Editorial: Quality improvement in cystectomy care with enhanced recovery (QUICCER) study
Enhanced recovery after surgery (ERAS) is a multidisciplinary, multi-element care pathway approach that aims to standardise and improve perioperative management. Since the first publication on ERAS for radical cystectomy in the BJUI in 2008, the literature on this important factor in postoperative management of patients undergoing major surgery in the field of urology is rather scarce and mainly in form of reviews [1]. This clearly reflects the very slow adoption of this approach, the reasons for which remain unclear.
Baack Kukreja et al. [2] in this issue of BJUI performed an analysis of sequential patients, before and after introduction of an ERAS protocol in their institution, using a propensity matched approach. The length of stay (LOS) could be reduced significantly from 8 to 5 days without increasing the rate of complications or increasing the number of readmissions or emergency department visits. The rate of readmissions is comparable to other published reported series. The difference in LOS of 3 days with an ERAS approach is impressive. However, the parameter of LOS has to be interpreted in the context of the medical system of each country in itself, as many factors may influence this parameter. The data presented indicates that there was no biased drive to discharge patients earlier in the study context.
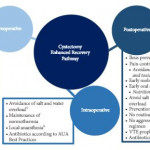
The ERAS programme presented here included preoperative counselling and intra- and postoperative precautions and interventions. Preoperative counselling focused on information on surgery and the handling of the stoma if needed. Patients were assessed for medical and socioeconomic factors that might have an influence on anaesthesia/surgery outcome, recovery, and management after discharge. As foreseen by ERAS, patients received probiotics and preoperative carbohydrate loading [3, 4].
Apart from the LOS, one of the major findings of this study [2] was a distinct decrease in gastrointestinal complications, such as ileus, which is not surprising as this is one of the declared goals of ERAS, which was first introduced in colorectal surgery.
The reported decrease of myocardial infarction is another interesting finding. There is no difference in American Society of Anesthesiologists score between the two groups. However, there is a tendency to more blood transfusions in the cystectomy enhanced-recovery pathway group in the study. The current debate on whether blood transfusions may have a negative effect on oncological outcomes might have an influence on this eventually. Astonishingly, fluid management was not different between the two groups despite the declared goal to avoid salt and water overload. The use of pulse pressure variation or an oesophageal Doppler probe to guide fluid management might be complemented by restrictive deferred hydration combined with preemptive noradrenaline infusion [5, 6].
After discharge patients did not require home i.v. fluid administration and were able to drink at least 1 L. They did not require more support at home than the control group.
The authors are to be complemented for implementing an ERAS protocol and evaluating the effect in a scientific manner. Some of the findings are confirmatory of other studies, some are novel and worthy of further analysis, while others suggest a potential for further improvement. The results of this study [2] clearly indicate the usefulness and validity of an ERAS protocol and the need to implement and further develop such an ERAS approach in everyday urological practice.