Article of the Week: With a previous negative prostate biopsy and a suspicious lesion on MRI, is a 12-core biopsy still necessary in addition to a targeted biopsy?
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Art R. Rastinehad , discussing his paper.
If you only have time to read one article this week, it should be this one.
In patients with a previous negative prostate biopsy and a suspicious lesion on magnetic resonance imaging, is a 12-core biopsy still necessary in addition to a targeted biopsy?
OBJECTIVES
To evaluate the performance of multiparametric magnetic resonance imaging (mpMRI) in predicting prostate cancer on repeat biopsy; and to compare the cancer detection rates (CDRs) of MRI/transrectal ultrasonography (TRUS) fusion-guided biopsy with standard 12-core biopsy in men with at least one previous negative biopsy.
PATIENTS AND METHODS
We prospectively enrolled men with elevated or rising PSA levels and/or abnormal digital rectal examination into our MRI/TRUS fusion-guided prostate biopsy trial. Participants underwent a 3 T mpMRI with an endorectal coil. Three radiologists graded all suspicious lesions on a 5-point Likert scale. MRI/TRUS fusion-guided biopsies of suspicious prostate lesions and standard TRUS-guided 12-core biopsies were performed. Analysis of 140 eligible men with at least one previous negative biopsy was performed. We calculated CDRs and estimated area under the receiver operating characteristic curves (AUCs) of mpMRI in predicting any cancer and clinically significant prostate cancer.
RESULTS
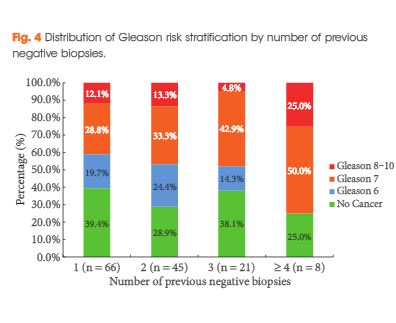
The overall CDR was 65.0% (91/140). Higher level of suspicion on mpMRI was significantly associated with prostate cancer detection (P < 0.001) with an AUC of 0.744 compared with 0.653 and 0.680 for PSA level and PSA density, respectively. The CDRs of MRI/TRUS fusion-guided and standard 12-core biopsy were 52.1% (73/140) and 48.6% (68/140), respectively (P = 0.435). However, fusion biopsy was more likely to detect clinically significant prostate cancer when compared with the 12-core biopsy (47.9% vs 30.7%; P < 0.001). Of the cancers missed by 12-core biopsy, 20.9% (19/91) were clinically significant. Most cancers missed by 12-core biopsy (69.6%) were located in the anterior fibromuscular stroma and transition zone. Using a fusion-biopsy-only approach in men with an MRI suspicion score of ≥4 would have missed only 3.5% of clinically significant prostate cancers.
CONCLUSIONS
Using mpMRI and subsequent MRI/TRUS fusion-guided biopsy platform may improve detection of clinically significant prostate cancer in men with previous negative biopsies. Addition of a 12-core biopsy may be needed to avoid missing some clinically significant prostate cancers.