quality of mpMRI, systematic biopsies in addition to targeted ones are still necessary. Urologists as a group have to come to an agreement about what is acceptable as a remaining risk when reducing or omitting systematic cores.
Cognitive targeting has been shown to be highly accurate; yet, fusion may offer standardisation and reduce user dependency. Not all fusion software on the market has undergone a thorough validated technical development and clinical accuracy evaluation. Peer-reviewed publications can be found involving the systems Urostation-Koelis, Uronav-Philips, Artemis and BiopSee-Medcom.
3 Translation into Clinical Practice
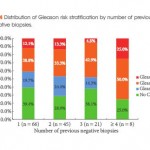
The positioning of the mpMRI within the assessment algorithm is key to optimise the benefit. Use as a pre-biopsy assessment tool may allow omission of further biopsies in some patients or facilitate targeting [6]. However, an established skill in the use of mpMRI and mpMRI-based biopsy is essential. Many UK centres have started the use of mpMRI in their practice further downstream in patients with persistent suspicion after negative first biopsies with good results for patients. It is already part of guidance that active surveillance should involve the use of MRI [1]. Some leading centres advocate that the diagnosis should be confirmed by MRI-based targeted and systematic biopsies.
Knowing that mpMRI will improve the accuracy of our assessment, we need to re-consider follow-up protocols. Increased certainty should be reflected in an improved cancer-related outcome, better patient experience and reduction in costs for the health system.
Prostate mpMRI as part of the urologists’ armamentarium is here to stay. A standardised team- and evidence-based approach will allow us to remain in control of the destination it leads us to.