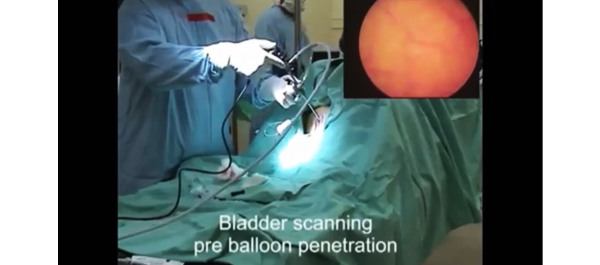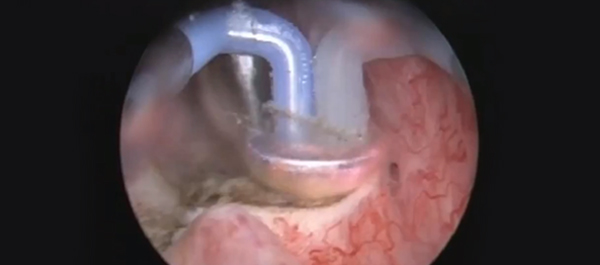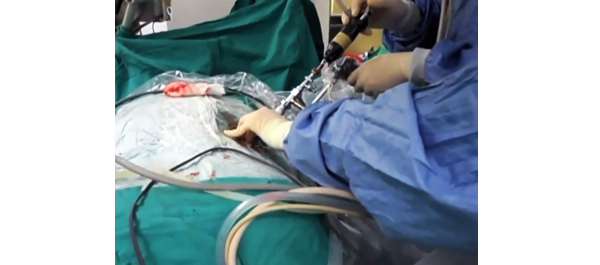
Video: Tract creation using plasma vaporization
Randomized and prospective trial comparing tract creation using plasma vaporization with balloon dilatation in percutaneous nephrolithotomy
Po Hui Chiang and Hsin Hao Su
Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan
OBJECTIVE
• To evaluate the efficacy and safety of plasma vaporization for tract creation in percutaneous nephrolithotomy (PCNL).
PATIENTS AND METHODS
• In this randomized prospective trial we enrolled 65 patients and assigned each to one of two groups: 33 patients were randomly scheduled to undergo plasma vaporization and 32 were scheduled to undergo balloon dilatation for tract creation.
• A bipolar resectoscope mounted with a plasma vaporization button electrode or a traditional balloon dilator were used to create the nephrostomy tract.
RESULTS
• The mean blood loss, mean length of hospital stay and mean operating time, stone-free rates and postoperative complications in the two groups were compared using the t-test or chi-squared test (Fisher’s exact test).
• The plasma vaporization group had a significantly lower mean (SD) decrease in haematocrit level (3.5 [2.8]% vs 6.6 [3.3]%; P = 0.02) and a shorter mean (SD) hospital stay (2.6 [1.2] days vs 5.3 [3.4] days; P = 0.0).
• There were no significant differences in the operating time, stone-free rate or cases of postoperative fever between the two groups.
CONCLUSION
• The plasma vaporization technique is safe, leads to less blood loss than the other techniques, and is a simple solution for creating the nephrostomy tract for PCNL.