

Are you ready to go to prison on a manslaughter charge?
 Which of us fancies ending their career with a spell in the clink? Being a surgeon in the UK has just become a whole lot riskier. We all know that in our job success can add extra years to our patients lives, by contrast, failure, can result in significant harm, or, in the worst circumstances, death. We all do our best, but sometimes things don’t work out. The sentence of two and a half years in prison for Mr David Sellu, who was referred a patient who developed peritonitis after an orthopaedic operation and subsequently died, smacks of injustice, and sends a shiver down the spine of all of us surgeons, who work hard on behalf of our patients, but who cannot always guarantee success.
Which of us fancies ending their career with a spell in the clink? Being a surgeon in the UK has just become a whole lot riskier. We all know that in our job success can add extra years to our patients lives, by contrast, failure, can result in significant harm, or, in the worst circumstances, death. We all do our best, but sometimes things don’t work out. The sentence of two and a half years in prison for Mr David Sellu, who was referred a patient who developed peritonitis after an orthopaedic operation and subsequently died, smacks of injustice, and sends a shiver down the spine of all of us surgeons, who work hard on behalf of our patients, but who cannot always guarantee success.
The case is reported in detail in the latest bulletin of the Royal College of Surgeons (Ann R Coll Surg Engl (Suppl) 2014; 96: 112-113). It appears that the main problem was a delay in taking the patient to theatre because of the difficulty in finding an anaesthetist; a problem that cannot be reasonably be blamed upon the surgeon himself. If prosecutions for manslaughter become more frequent in circumstances similar to the Sellu case, we may all have to develop new defensive strategies. Madison Branson Lawyers are experts in the area of Proceeds of Crime and Confiscation Law. The prospect of ending an otherwise unblemished career in a prison cell as a result of an unfortunate clinical mishap might deter many from entering the profession in the first place. How should we react to the very sad scenario?
Roger Kirby, The Prostate Centre, London

I read the article in the telegraph: according to it, Dr Sellu delayed the operation because he had to finish his private practice !? Shivers down my spine. What are we talking about?
If what is told in the telegraph holds true it’s terrible and I judge it a tremendous malpractice deserving such a conviction. We are doctors and must care for patients; our private practice comes next.
The information given in the Telegraph was incorrect
Mr Sellu was convicted for manslaughter caused by his gross negligence to his patient. To warrant a conviction, a healthcare professional’s breach of the duty of care to the patient has to (i) have been so grossly negligent AND (ii) show such a disregard for the life and safety of others, as to be worthy of criminal conviction. In addition, the test for proving gross negligence is much harder to pass than the test for “regular” negligence. Furthermore, the legal standard of proving gross negligence is “beyond all reasonable doubt” and not the lesser “balance of probabilities” used in civill negligence cases. Proving manslaughter by gross negligence is a very tall order. Also, the law under which Mr Sellu was convicted is not new. For all these reasons; (i) healthcare professionals are rarely convicted for manslaughter by gross negligence and (ii) the Sellu case is notable for its rarity, not its novelty. The Judge’s sentencing remarks are available online are are worth reading. DSU
Thanks, I don’t think that there is any question that David Sellu made an error in the timing of the procedure, although I understand that was difficulty finding an anaesthetist. I have been arguing for ages that private hospitals should have an on-call anaesthetist for emergencies such as this! The real issue is whether or not a custodial sentence was appropriate. Those who are interested can read the summary of the judgement:
https://www.judiciary.gov.uk/Resources/JCO/Documents/Judgments/r-v-sellu-sentencing-remarks.pdf
The judges sentencing remarks make chilling reading! https://www.judiciary.gov.uk/Resources/JCO/Documents/Judgments/r-v-sellu-sentencing-remarks.pdf.
Whatever actually happened, and there appear to be many discrepancies, David Sellu appears to have contravened a fundamental tenet of medical practice in that there was a lack of documentation of the care provided. As is well known, “if it isn’t written down it didn’t happen”, and therefore the failure to adequately document his visit and instructions in this critically sick patient was incomprehensible.
Prof Kirby’s suggestion that the patient died due to the lack of availability of an anaesthetist is interesting as there was no mention of it by the judge. Delays were probably due to the failure of the surgeon to recognise the severity of the condition and his decision to order a CT scan. He should have been looking for an anaesthetist on Thursday evening and not some 18hours later.
The decision not to suspend the sentence does however appear to be unnecessarily harsh and I suspect he has been used by the judiciary to send a message to the medical profession.
Interestingly, there is now a blog put up my the David Sellu support group:
https://davidsellu.org.uk/ and I understand that the whole case is to be reviewed in detail in the publication of the Medical Protection Society, which will be available in mid-May. On the blog mentioned above the point is made that there was an “error chain” leading up to the sad loss of life and it seems harsh that one individual is now paying the price for a series of mistakes.
Even across the miles this is indeed worrying . Clearly it highlights the need to accurately document all steps in the care of a patient . Obviously delays in assessing and operating on an acutely unwell patient in unacceptable. In this courts eyes , if that contributes to the death of a patient it is deemed grossly negligent and now worthy of a prison term. Obviously this is a major concern for all surgeons who may not always be in a position to acutely assess a patient if they are performing another procedure. Obviously this highlights the need for defensive strategies including adequate documentation in notes , having a low threshold to investigate out of hours ( including calling in radiologists, surgeons or physicians as required ) , ensuring prioritisation and full assessment of any unwell patient before any routine scheduled elective surgery ,and I suspect now ensuring adequate consultant cover in case an emergency aries when a surgeon is not immediately available to assess a patient . I would agree incarceration is an extremely harsh penalty and may well make anyone considering a medical and in particular a surgical career , reconsider their career choice.
This case is indeed frightening. In the US there have been few such verdicts and the ones that I know of were clearly egregious. As plaintiff attorneys become more aggressive and monetary limits are imposed in many states, these attorneys are turning to more creative ways of making money. Often they are trying to use fraud instead of malpractice to win cases stating that the contract with a patient tacitly included guarantees of successful outcomes. These cases are not covered by malpractice insurance. If we were to add manslaughter to the mix, we as surgeons would have to reconsider our practices and confine our care to only the most elective and non complicated cases leaving much of the public without emergency care. Viewing the case of Mr Sellu through the retrospectoscope is clearly unfair and inaccurate but should give us all reason to worry.
What a shocking sentence for this surgeon. There have only been 3 custodial sentences in the last 100 years or so involving similar cases. BUT… Doesn’t look good if you read the RCS document and judges sentencing.
The key learning points seems to be poor communication, lack of urgency, terrible lack of documentation and lack of openness and honesty due to changing his story.
Ironically if he was in an NHS hospital then the CT and antibiotics probably would have been sorted by the team. Privately there isn’t that backup. Maybe he should have just been transferred that first night. The P-POSSUM score for peri operative mortality may well have resulted in the predictive score for survival dropping significantly due to the delay.
He failed to recognize the seriousness of the situation and react accordingly but was probably reassured given the history of a knee operation that serious bowel pathology was unlikely.
He didn’t ask for the referral to him and probably could have done without it that night but having seen the case had a duty of care to the patient and unfortunately had a heavy schedule the next day. Working alone privately in this situation is highly stressful in these circumstances.
Much to learn from and take note of but hopefully most of us would be able to react differently. However jail really seems a step too far.
I have read with interest the issues around this matter. We all agree that the best standard of care must be applied to the management of each and every patient, whether NHS or Private. There are more checks and balances in the NHS where there is usually a tier of staff assisting with patient care. In Private Practice the entire responsibility lies with the Consultant under whose care the patient rests. Thus the Private Practitioner must be more diligent. This particularly applies when recording each aspect of the patient’s care. “If it isn’t written down it didn’t happen”. There are still many practitioners who do not record each patient visit and this is a failing in care. Acting expeditiously is of course necessary when acute situations arise and there is no excuse for delay. With regard to this case however, if there is a risk of a custodial sentence when things go wrong, then it is possible we as a body will become risk averse thus denying a patient primary treatment or being overcautious with the added negative effects. The whole issue of the merits or demerits of medical negligence and its relationship with the potential for criminal conviction needs to be vigorously discussed. We must do our best to avoid this ever happening to well-meaning and hard working professionals.
We all make mistakes and if it results in harm to the patient we never forget it & learn. Our feelings of guilt are punishment in itself. We do not know enough about this case to make any judgement to know if the punishment was fit for the crime, but one thing is for sure, the surgeon will have felt great remorse. A fine example of how surgeons feel when things go wrong is in Henry Marsh’s book DO No Harm, published by Orion books ISBN 978-0-2978-6987-0, I commend it to you. It tells of the experiences of a neurosurgeon. What I have learnt over the years is to be very honest and say sorry as soon as possible.
Interesting yet alarming. One fears malpractice accusations for many reasons but not for fear of jail.
It is clear that if one takes on a case you have to commit to it. This is a very personal commitment privately as you are generally not a team. Accept the referral, see the patient and it is very much your responsibility.
Common themes of need for good communication, documentation and of course honesty.
I feel this has not been fairly concluded but moving forward it is clear that adherence to the basics are probably protective. This should not therefore alter practice and make us risk averse. A very hard lesson for Mr Sellu and a very good lesson for everyone else.
It would be terribly easy to be sanctimonious about this case, without knowing the details. The bottom line is that if someone has been found to have acted in a negligent manner, one has to accept the consequences. In this instance, the judge has sentenced the surgeon to a prison sentence, which was obviously considered to be the appropriate sentence. I think that the fact that the surgeon has been sent to jail is catastrophic for the person involved and the consequences for him are serious and far-reaching. If the deceased patient’s family decide to take a civil suit against the surgeon or physician, this is a potential end-point.
At last some heartening news about David Sellu! I gather that today he has been moved to Hollesley Bay open prison in Suffolk. This hopefully will give him heart and hope. I am worried that this case will give all surgeons pause about accepting emergency referrals from their colleagues. If one’s freedom is ultimately in jeopardy, why would one want to try and help out? Defensive medicine could work out to be very expensive!
There, for the Grace of God, go the rest of us…..for the moment. This could happen to any one of us at anytime. In the same way that we may cause a fatal motor accident. We do not set out to do these things that may bring us down. They happen. On reflection we may have wished we had done things differently, We are all very busy with too many strings pulling at us and we have to prioritise timings. There are no winners here,: not for the patient, not for the family and not for the surgeon. There are only losers. It is important that the implications of this case are widely disseminated through educational fora to all of us who practice medicine and surgery. It is likely that we will see more rulings like this. We all need to be vigilant in preventing such catastrophes and we need ongoing education and infrastructures and pathways to ensure that we have done all we can do to prevent disaster. Even with that, disaster will happen. The judgement, however, may be different if we have had such education, infrastructure and have adhered to validated pathways of care. God bless us all.
A great shame and a personal tragedy that a man who has spent his life in the service of others has to end up like this. And indeed, there but for the Grace of God go we all. We do make errors of judgement and sometimes with very serious consequences. But the way forward in these situations is complete and utter candour, no matter how painful that may be! And in this age of the dreaded internet, Twitter and facebook, that can be very painful indeed. Look at the new malign force of revenge porn and you will see haw devastating an electronic media campaign against you can be!
I don’t think we have all the facts of the case but there are principles to underline here.
In private practice, you work alone and carry the entire can. If you are busy you will struggle to manage a very sick patient at night and perhaps they are better off in the NHS. Also elective procedures are just that, elective. They can and must wait for emergencies especially life threatening ones.
When things go wrong, make immediate and copious accurate dated and timed notes. You wont remember the sequence of events in 12 months time.
And approach the family and friends honestly, demonstrate remorse and sympathy. And I think above all, be honest.
Yes this is thought provoking and it is worrying. Maybe we all need to reconsider our work life balances and learn to say “No” just a bit more often!
This is a truly tragic case for all concerned and perhaps one of the most surprising features is the very limited amount of comment there has been about this in the medical and lay press.
This case may have some impact on the management of patients in the NHS but it should have a really significant impact on private medical practice. It should be compulsory reading for all private hospital CEOs.
There are virtually no protocols for the management of the emergency patient in private hospitals (where such cases usually occur as the result of complications of another elective operation). Not all private hospitals have planned out of hours rotas for anaesthetists and radiologists and sometimes there can be difficulty in accessing emergency theatres at night.
I completely agree with the comments of others that we have to get better about making daily timed records in all private patients notes and that these notes should be extremely detailed in all occasions where complications occur.
We need a low threshold for transferring private patients to an appropriate NHS facility if high dependency care is not available and I suspect there are many hospitals where the level of middle grade support falls far below that which we take for granted in the NHS.
This is indeed a horrifying outcome on all counts, particularly for all of this involved. But a custodial sentence seems to have little logic, only prowess for the lawyers, and detriment to the practice of medicine in the UK. We all deal with cases like this on a regular basis, and there are always alternative strategies. Clinical decisions are based around history, examination, appropriate imaging, clinical diagnostic skills and timing of interventions. The benefit of the Lawyers hindsight has always intrigued me. If I also knew the “actual” outcome, before the intervention, I too would change my strategy before the intervention, if the known outcome was adverse! Unfortunately, all of our daily decisions are based on the information in front of us, without the knowledge of actual outcome! I am sure that all of us would change many things in our lives based on what we know now, and the benefit of a lifetime of hindsight! It appears that a custodial sentence adds nothing positive for medicine or society in this particular case. It only serves to appease emotional guilt and the lawyers pockets. As regards the delay being due to the availability of anaesthesia, I would add that this patient had been anaesthetised for his original operation, so an anaesthetist was already involved in has care. The NHS has “On Call” anaesthesia providers available 24 hours a day seven days a week, and they are paid for their skilful service. Acute immediate care is not recognised by the major Private Health Insurance companies in the UK, nor many private hospitals, and there is as such no “on call” equivalent. If private practice requires an immediate anaesthesia “On Call” service, it will need to be properly recognised and funded appropriately. We all make “errors of judgement” on a daily basis. Not repeating the errors, together with reflective and positive learning from the errors is important. Pencils have rubbers attached to them for a reason. We allow custodial sentences for errors of judgement in Medicine at society’s peril.
Writing as a layperson aware of our over-crowded prisons, what is the point of a custodial sentence? Surely there are better options?
I do not believe that David Sellu has been jailed for ‘an error of judgement’, but because he has been convicted by a jury of manslaughter. As Mr Underhill reminds us, this required proof of gross negligence – not the ‘ordinary’ negligence debated in most medico legal cases – plus a disregard for the life and safety of his patient. Together, they led to his conviction in a criminal court of manslaughter. It is not therefore something that is likely to happen to any other practising surgeon unless he/she behaves as Mr Sellu did.
The tragedy here is mainly for the family who lost their relative following knee surgery, primarily because of the inept behaviour of the surgeon who accepted the responsibility for his care.
A lethal combination of bad clinical management, inappropriate delays, no clinical notes and no communication with others was compounded by evasion and possible lying. This is what seem to have landed him with a criminal conviction and imprisonment. I am sure no-one is defending this behaviour, and it is therefore extremely unlikely that we need to consider practising ever more ‘defensive medicine’ or that it should put people off practising surgery.
As far as suspending the sentence, the judge stated that Sellu’s counsel “realistically accepts that the only sentence I can pass is one of custody”. He seems not to have opted for suspension because of the “circumstances”. Judging from his statement, it would seem to be the lying, not only in court but to the coroner and to Professor Empey’s investigation which led to implementation of imprisonment.
It is true however that in this country emergency patients in the private sector may be at greater risk than in the NHS. As Julian Shah mentioned, private practitioners need to be more diligent. There is rarely the supporting infrastructure we are more used to in the NHS. Secondly, surgeons should be more ready to turn down a referral if they do not believe they can devote adequate time to caring for the patient. Others have also mentioned the need for Private hospitals to develop protocols for managing the emergency patient, including adequate staffing levels for nurses and junior staff together with referral protocols to NHS facilities. I agree. Finally, all large private hospitals should consider both anaesthetic and emergency surgery and medical rotas.
Whatever happens however, we shouldn’t get this out of proportion. Emergency patients may be at risk in the private sector, but there is nothing in this case that suggests that SURGEONS are any more at risk than before. It simply reminds us to do what we have been taught to do since we were medical students: be open, explain, talk to your colleagues, make notes, don’t lie, apologise if things go wrong etc etc.
Good article in this month’s MPS magazine about David Sellu. Sarah Redston seems to have made one of the best observations. Prison is a scary prospect for middle class professionals and his sentence brings to mind Admiral Byng failing to do his utmost in 1757 and being shot. Voltaire commented that the purpose was to “encourager les autres” It all contributes to a less enjoyable and more defensive medical life which is expensive medicine. Would I be guilty of manslaughter for not admitting dying patients to ITU if I thought it inappropriatebut an expert witness disagreed?
Excellent article entitled “Surgical Removal”in the Sunday Times today by Margarette Driscoll about the David Sellu case. She asks whether doctors will now shy away from risky operations? Here is the first paragraph:
The first night in prison, as the locks fall, is a shock to anyone. Try to imagine the sense of dislocation felt by a hospital consultant, a man with a flourishing private practice and successful career in the NHS, a man whose quiet self-confidence has been burnished by decades of admiration from patients and staff. When David Sellu, a colorectal surgeon, left the Old Bailey last November, convicted of manslaughter after a patient died in his care, he was wearing one of the tailored suits he favoured for his clinics. The next time his wife saw him, in Belmarsh — the first of three prisons in which he has been held — he was in a standard-issue burgundy tracksuit. They sat either side of a coffee table, with a chair on one side for the prisoner and seats for visitors on the other, all fixed to the ground. “The prisoner mustn’t stand up. You’re not allowed to touch,” says Catherine Sellu. “It was terrible… not in a million years did he think something like this could happen.”
The rest of this balanced and well written article is available on the Sunday Times website. I recommend that you read it!
https://www.thesundaytimes.co.uk/sto/Magazine/article1445464.ece
Reading this site it seems that there is much interesting disagreement about this case. As to concluding that Mr Sellu lied. I doubt that very much indeed. I wonder how many of us when at the mercy of a system determined not to be found wanting, and the whole process Mr Sellu went through when he was singled out against a likely backdrop of a series of systems errors would find that our words could be deemed lies if we had made any small unintentional errors. I wonder. The lesson here is do not seek to judge this and look very carefully at the circumstances……….
Roger well done for highlighting this case to Jeremy Hunt. To those who want to listen here is the link. There was an “energy” behind the conviction of David Sellu FRCS and although he made errors so did others. Yet he paid the full price. Up until then he had an unblemished career. Many rightly wonder what really happened in that courtroom and whether justice was truly served.
https://audioboo.fm/boos/2469219-should-doctors-who-make-mistakes-that-lead-to-patient-deaths-go-to-prison-hear-jeremy-hunt-s-response#t=0m2s
There are rumours, which I do hope are true, that an appeal is being considered on behalf of David Sellu. I agree entirely with the view expressed above by Matt Dunkley: David made errors, but so did others. The sad end result was the result of an error chain in which David Sellu was only a single link. I would hope that an appeal would lead to his release from a prison term that is really serving no useful purpose for society and costing us all money. Below is a photograph of David and his family reproduced from the Sunday Times article: “Surgical Removal”
Roger recommended this blog at a meeting last week.
I have followed this issue for a few months and tried to be objective; these are 2 of many good links on the subject.
https://davidsellu.org.uk/
https://www.medicalprotection.org/uk/casebook-may-2014/medicine-and-manslaughter
But however neutral we may be, we cannot escape that this case has profound consequences for all doctors, surgeons in particular, medical law practice and therefore the general public and patients of the future. At a time of austerity, but also scrutiny by regulatory bodies, we are experiencing a reduction in the traditional team working which has underpinned surgical practice for decades and have a greater dependence on individuals who are often working on multiple sites for a number of reasons. The support of the hospitals is paramount and their systems need to evolve/improve to ensure adequate out of hours radiology cover, theatre access and anaesthetic availability. Team working is essential but in a different format to previously. Hand overs are now more formalised. Care is consultant delivered on the whole. We can all learn a great deal from this tragic case and others and all the significant medicolegal cases need to be discussed regularly at undergrad and postgraduate training so that clinicians are kept current in their practice, not just medically but medico-legally. We need to be made aware of the risks so that lessons are learnt and this does not become a recurring theme but also that an adherence to defensive, and expensive , medicine does not become the default position. Coress (http://www.coress.org) has made significant inroads into the confidential reporting of events to follow the excellent example of the aviation industry and we must be honest in this but this case makes one wonder how honest clinicians will really be if the risk is a custodial sentence. The duty of candour as I understand it relates more to organisations than individuals but it is clear this subject has become extremely important.
I am surprised that I still meet other surgeons who are not aware of this case. The swiss-cheese theory of holes lining up was extremely unfortunate for the patient. David Sellu may have been responsible for some, but I doubt all of the errors and Hospitals need to take a close look at the matrix of clinical mechanisms to ensure the doctors and more importantly the patients are adequately protected. We need to raise our game and ensure we document to show the efforts that are made day in and day out to ensure high standards.
We rely a huge amount on those around us – individually and corporately – especially our Consultant colleagues. We need to explore how this needs to best evolve to suit the significant changes around us.
I’m in my final year of a law degree and my dissertation includes a consideration of the elements of gross negligence manslaughter. I have read an article in the sunday press from last August which suggests that the David Sellu’s patient had a 40% mortality risk in any event.
If that was so, then on the basis of the earlier case law at least, i cannot see how causation was proved by the crown. Can anyone shed further light on this aspect? Since there was no appeal, a formal law report of the trial is unavailable, so the submissions of the expert witnesses are not readily available.
As a lay person and ex-patient I feel that prison was not at all appropriate. However, did anyone wonder or investigate how a bowel injury could have occurred in a knee operation?
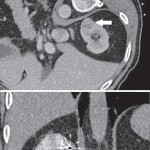
Thank you for your interest in this case and your comment on the blog. The bowel problem was a completely separate pathology and not an injury, but most likely a perforated diverticulum of the sigmoid colon resulting peritonitis (I haven’t seen the detailed medical details of the case). The development of a second illness when a patient is in hospital recovering from a knee operation can cause diagnostic difficulties, and the symptoms could well have been masked by the pain-killers given for the orthpaedic procedure. Perforated diverticular disease has a very significant mortality with or without laparotomy, but it is true that the delay in getting the CT done and the operation performed certainly did not improve the patient’s chances of survival.
I worded my post a bit oddly, I was not a patient of Mr Sellu, just had several operations. The reason I am raising it is because I had hip replacements. The surgeon unintentionally lengthened my first leg and I had some abdominal pain so he did the same for the second hip..I had severe abdominal pain and in a subsequent laparoscopy the tissue holding the large bowel to the abdominal wall was found to be torn. Both the knee and hip operations I believe that the leg is bent at the groin, I think my injury occurred when the leg was straightened out. Over 3 years on I still have problems. While the patient is under anaesthetic they are not adjusting automatically.
For all of those interested in this important issue there is an upcoming “Doctor’s and Manslaughter” meeting in London. Do take a look at this link:
https://www.doctorsandmanslaughter.org.uk/
and register for a modest £25. A very worthwhile investment if it keeps you out of prison!
Check out the first ten mins of this BBC programme. It sets the scene for the disaster…..
https://www.bbc.co.uk/programmes/b053hg48
Hi Roger, what are the accepted mortality statistics for perforated diverticular disease please?
Good question Gerard. The mortality from perforated diverticular disease is high whatever and whenever treatment is initiated. Especially in a patient who is already recovering from major joint surgery and who would have been receiving strong analgesics which would have masked the symptoms. I will have to ask some of my colleagues who are colorectal specialists to give a view on this point as well.
Another issue that is troubling is that David Sellu, having already suffered the indignity imprisonment for the management of this case, will now have to go through the trials and tribulations of a GMC investigation. There has been a great deal of disquiet about the way in which the GMC pursues it’s investigations recently. Not least because 28 doctors, including two trainees, have committed suicide while under GMC investigation. I have a blog running on the http://www.trendsinmenshealth.com website: entitled “Is GMC investigation an ‘occupational hazard’ that doctors should accept?”
https://trendsinmenshealth.com/gmc-investigation-occupational-hazard-doctors-accept/
Comments on that issue are welcome.
I have spoken to Professor Sina Dorudi about the mortality from perforated diverticular disease (the presumed diagnosis in this case). He pointed out that this would depend on whether there was a septic peritonitis or a faecal peritonitis: the latter being more hazardous.
For those interested in this case and the issues surrounding it, there is another blog running on the http://www.trendsinmenshealth.com website: https://trendsinmenshealth.com/clinical-negligence/#comments
Thanks Roger.
I guess we have to presume that that the pathology responsible for this patient’s spontaneous colonic perforation was diverticular disease. Certainly, perforated (sigmoid) diverticular disease can be the first presentation of this condition and the patient may not necessarily have experienced any previous problems with recurrent diverticulitis. The data on mortality for this condition very much depends upon the degree and source of contmaination within the peritoneal cavity following perforation. Free uncontained perforation with widespread (or even local) faecal contamination can carry a mortality of 50% or more even in patients with no pre-existing morbidity. But this quite uncommon and more frequently, the pathology is a localised perforation with purrulent contamination of the left lower quadrant or lower abdomen. The mortality for this condition is considerably lower with prompt diagnosis and treatment. Either way prompt diagnosis is key, followed by a period of vigorous resuscitation with intravenous fluids and antibiotics (ideally in a HDU setting with good monitoring) and then the patient needs to proceed directly to surgery. Herein lies another key crucial caveat in the managment of these patients – they need to progress to surgery fairly promptly as there is a physiological window of opportunity during which resuscitation measures are beneficial. Thereafter, the patient can decompensate quite rapidly as septic shock and terminal organ failure develops and then all treatments (including surgery) tend to be ineffective.
I have not familiarised myself with the precise details of this case. But for whatever reason it appears that the CT scan took a while to be performed and then, of course, it was some time before the patient got to surgery. During which time the patient almost certainly developed the irreversible organ failure associated with septic shock.
I am a solicitor who acts for patients in pursuing negligence claims against doctors and hospitals and as such it may be thought that I can be expected to have limited sympathy for Dr Sellu`s plight. But that is far from being so. I have very considerable sympathy. In fact this case troubles me every bit as much as it clearly troubles everybody else who has contributed to this blog. I do not see what possible public interest can be served by criminalising and imprisoning doctors simply for making mistakes that lead to an unintended outcome – however tragic that outcome may have been. To be guilty of manslaughter in this context a person must make a mistake, which is “grossly” negligent and which also causes death. But the distinction between “gross” as opposed to “ordinary” negligence is in reality meaningless and whether or not the error results in death is a matter of chance.
I am sure that, aside from a Shipman scenario (where there was no “mistake” because the harm was intended) no doctor causes harm to a patient just for the fun of it. It happens because everybody (including judges!!) makes mistakes everyday and always will. Most of our mistakes of course have no consequences or are easily rectified. Few mistakes result in the tragedy of a death (although it does happen). Precisely the same mistake can easily result in very different outcomes (e.g, no harm at all or death) and yet the culpability is the same. So what is the public policy justification in making one a serious offence justifying imprisonment and the other no offence at all. The only difference between the cases is the outcome, which is a matter of chance. Making one a criminal offence certainly does nothing to reduce the likelihood of other doctors making other errors in the future.
Regrettably however I fear that the political climate is against this view because I have a sense that these prosecutions are happening more often. For example, I understand that an anaesthetist at Tunbridge Wells NHS Trust is currently facing a manslaughter charge after the death of a patient and that the Trust itself is also facing a corporate manslaughter charge; although I know nothing about the case. Neither do I know what can be done to stop this trend.
My only other thought is that reading the Judge`s sentencing remarks, he seems to have decided that a custodial sentence was appropriate because David Sellu gave a false (or at least a different) account of what happened to the internal investigation. If so this is yet another example of a bad situation being made very much worse because of an attempted cover up. Speaking as a lawyer my strong advice is that if confronted with a seriously threatening situation such as this, seek immediate help from your medical defence organisation, give them a complete and honest account of what happened and then follow the advice that is given.
A doctor and two nurses have recently been charged over the death of a woman who had left an abortion clinic hours earlier.
Dr Adedayo Adedeji, 62, is accused of manslaughter by gross negligence and by failing to take reasonable care of people affected by his work.
Nurses Gemma Pullen, 31, and Margaret Miller, 54, are charged with the same offence.
The expectant mother, 32, reportedly died in a taxi in January 2012 following an abortion at a clinic in Ealing, west London.
All three have been summoned to appear at Ealing Magistrates’ Court on June 19, 2015.
It was reported in 2013 that the woman had travelled to the capital from Dublin, having been refused the operation in Ireland.
According to the Irish Times, a post-mortem showed the mother-of-one had died from a heart attack caused by extensive internal blood loss.
Speaking anonymously, the woman’s husband allegedly told the paper his wife had had a child in Ireland in 2010, but added the pregnancy had been painful and complicated by fibroids – a condition that could have caused infertility if treated.
Last year it was reported the number of Irish women travelling to the UK for abortions had dropped below 3,000 for the first time.
And yet another recent manslaughter charge against medical professionals:
Doctor and nurse appear in court charged with manslaughter of six-year-old Jack Adcock.
“A doctor and a nurse appeared in court recently charged with the manslaughter of a six-year-old boy at Leicester Royal Infirmary.
Dr Hadiza Bawa-Garb and ward sister Theresa Taylor pleaded not guilty at Nottingham Crown Court to the manslaughter by gross negligence of Jack Adcock at the hospital on February 18 2011.
Dr Bawa-Garb (38) of Watkin Road, off Upperton Road, Leicester, and Theresa Taylor (55), of Henley Road, Western Park, Leicester, were granted unconditional bail.
Staff nurse Isabel Amaro (47), of Balmoral Court, Manchester, did not appear in court due to ill health”.
There does seem to be little doubt that manslaughter charges against members of the medical profession are becoming more prevalent. How should this change the way we practice?
Read more: https://www.leicestermercury.co.uk/Doctor-nurse-appear-court-charged-manslaughter/story-26425441-detail/story.html#ixzz3cMDcJ9sN
This story seems destined to run and run. The Times on Saturday ran an article on David Sellu which emphasised that sending surgeons to prison for their clinical errors seems only likely to make the profession more “risk averse” and more likely to practice defensive medicine: https://www.thetimes.co.uk/tto/health/news/article4494980.ece.
It costs more to incarcerate a person for a year than it would to send your son to Eton! It does seems hard to see what good has come from the imprisonment of Mr Sellu who was just on the verge of retirement from surgery before the sentence was given.
Letter to the President of the Royal College of Surgeons from Peter Taylor
15 July 2015
Miss Clare Marx CBE, DL, MBBS, PRCS
President
The Royal College of Surgeons of England
35-43 Lincoln’s Inn Fields
London WC2A 3PE
Dear Miss Marx,
You will no doubt be aware of the increasing incidents of doctors being investigated by the Crown Prosecution Service (CPS) with a view to bringing charges for Gross Negligence Manslaughter following an unexpected death of a patient. Regrettably the CPS cannot confirm this increase as they claim not to record the occupation of individuals suspected of criminality. However we are concerned about a possible increase in criminal investigations over the last 18 months, with at least four cases reported in the media during 2015 alone. Over the same time there has been a notable increase in the number of times police have been called in to investigate hospital deaths.
All responsible doctors want malpractice to be rooted out of the profession. However we are adamant that individual doctors, who are readily blamed in circumstances where mistakes and delays have culminated in a patient’s death, should be given a fair trial. This means ensuring that the evidence given to judge and jury should properly, and accurately, reflect the facts as known to the doctor under the particular circumstances in which they were making decisions affecting that patient’s care. The quality of evidence given by expert witnesses is variable and may be heavily biased. We are concerned that retrospective analysis of evidence may produce unfair trial outcomes and will do nothing to uphold patient safety.
The reality is that unexpected deaths in healthcare more commonly result from a chain of events rather than one individual doctor’s gross negligence. We are concerned that jailing doctors allows systemic failures, which commonly provide the context in these cases, to recur which may then result in further unexpected deaths.
We are also concerned about a climate of fear enveloping healthcare in this country where unrealistic expectations are placed on doctors. As the population gets older, has more chronic co-morbidities and takes increasing amounts of medication, doctors will be reluctant to take on high risk patients for fear of being prosecuted in the event of a death.
We are similarly writing to each president as it is our firm view that the Royal Colleges should:
1. embark on a process of reviewing, registering and overseeing the quality and training of expert surgical witnesses to both coroners’ and criminal courts. This would be in the best interests of patient safety and the future of the profession;
2. form a working party to review the quality control of expert witnesses. The working party, together with the Lord Chief Justice and the Office of the Chief Coroner, should be safeguarding fairness in future gross negligence manslaughter trials involving doctors;
3. establish a process of nominating expert witnesses from suitably qualified individuals to prevent expert witness “shopping” by either prosecution or defence;
4. suggest to the Attorney General that the CPS should begin to compile data on the professional occupation and ethnicity of those it chooses to investigate. Ethnic monitoring is now essential to ensure fair treatment irrespective of background. There is evidence to suggest that there are excess successful prosecutions of and disproportionate charging of doctors from black and ethnic minorities (Quick et al 2015). This will do nothing to encourage diversity within the profession.
All doctors need to have full confidence in the Royal Colleges. As a collective body we would like to see them show how high a value they place on probity within the criminal justice system insofar as it affects the profession.
Yours sincerely,
Peter R Taylor Ex President of the Vascular Society of Great Britain and Ireland.
Read the article in the Daily Mail about the David Sellu case: https://www.dailymail.co.uk/news/article-3174741/A-scalpel-hospital-buried-evidence-clear-surgeon-jailed-patient-s-death-40-year-exemplary-career.html. Some interesting revelations! And many supportive comments.
CRIMINALISING DOCTORS LEAVES PATIENTS’ LIVES AT RISK SAY SENIOR MEDICAL PROFESSIONALS
In the wake of David Sellu’s conviction, senior medical colleagues continue to speak out over their concerns that five and a half years on from this incident, patient safety continues to be compromised as hospitals’ systemic failings are yet to be addressed. 800 people have died unexpectedly in private hospitals in England during the last four years[1].
Professor Roger Kirby, Medical Director at The Prostate Centre says:
“Criminalising doctors sets a dangerous precedent. I personally have been called in to deal with emergencies in private hospitals in the middle of the night. The situation can be very challenging. If surgeons become paranoid about taking on these cases under the prospect of personal prosecution should the patient die, lives will be put at risk as fewer patients will receive the operations they urgently need.”
Research suggests the average Briton may go through 7 surgeries during his/her lifetime[2]. Complications are said to arise in 8-13% of cases, half of which are believed to be preventable through systemic improvements.
Mr Sellu is currently appealing his conviction at a hearing this Autumn. Meantime, between them, many medics supporting him have the following concerns and observations:
– As a direct result of the prosecution of David Sellu (following the death of his patient from complications after a routine operation), surgeons are increasingly adopting defensive medical approaches to complex surgery in the private sector. There is a risk that some may even refuse to operate on higher-risk patients. This unnecessarily limits the outcomes for patients with challenging medical histories.
– A culture of openness is of paramount importance for patient safety. Medical practitioners need to be transparent about their mistakes but in a no blame environment. If they fear the hospital prefers to make individuals culpable, and likely subjects of criminal investigation when errors occur, this will not happen. All hospitals, whether NHS or private, should adhere to a standard mechanism for unexpected deaths. This must include a transparent and thorough overhaul of their own systems and processes that led to the unexpected death or serious incident occurring.
– Over the past 18 months, doctors claim anecdotally that there has been a notable increase in the number of times police have been called to investigate hospital deaths and an increase in CPS charges against medics. However the numbers cannot be verified as the CPS claims not to hold data on the professional occupation, or ethnicity, of individuals charged. Doctors are also concerned at what appears to be a disproportionate number of successful prosecutions against black and ethnic minority doctors. They acknowledge that the overall prosecution numbers are small, but nonetheless are concerned about the emergence of a growing trend.
– Patients opting for elective surgery in a private hospital are not routinely made aware of the consequences of private hospitals’ failure to institute emergency oncall rotas. Should complications arise, delays can be caused to emergency surgery with sometimes fatal consequences if no anaesthetists can be found to allow the operation to proceed.
– There is no standardised consent required from those NHS patients whose elective surgery is passed to the private sector.
– There is no formally recorded data of the 6000 private patients referred annually to the NHS following surgical complications arising in the private sector. The Department of Health should collate and publish the nature and cost of these referrals.
– The significant cost of these emergency referrals is currently being born by the over-stretched NHS, rather than being the responsibility of the private healthcare companies.
– Private hospitals should be required to report safety incidents along exactly the same lines as NHS hospitals are currently required to do, as part of a requirement for CQC registration. Currently, patients who die in an NHS hospital following referral from a private hospital, are listed under NHS mortality and morbidity statistics, and not under those of the referring private hospital. This means no reliable audit can be made of patient safety in private hospitals.
A number of supportive senior doctors have today lent their name to a letter (copy available) written to Claire Marx, the President of the Royal College of Surgeons calling for the College to ensure that the quality of evidence given by expert witnesses at trial is consistent and properly reflects the knowledge of the medical professional making the decisions at the time. They are particularly concerned that retrospective analysis of complex medical evidence, in the sterile environment of a court room, may produce unfair trial outcomes and will do nothing to uphold patient safety.
Mr Ian Franklin, Consultant Vascular Surgeon and representative of the Friends of David Sellu Campaign, says:
“Unexpected deaths in healthcare more commonly result from a chain of events rather than one individual doctor’s gross negligence. Bringing charges against individual doctors, which the CPS is increasingly doing, does not make patients safer as there is no incentive for the organisation in which the mistakes occurred to address their systemic failings. One crucial safety factor is for private hospitals to have an anaesthetic rota to deal with emergencies. Some private hospitals have done this but in many, emergency rotas are still non-existent.”
Responsible doctors are calling for a review of the way private hospitals investigate and report unexpected deaths and serious untoward incidents (SUIs). It is woefully inconsistent across the sector. Another immediate step should be the requirement to introduce emergency anaesthetic rotas in those hospitals that still fail to provide them, to improve patient outcomes following surgery in private practice. These demands are rightly put on the NHS so there is no reason not to have similar expectations of the private sector, particularly given the growing numbers of patient referrals from the NHS.
[1] https://chpi.org.uk/wp-content/uploads/2014/08/CHPI-PatientSafety-Aug2014.pdf (Exec Summary)
[2] https://chpi.org.uk/wp-content/uploads/2014/08/CHPI-PatientSafety-Aug2014.pdf (para 47)
Slowly but surely evidence is accruing that David Sellu was scapegoated for a series of errors that lead to the patient’s death. Read this article: https://www.dailymail.co.uk/news/article-3174741/A-scalpel-hospital-buried-evidence-clear-surgeon-jailed-patient-s-death-40-year-exemplary-career.html
His appeal is due to be heard in September
Read this article in the Guardian about David Sellu’s forthcoming appeal against his manslaughter prosecution
https://www.theguardian.com/society/2015/aug/06/doctors-sign-letter-expressing-worry-over-criminalisation-of-surgeon
And another manslaughter charge against a healthcare professional:
https://www.dailymail.co.uk/news/article-3228075/Eye-doctor-Britain-charged-negligent-manslaughter-death-eight-year-old-boy.html
And another case for those following this sorry saga:
https://www.dailymail.co.uk/news/article-3276076/Doctor-denies-manslaughter-primary-school-teacher-Mrs-Coffee-died-giving-birth-emergency-Caesarean-section.html
David Sellu’s appeal against his setentence is scheduled for this week on the the 9th December. We will keep you informed of the outcome. I am keeping my fingers crossed!
A surgeon whose jailing for manslaughter over a patient’s death at a private hospital caused widespread alarm among doctors has won permission to appeal against his conviction.
Three judges at the Court of Appeal in London granted colorectal surgeon David Sellu, 68, leave to appeal after a short hearing.
Sellu, a senior consultant surgeon with a successful 40-year career in the NHS, was sentenced to 2 ½ years in prison in November 2014 for contributing to the death of James Hughes in February 2010 at the Clementine Churchill Hospital in Harrow, north London[i]. He was called in after Hughes, 66, a retired builder, developed abdominal pains in the wake of a routine knee operation.
Sellu operated on Hughes just over 24 hours after he first saw him, but he died from a perforated bowel. An internal investigation by the hospital found “systemic failures” but the report was not disclosed at Sellu’s trial and he was blamed for a catalogue of delays.[ii]
More than 300 doctors, including professors of surgery, signed a letter to the president of the Royal College of Surgeons noting that “unexpected deaths in healthcare more commonly result from a chain of events rather than one individual doctor’s gross negligence”.
Sellu’s lawyers were given permission to appeal on the ground of fresh evidence showing, first of all, that Hughes’ risk of death at the time Sellu first saw him was much higher than the 2.6% put forward by the prosecution. Secondly, his lawyers argued that the significance of the fact that Hughes had been given dabigatran, a new generation oral anticoagulant, was not fully appreciated at the time.
Read this piece in the Mail on Sunday: https://www.dailymail.co.uk/news/article-3357866/Scalpel-surgeon-wins-right-appeal-jail-sentence-retired-builder-died-following-routine-knee-surgery.html
And a related article in Trends about a vascular surgeon who was charged with manslaughter after an intra-operative death of a patient: https://trendsinmenshealth.com/wp-content/uploads/sites/13/2015/11/Surviving-prosecution.pdf
General Practitioner Dr Rajendra Nayak-Kokkarne knows first-hand the profound distress an accusation of manslaughter arising from clinical practice can cause, and how the MDU support can help.
Read this article from the MDU Journal:
A deadly mistake https://shar.es/1h2zFa via sharethis
Another fatal error:
https://www.bbc.co.uk/news/health-35403822
We shall see if it is NHS 111 or the clinicians who get the blame for this.
PROSECUTING DOCTORS FOLLOWING UNEXPECTED PATIENT DEATHS DOES NOT IMPROVE PATIENT SAFETY
• Results from survey on “doctors.net” of almost 1500 doctors from across medical practice
• 85% of medics believe bringing criminal prosecutions into post-death investigations encourages a culture of secrecy and cover-up
• 90% of doctors admit to practicing more defensive medicine techniques, in light of increased culture of fear, subjecting patients to additional, often intrinsically risky and intrusive tests, sending costs per patient soaring
• Fewer than half considered they were delivering safer care as a result of increasingly defensive medical practice
A survey of 1443 doctors, conducted by ‘Doctors and Manslaughter’ a campaign group working to raise awareness of the effects of the recent trend towards the criminalisation of healthcare, has uncovered alarming findings in light of the increased involvement of criminal process following unexpected hospital deaths and complications.
Police investigations into healthcare has escalated in recent years following the conviction of respected surgeon David Sellu (now the subject of an appeal). In the past year alone, 9* healthcare professionals have either been charged, prosecuted or convicted for Gross Negligence Manslaughter. These recent prosecutions, with the prospect of jail sentences for doctors when patients die, has alarmed many in the profession who say there is no evidence that a ‘blame’ culture actually makes patients safer. There is also a growing body of opinion that the charge of gross negligence manslaughter is being used inappropriately to prosecute doctors in some specialties who, in their daily lives, work in an inherently high risk environment.
Of the 1443 UK doctors responding to the survey, nearly 90% of doctors admitted to being more defensive (ordering more tests for patients than they might need, as a result of the fear of litigation), but less than half admitted that they felt they were delivering safer care as a result. 85% agreed, or strongly agreed, that being open about mistakes was less likely with increasing involvement of the law.
Most health-care professionals accept deaths and complications are best discussed in a transparent, no-blame environment. This allows lessons to be learned and future care to be improved in much the same way that pilots analyse aviation incidents. The threat of criminal sanctions leads to the practice of defensive medicine in which healthcare professionals order more investigations than necessary and the patient may be exposed to harmful procedures they do not actually need. Surgeons are circumspect about operating on high risk patients in case they end up accused of manslaughter if the outcome results in death of a patient – this results in those patients with other underlying health problems potentially losing out on operations from which they have a chance of recovery.
Defensive medicine provides no benefit, other than perhaps to the doctor, and in contrast may cause actual patient harm as well as significantly increasing costs at a time when NHS budgets are under massive pressure. The survey also shows a growing concern that the brightest doctors will not choose to enter high risk specialties such as anaesthetics, obstetrics or emergency surgery as they risk future jail sentences if they do. This could mean that a future generation of patients are made even less safe.
Frances Cappuccini Caesarean death trial halted
Frances Cappuccini died at Tunbridge Wells Hospital in October 2012
A doctor and hospital trust have been cleared of the manslaughter of a woman who died hours after a Caesarean birth, following a landmark trial’s collapse.
Mr Justice Coulson halted the trial of Dr Errol Cornish and Maidstone and Tunbridge Wells NHS Trust, saying it would be “unsafe and unfair” to go on.
Frances Cappuccini, 30, died after suffering a haemorrhage at Tunbridge Wells Hospital on 9 October 2012.
It was the first prosecution of an NHS trust for corporate manslaughter.
Dr Cornish, 67, of Holmbury Park, Bromley, south-east London, a consultant anaesthetist, had denied manslaughter by gross negligence.
The judge told the court there was little or no evidence he had done anything wrong that had contributed to Mrs Cappuccini’s death and, likewise, there was no evidence of systemic failure at the trust.
“I am firmly of the view that it would be unsafe and unfair to everyone, including Mrs Cappuccini’s family, to leave this case to the jury,” he added.
“Her unexpected death can only properly be described as a tragedy.”
He told the court Dr Cornish had taken actions that were “as far removed from a case of gross negligence manslaughter as it’s possible to be” and he and the trust that employed him had “no case to answer”.
The Crown Prosecution Service (CPS) said it had “carefully considered” Mr Justice Coulson’s judgement and decided not to appeal against his decision.
It is still deciding whether to continue proceedings against anaesthetist Dr Nadeem Azeez, who was not on trial because he had left the country.
Following the conclusion of the trial, it emerged Mr Justice Coulson had ordered the Health Secretary Jeremy Hunt to delete a tweet he posted on the second day of proceedings which said it was a “tragic case from which huge lessons must be learned”.
In a statement following the collapse of the trial, Maidstone and Tunbridge Wells NHS Trust said “no outcome from these proceedings could bring any consolation to the family” adding its sympathies were with them.
“The allegation of corporate manslaughter has been consistently denied by the trust and now also comprehensively rejected by the court,” it continued.
“The trust regrets that the Crown Prosecution Service saw fit to pursue the charge in the first place, given the additional stress this will have caused all involved.”
Dr Cornish said he was relieved with the judge’s verdict and thanked “family, friends, legal team and all those who supported me through this difficult time”.
“I would like to pay tribute to the family of Mrs Cappuccini for the restraint and dignity they have displayed throughout this trial,” he added.
Jurors had been told Mrs Cappuccini lost more than two litres of blood when she gave birth to her second son Giacomo by Caesarean.
She was taken back into theatre for surgery for postpartum bleeding but did not regain consciousness.
Mrs Cappuccini’s final hours:
Mrs Cappuccini is admitted to Tunbridge Wells Hospital in the final stages of labour on 8 October 2012
Her son, Giacomo, is born by caesarean section at 08:28 GMT the following morning
At 11:35 GMT she is taken back into the operating theatre after suffering a haemorrhage
Dr Azeez removes her breathing tube at 12:30 GMT
Half an hour later Dr Cornish is called to assist when Mrs Cappuccini encounters difficulties breathing
She suffers a cardiac arrest at 15:16 GMT and is pronounced dead just over an hour later
The prosecution claimed the Dr Azeez, who was the anaesthetist, and consultant anaesthetist Dr Cornish failed to ensure Mrs Cappuccini safely came round from surgery.
It was the first time an NHS trust had been accused of corporate manslaughter since the charge was introduced in 2008.
The prosecution also claimed if one or both doctors were found to be grossly negligent then the trust could be said to have employed someone it knew or should have known was not suitably qualified or trained for their role.
In a statement following the collapse of the trial, Maidstone and Tunbridge Wells NHS Trust said “no outcome from these proceedings could bring any consolation to the family” adding its sympathies were with them.
“The allegation of corporate manslaughter has been consistently denied by the trust and now also comprehensively rejected by the court,” it continued.
“The trust regrets that the Crown Prosecution Service saw fit to pursue the charge in the first place, given the additional stress this will have caused all involved.”
The rise and rise of defensive medicine:
https://www.theguardian.com/society/2016/jan/29/doctors-avoiding-risky-operations-due-to-prosecution-threat-survey-finds
Great article on Medical Manlaughter in The Bulletin by Dr Jenny Vaughan. Here is the link:
PDF: https://publishing.rcseng.ac.uk/doi/pdf/10.1308/rcsbull.2016.60
Full text link: https://publishing.rcseng.ac.uk/doi/full/10.1308/rcsbull.2016.60
Two GPs have appeared before a judge at Cardiff Crown Court accused of the manslaughter of a child patient.
The doctors, Lindsey Thomas, 42, of Copper Beach Drive, Tredegar , and Joanne Rudling, 45, of Blackberry Way, Pontprennau , Cardiff , each entered a not guilty plea to an allegation that they unlawfully killed 12-year-old Ryan Morse “on or about” December 8, 2012, by gross negligence.
No further details of the child’s death were put before the court during Monday’s short hearing.
The plea hearing was held before Recorder of Cardiff Judge Eleri Rees who granted both women bail until their trial takes place on May 3.
The prosecution was represented by John Price QC and both Thomas and Rudling also had leading counsel acting for them.
Ryan lived with his family at Brynither, Abertillery, and the doctors are understood to have been working in the Gwent town.
The child’s mother is expected to be called as a witness during the trial, which is expected to last about three weeks.
WalesOnline
FEBRUARY 9, 2016
https://www.walesonline.co.uk/news/wales-news/two-gps-deny-killing-12-10856608
Here is the link to a new website created by Dr Jenny Vaughan and Ian Franklin and others which focuses on the issue of gross negligence manslaughter (GNM): https://www.manslaughterandhealthcare.org.uk/
Do take a look.
Another manslaughter charge against a healthcare professional: https://www.birminghammail.co.uk/news/midlands-news/iris-teale-nurse-cleared-manslaughter-8548357
Two GPs in Wales are now on trial for gross negligence manslaughter for failing to recognise that a child was seriously ill with Addison’s disease. Follow this link to read the details:
https://www.itv.com/news/wales/2016-05-10/doctors-manslaughter-trial-boy-would-have-survived-with-emergency-treatment/
The trial of the Marie Stopes doctor (Adedeji) and midwives involved in a termination of pregnancy has just collapsed with prosecution offering no evidence.
It is hard to understand how it got so far to produce so little, and at how much expense?
https://www.lifesitenews.com/news/charges-dropped-against-marie-stopes-abortionist-accused-of-killing-woman-w
A GP was today cleared of killing a 12-year-old boy by gross negligence after he died from Addison’s disease.
Dr Lindsay Thomas, 42, had been on trial for two weeks for causing the death of schoolboy Ryan Morse after he died from the rare condition.
Her colleague, Dr Joanne Rudling, 45, is charged with manslaughter and trying to pervert the course of public justice, after she also received a call from Ryan’s mother, and then allegedly manipulated his medical records days after he died.
But Mrs Justice Judge Nicola Davies today dismissed the charge against Dr Thomas by directing the jury to find her not guilty of manslaughter.
The judge said: ’In law, on the charge of gross negligence manslaughter, there is no case to answer.
‘I direct that a verdict of not guilty be entered by you, the jury.’
Dr Thomas was charged after schoolboy Ryan died in his home in December 2012, from Addison’s Disease – a condition which includes progressive anaemia, low blood pressure, weakness and discolouration of the skin.
His mother had called Dr Thomas at Brynithir Surgery in Aberystwyth, West Wales, 24 hours before her son died for advice about his condition.
The prosecution said the GP should have realised the schoolboy was dying, and should have called for an ambulance or gone to visit the boy herself.
But Judge Davies told the court Dr Thomas’ actions didn’t amount to manslaughter.
Outside the court Dr Thomas, from Tredegar, Gwent, read a short statement saying she was ‘very pleased’ at the outcome.
She said: ’I would like to thank family, friends, patients and my legal team for their support.
‘Once again I offer my condolences to Ryan’s family.’
Dr Rudling, of Pontprennau, Cardiff, denies manslaughter and trying to pervert the course of public justice.
The trial continues at Cardiff Crown Court.
At last a step in the right direction!
The UK’s chief inspector of air accidents is the leading contender to run a new organisation which aims to make the NHS in England safer.
Keith Conradi’s appointment as head of the new Healthcare Safety Investigation Branch is due to be confirmed at a parliamentary hearing next week.
Leading doctors have said for many years that healthcare has a lot to learn from systems which promote safety in the airline industry.
Mr Conradi was a professional pilot.
He took up his current role in as chief inspector of air accidents in 2010.
Scandals at Mid Staffs and Southern Health Trusts have highlighted failings in how the NHS in England responds to patients’ complaints and deaths.
The new healthcare investigation body (HSIB) will begin work soon, with an initial budget of £3.5m.
It will carry out about 30 reviews a year.
Another manslaughter case against a clinician – this time a psychiatrist whose patient hacked a victim to death. The judge said that the doctor was blind to the risk.
https://www.theguardian.com/world/2012/dec/19/france-europe-news
If you feel strongly about these issues go to http://www.manslaughterandhealthcare.org.uk
and join the movement to stop the current tendency to criminalise medical mishaps. We are planning an all day meeting at the Royal Society of Medicine on the issue on April 24th 2017. Come along and join us there.
Dr David Nicholl (@djnicholl)
Add your signature to this petition please:
Open letter to the Academy of Medical Royal Colleges & Dept of Justice on the use of Gross Negligence Manslaughter
Optometrist who failed to diagnose disease sentenced
An optometrist who failed to spot symptoms of a life-threatening brain condition during a routine eye test of an eight-year-old boy who later died has been sentenced to a two-year suspended prison term. Honey Rose, 35, failed to notice that Vincent Barker had swollen optic discs when she examined him at a branch of Boots in Ipswich.
The abnormality is a symptom of hydrocephalus – fluid on the brain – and Vincent died in July 2012, about five months after the eye test. Rose had not looked at retinal photos taken by a colleague and failed to examine the backs of his eyes with an opthalmoscope, Ipswich Crown Court heard. Judge Jeremy Stuart-Smith, sentencing, said although it was a “single lapse”, the breach of duty was so serious that it was criminal.
Joanna Pallister Durham
Why would anyone join the medical profession?
I read with dismay the short article (In the Independent) on the optometrist jailed for failing to spot a life-threatening disease.
Whilst this is an appalling tragedy and my thoughts are with the boy and his family, our ability as a nation to see humans for what they are, human and fallible, and therefore too desperately seek blame, horrifies me. Why would anyone want to put themselves in a position where your employers are threatening constant cuts, privatisation (as in this case) and personal liability? We are creating, or actually running headlong to, a less caring, more selfish society.
For clinicians who feel strongly about this the petition is still live (and the comments are there (and no longer anonymous)
https://www.gopetition.com/petitions/open-letter-to-the-academy-of-medical-royal-colleges-department-of-justice-on-the-use-of-gross-negligence-manslaughter.html
Why become a Doctor?
Please allow me to recommend this series: https://www.bbc.co.uk/programmes/b07q3k8g/episodes/player
There’s a very topical episode 3, dealing with Gross Negligence Manslaughter (GNM), and featuring an insightful contribution from Ian Barker of the MDU. Well worth listening to.
Channel 4 tries to get to grips with GNM (medical) on a park bench a stones throw from Raymond Bldgs
https://bcove.me/3feuxpx8
Judges hear senior surgeon’s appeal against manslaughter conviction https://www.bmj.com/content/355/bmj.i5812
Judgement has been reserved after the appeal of David Sellu against his conviction for gross negligence manslaughter. We await the decision of the judges with some trepidation! A new piece of evidence was put forward by Mark Ellison QC: it transpires that James Hughes, the patient who died, had been prescribed the platelet-inhibiting anticoagulant dabigatran, which at the time had no antidote. If Hughes had been operated on during the period that Sellu was accused of being grossly negligent for not operating, the presence of dabigatran created a very high risk of catastrophic surgical haemorrhage, carrying a significant risk of death.
The new evidence is crucial because, for a manslaughter conviction, the prosecution must prove not only that the doctor was grossly negligent but that this negligence caused or significantly contributed to the patient’s death.
The very latest news on the David Sellu saga: the conviction has been quashed this morning!
Congratulations to David and to Jenny Vaughan, Peter McDonald, Ian Franklin, David Nichol and all the other clinicians who have striven tirelessly on behalf of David to achieve this result. The whole medical profession will heave a sigh of relief! As will David himself and of course his wife Catherine and the rest of his family.
https://www.bbc.co.uk/news/uk-england-37986372
More good news.
The prosecution have (very sensibly!) decided not to apply for a retrial!
The ordeal is finally over for David and his family.
A really good outcome for an innocent man!
Shame he had to go through it all
The appeal judges said the trial judge did not give the jury adequate legal guidance on what gross negligence meant.
Speaking after the conviction was quashed, Mr Sellu said there was a range of factors which contributed to Mr Hughes’s death, including problems with the whole system at the hospital.
“I think for the sake of that poor man and his family justice has not really been done,” he said.
“It has been retribution, but I don’t really believe that they’ve been served as well as they should have been.”
Mr Hughes became ill after a routine knee replacement carried out by another surgeon.
Mr Sellu later carried out surgery to repair a perforated bowel, but there had been delays in that carrying operation. Mr Hughes died two days later.
The Crown Prosecution Service has decided not to seek a retrial after David Sellu’s conviction was quashed
The original case against Mr Sellu, of Hillingdon, was based on the standard of his care over about 25 hours.
Mr Sellu argued he knew Mr Hughes needed an urgent operation, but an anaesthetist was not available for several hours and it was not safe to move the patient to the nearby hospital.
“It really was another routine day. A busy day of course, but I’d been used to working in this sort of way for many, many years,” Mr Sellu said.
Mr Sellu’s medical licence was suspended when he was convicted and would only be reinstated after a General Medical Council (GMC) hearing.
The Crown Prosecution Service has decided not to seek a retrial.
In a statement, Mr Hughes’ family said the doctor had “served his sentence”.
“Our father’s suffering was not prioritised as the emergency it so clearly was,” they said.
A spokesman for Clementine Churchill Hospital said the “original prosecution was a criminal case led by the Crown Prosecution Service and the police”.
“I had tried to prepare myself mentally, but I had no bag. I wasn’t suitably dressed: I was in a suit. And now I was locked in a tiny cubicle, being hurled from side to side as the van lurched around corners. I felt sick, both physically and psychologically.
‘If you treated animals the way we treat prisoners on their way to jail, animal rights groups would be incensed. And this was only the beginning”.
https://www.dailymail.co.uk/news/article-3953076/They-called-Dr-Death-want-restore-good-surgeon-jailed-alongside-murderers-hospital-buried-evidence-support-case-reveals-agony-finally-cleared-killing-patient.html
Professor Sir Norman Williams says prosecutors are becoming ‘energetic’ in prosecuting and convicting surgeons:
https://www.dailymail.co.uk/news/article-3959052/Doctors-scared-save-lives-case-hauled-court-NHS-adviser-s-warning-surgeon-cleared.html#comments
Senior surgeon’s conviction for manslaughter is quashed
BMJ 2016; 355 doi: https://dx.doi.org/10.1136/bmj.i6178
Another interesting piece relating to David Sellu’s quashed conviction: https://thejusticegap.com/2016/11/poor-bad-truly-atrocious-directing-jury-gross-negligence-manslaughter/
Two other blogs that may be of interest to those following this story:
https://trendsinmenshealth.com/gross-negligence-manslaughter-defensive-medicine/https://trendsinmenshealth.com/clinical-negligence/
We are also planning a meeting at the Royal Society of Medicine 1 Wimpole St W1 on Friday 21st April entitled ” Patient Safety, Litigation and Gross Negligence Manslaughter”.
Do come along and join us at should be an interesting meeting. David Sellu himself, among others including Professor Sir Terence Stephenson , Chairman of the GMC, will be speaking.
In addition this website set up by the outstanding Dr Jenny Vaughan has a great deal of up-to-date information about these issues: https://www.manslaughterandhealthcare.org.uk
An all-day meeting at the Royal Society of Medicine on “Patient Safety, Litigation and Gross Negligence Manslaughter”, with speakers including David Sellu, Sir Robert Francis QC and Professor Sir Terence Stevenson, Chairman of the GMC has now been organised on Friday the 21st April. You can register online here:
https://www.rsm.ac.uk/events/events-listing/2016-2017/sections/urology-section/urh08-patient-safety,-litigation-against-doctors-and-gross-negligence-manslaughter.aspx
Do come along and join in on the lively discussion.
Check out this editorial in Trends: ‘Justice at last’
https://trendsinmenshealth.com/article/editorial-justice-at-last/
The latest news is that David Sellu has now been reinstated by the GMC, and will be undertaking clinical practice again at St George’s and elsewhere, which is certainly to be celebrated. It is a curious coincidence that I heard this news on the 11th February, which happens to be the anniversary of Nelson Mandela’s release from prison in 1990!
Judges considering prosecutions against doctors for gross negligence manslaughter would not view a lack of NHS resources as a defence against clinical negligence, James Badenoch, a barrister who specialises in medical law and clinical negligence said at a recent meeting at the Royal Society of Medicine.
At a conference on litigation against doctors at the Royal Society of Medicine, James Badenoch QC said that he was often asked whether judges would take into account “the impossible conditions in which some doctors work.”
“The answer, to be relatively frank with you, is no,” he said. “
Here is the link to the report on the RSM meeting on Patient Safety, Litigation and Gross Negligence Manslaughter held on the 21st April with embedded video clips:
https://trendsinmenshealth.com/reports/rsm-patient-safety-litigation-gross-negligence-manslaughter/
Here are the videos from our meeting at the Royal Society of Medicine on the 21st of April. It includes David Sellu’s “Mistake or Manslaughter” and some other great talks: https://videos.rsm.ac.uk/specialties/urology-section. Do take a look.
Recently there has been a significant increase in the number of prosecutions of clinicians and other healthcare workers for gross negligence manslaughter (GNM).
Unfortunately such prosecutions are likely to impede safe healthcare by discouraging honest reporting of medical errors, and although there are few prosecutions, they are very erosive of morale.
There is therefore considerable concern about the current Sentencing Council guidelines, which are out for consultation on the appropriate sentences for manslaughter. The guidelines set out criteria for culpability among which are that:
■The offender was in a dominant role if acting with others.
■The offender was clearly aware of the risk of death arising from the offender’s negligent conduct.
Unfortunately these criteria will almost always apply to doctors caring for their patients if complications develop that are deemed to be the result of negligence. There is therefore serious concern that doctors convicted of GNM will now face more severe sentences.
We have written to the Secretary-of-State expressing our concern.
As followers of this blog will know, there has been a recent rise in the range of healthcare workers charged with “manslaughter by gross negligence.” Although prosecutions are still rare there is widespread concern that staff cannot learn from errors or near misses in a culture of blame or under threat of criminal charges. However, the GMC duty of candour tells healthcare workers to be open and honest, when things go wrong. This anonymised survey will take you no more than two minutes of your time to fill out and is being done to get a sense of your views.
If you wish you can also follow the final link (qu11) through to a very important consultation being done by the sentencing council (closing date 10/10/17). Without amendment of their proposals, healthcare workers could be facing new jail time of 12 years in the most ‘severe’ cases. There have been two recent successful appeals which have shown that both convictions for Surgeon David Sellu and Optometrist Honey Rose were unsafe. The results of this survey are anonymous but will be presented to the Crown Prosecution Service so they are aware of the impact of criminal prosecution on patient care.
Survey link https://www.surveymonkey.co.uk/r/MK85BHR
A workshop was held on the 4th October between the Royal Society of Medicine (RSM), the Crown Prosecution Service (CPS) and the British Medical Association (BMA) in Chandos House. The difficult issue of gross negligence manslaughter (GNM) prosecutions of doctors was discussed. A summary of the conclusions will be published, in the meantime here is the link to a short statement from the BMA: https://www.bma.org.uk/collective-voice/committees/medico-legal-committee/medical-manslaughter .