The Indian captain MS Dhoni has retired from Test cricket after the MCG test in Australia. The timing of this announcement from a national hero has left opinions divided amongst pundits and people in a cricket mad nation. See the video on NDTV here.
One of India’s most successful captains, wicket-keeper and unorthodox batsmen, MS will now focus on one day and T20 cricket. With 3.3M followers on Twitter (@msdhoni) his popularity remains unabated, with Sky sports dedicating a program to highlight his test career.
If you are planning to visit his hometown for USICON 2015, Ranchi, you may be lucky enough to catch a glimpse of the great man as its brand ambassador. The BJUI will be there as the affiliated journal of the Urological Society of India. The Best of India has been published by the BJUI to celebrate this important occasion.
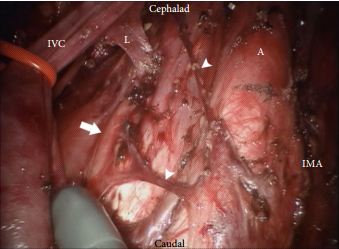
The da Vinci surgical system delivers the benefits of laparoscopic surgery with an easier and more precise human–tissue interface than conventional laparoscopic instruments. Nearly all major uro-oncological procedures are being performed robotically. In this issue of BJUI, Cheney et al. [1] present their technique and initial experience of robot-assisted retroperitoneal lymph node dissection (RA-RPLND) for patients with primary and post-chemotherapy non-seminoma germ cell tumours. Quality indicators for RA-RPLND include adequate clearance of the desired surgical field, satisfactory lymph node yield, acceptable perioperative morbidity and length of stay, as well as longer-term functional and oncological outcomes. So how well does RA-RPLND stand up to scrutiny?
The technique employed by Cheney et al., placing the robot at the head of the patient, is unfamiliar to most urologists I suspect. It appears to offer excellent access to the retroperitoneum, but still requires a re-docking when performing full bilateral dissections. Whether this technique is superior to the lateral approach that I and others have used for modified dissections requires further study [2,3]. The lymph node yield was lower than that previously reported for open RPLND and while Cheney et al. [1] observe this may be due to the use of a modified template where appropriate, the absence of any in-field recurrences at a median of 22 months is perhaps the more reliable sign that there is oncological equivalence. Concerns that a true template dissection cannot be completed with a robot-assisted laparoscopic approach are probably unjustified in my opinion. The description of surgical technique by Cheney et al., including suture ligation and division of lumbar vessels, confirms that if a surgeon is minded to do so, a complete bilateral or modified template clearance can be completed.
The absence of significant complications in this series is impressive; however, there were three out of 18 conversions to open surgery. The mean length of stay of 2.4 days is close to the 3–4 days stay I would expect after an uncomplicated open RPLND in a young fit man. However, 1–2 night stays were seen in their later cases as they gained experience. Perhaps more importantly in a group of working age men, return to full physical activity within 3 weeks is possible [2].
As highlighted by Cheney et al. [1], minimally invasive primary RPLND has been previously reported both by laparoscopic and robotic approaches. Their larger series provides an important demonstration that the robotic approach facilitates the more complex undertaking of post-chemotherapy RPLND. Furthermore they show that except for operative time, all other outcomes were similar in primary and post-chemotherapy cases.
As an enthusiast for minimally invasive therapies, I of course welcome these results and think that along with other published and presented series, they provide sufficient evidence to consider a more formal evaluation of this approach. However, how feasible is the wider introduction of RA-RPLND? Despite having experience of robotics and working in a team performing around 30 RPLNDs a year, I was only able to identify five cases during a 1-year period suitable for a robotic approach. With experience this could have been a higher proportion, but it is fair to conclude that suitable cases in typical cancer centres would be limited in number. This is particularly so for the UK and other European countries, where primary RPLND is not used. Cheney et al. [1] had similarly low numbers each year and recruited their cohort of 18 cases over 5 years.
An international multicentre registry is arguably the best way to gather more information on the safety and completeness of template dissection RPLND. Existing registries, e.g. the BAUS complex operations database, have already provided valuable insights into the results of RPLND in the UK [4] and could be combined with other international RA-RPLND databases already being compiled (Erik Castle MD personal communication). Partnership of testicular cancer surgeons without robotic experience with experienced robotic surgeons may also facilitate the development of additional centres for development of this procedure. They will also aid optimal patient selection and help avoid incomplete template dissections, which may compromise the excellent cancer control we are now used to.
There are clear potential advantages with a minimally invasive approach to RPLND, not least of which are the avoidance of a laparotomy scar, the reduction of complications and an earlier return to normal activity. Cheney et al. [1] have shown that their technique is feasible, safe and effective in the medium term and their results justify wider consideration of the procedure for further study and improvement.
In this issue of BJUI, Poulsen et al. [1] present a prospective comparison of 18F-fluoride (NaF) and 18F-choline (FCH) positron emission tomography (PET)/CT with planar whole-body bone scintigraphy (WBS) using spinal MRI, including short tau inversion recovery (STIR), T1 and T2 sequences, as the reference standard in 50 hormone-naïve patients with confirmed bone metastases on WBS. They found that both PET/CT methods were significantly more sensitive and accurate than WBS and that FCH PET/CT was more specific than NaF PET/CT.
Nevertheless, the authors should be congratulated in reporting valuable data from a prospective study where all imaging was performed in hormone-naïve patients, minimising confounding treatment-related effects, and within a small time window of 30 days; however, some questions remain. WBS is no longer state of the art for imaging the skeleton with radiolabelled bisphosphonates, such as 99mTc-methylene diphosphonate (MDP). Although NaF PET/CT has been shown to be superior to planar WBS augmented with SPECT [3], there have not been head-to-head comparisons with 99mTc-MDP SPECT/CT, where the potential advantages of the pharmacokinetics of NaF and the superior spatial resolution of PET compared with SPECT may not be as great. This may be particularly important given the difference in costs and availability of the two methods.
Despite the results from the present study, which show superiority of FCH PET/CT compared with NaF PET/CT with regard to specificity, taking the available literature as a whole, it remains unresolved as to what the best test for staging the skeleton in patients with high-risk prostate cancer should be at diagnosis. The different mechanisms of uptake of the PET tracers should be noted. NaF uptake reflects the local bone osteoblastic reaction to tumour within the bone marrow, whereas FCH uptake reflects metabolic activity within the tumour cells themselves. In prostate cancer, where the predominant effect is an increase in osteoblastic activity in the adjacent bone, the bone-specific tracers such as 99mTc-MDP and NaF have shown high sensitivity; however, direct imaging of tumour cell metabolism, such as increased choline kinase activity and cell membrane synthesis with FCH, may be advantageous in detecting metastases in the bone marrow before an osteoblastic reaction has occurred [6]. It is possible that both PET tracers may be required to provide optimum diagnostic accuracy and of course FCH PET/CT also provides valuable data on nodal and visceral metastatic disease. In patients with recurrent disease, better specificity has been reported with FCH [4], NaF possibly being limited by non-specific treatment-related effects such as osteoblastic flare. For similar reasons it may be that the more tumour-specific imaging methods, such as FCH PET/CT or diffusion-weighted MRI, may be better in assessing the treatment response of skeletal metastases. Questions therefore remain as to the best imaging test at different times in the management of patients with metastatic prostate cancer. 99mTc-MDP SPECT/CT deserves a full assessment, but perhaps the recent advent of PET/MRI and the potential synergies available from this hybrid technique may help resolve some of the remaining issues.
*Division of Imaging Sciences and Biomedical Engineering, King’s College London, † Clinical PET Centre, and ‡ Department of Radiology, Guy’s and St Thomas’ Hospitals NHS Foundation Trust, London, UK
As usual, contributions to the discussion were on a global scale including Australia, United States, Canada, United Kingdom, Ireland, France and the Netherlands. It was great to see participation from trainees and their interactions with leading experts.
Initial discussion focused on the inclusion of the patients, and questions were raised regarding the changing sensitivity of relapse detection due to improved imaging standards over the study period.
However @urorao made a good point regarding exclusion criteria:
The ‘King of Twitter’ felt the strength of study was a high 96.1% compliance rate among Danish men.
The management of stage I nonseminoma testicular cancer in terms of risk factors and appropriate treatment was nicely summarized by @drphil_urology
@dycmd chimed in on the risk factor discussion. Traditionally, with vascular invasion, the risk of relapse is thought to be 50% however it was interesting that this paper revealed that vascular invasion alone resulted in a risk of only 18%. The presence of three risk factors (embryonal carcinoma, rete testis invasion, and vascular invasion) was shown to have the historical 50% relapse rate.
The discussion then moved onto finer points of management in this group of patients,
In terms of management of Stage IA patients, participants all agreed that active surveillance is appropriate with risk of relapse being 12%.
In terms of management of stage IB patients, there were two schools of thoughts. One group saw the glass half full (@uretericbud, @nickbrookMD) and the other group saw the glass half empty (@RFowlr, @drphil_urology).
@uretericbud and @RFowlr had a somewhat contrary views on the matter.
There was a discussion regarding appropriate selection for RPLND and the conclusions of this exchange was nicely summarised by @scientistatlrge
Overall, this was a high quality discussion for our first ever journal club paper on testicular cancer. The Best Tweet Prize was supported by the European Association of Urology (@uroweb) who have kindly offered a complimentary registration to the #EAU15.
The winner was @nickbrookMD who nicely put forward his argument for surveillance
We look forward to seeing you join us for the next #urojc which commences on 4/5 January 2015 depending upon your time zone. Do follow @iurojc for updates.
Yuigi Yuminaga@Yyuminaga is an advanced urology surgical trainee at the Sydney Adventist Hospital in Sydney, Australia.
On the 16-17th February 2015 ten leading robotic centers of excellence from 4 continents will broadcast for 24 continuous hours. All the surgeons operating are experienced live surgeons, pioneers in their fields, who have contributed to the development and advancement of excellence in robotic surgery techniques.
WRSE24 incorporating 10 world leading robotic centres.
“Imagination is more important than knowledge. For knowledge is limited to all we now know and understand, while imagination embraces the entire world, and all there ever will be to know and understand.
We live in exciting and progressive times in healthcare, when technological advancements are rapidly changing the way we work and the way we learn as surgeons. Many of these technological advancements come from discoveries and innovations made outside healthcare, making the pace of change less predictable. For example, it is well known that the advancement of robotic surgery technology came from initial innovative developments made within NASA and further funded and developed by the US military [ref 1].
With the advent of minimally invasive surgery utilizing video technologies, opportunities for surgical learning greatly improved. No longer was surgical training a master-apprentice role, performed behind ‘closed doors’ with the associated limited opportunities to disseminate expertise. Video recording of surgery enabled wider dissemination of knowledge and live surgical video transmissions have revolutionized the way that national and international surgical conference meetings are now run.
Following the recently published ‘‘EAU Policy on Live Surgery Events’’, it is now assured that live surgery will be ongoing at conferences in the immediate future. However, the panel reached >80% consensus on the view that performing at a home institution may be safer. The committee also identified issues with a ‘‘travelling surgeon’’ performing complex surgery in an unfamiliar environment with a surgical team that is not experienced with the intricacies of the surgeon’s technique. LSE’s from a home institution remove or minimize these negative aspects [Declan Murphy]. Furthermore, there are other important reasons why LSE’s are enhanced when performed at a high- volume home institution. The potential to optimise surgical performance comes from working with an experienced team. Consistency is a key measure of quality, and robotic surgery in particular epitomises teamwork. An established theatre team will move purposefully through the standardised steps with well-rehearsed, orchestrated movements. It is therefore likely that the natural evolution of LSE’s, is that a greater proportion are broadcast from home institutions [Collins et al].
We aim to highlight the benefits of this approach to surgical training with a worldwide team who will represent the best of current standardized surgical technique. All the surgeons operating are experienced live surgeons, pioneers in their fields, who have contributed to the development and advancement of excellence in robotic techniques.
We will be coordinating the broadcasts using LiveArena hardware and infrastructure. LiveArena are currently, primarily a sports broadcaster and in partnership with Microsoft have developed, cutting edge video streaming technology that enables streaming of HD video onto the internet, whilst requiring minimal capacity (3Mb/sec). The videos can be watched in real-time and also paused or rewound via their link and the video can be viewed on laptops, PC’s, smart phones and tablets even on standard hospital wifi, making this approach very accessible and scalable.
Communication with surgeons in real-time:
There will be a blog set up on the WRSE24 website, that any doctor registered can ask questions or highlight a topic for discussion. Questions can also be posted via this BJUI blog or via Twitter #WRSE24. During the 24 hour transmission Karolinska will monitor these aspects, combining the discussions and providing regular feedback via a 24 hour ‘overview’ broadcast on a separate channel.
To see more details and to register now for this historic event go to www.wrse24.org
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers, or just click the ‘submit’ button below.
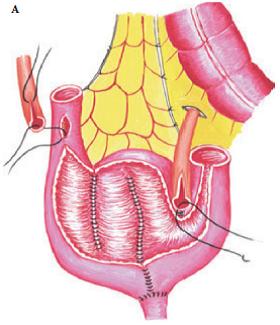
This image is taken from Harraz et al (BJUI 2014) describing long-term renal outcomes for 2 different anastomotic techniques in a W-shaped (Hautmann) neobladder formation.
Peyronie’s disease is a chronic and progressive disease characterised by fibrotic plaque of the tunica albuginea of the penis that can cause deformity, pain during erection and erectile dysfunction. Fibrosis is the hallmark of the pathology of Peyronie’s disease and is known to be driven by fibroblasts and myofibroblasts, which produce excessive amounts of extracellular matrix proteins and, hence, disturb the architecture of the tunica albuginea.
In this issue of BJUI, Kwon et al. [1] have shown that selective inhibition of histone deacetylase isoform 2 (HDAC-2) using a small hairpin silencing RNA elicits reversal of plaque development in vivo and prevention of collagen production and myofibroblast transformation in vitro. Histone deacetylases (HDACs) are a group of enzymes that remove acetyl groups from lysine amino acid in histones, causing histones to wrap around the DNA tightly and, ultimately, affecting gene transcription. In addition HDACs can de-acetylate cytosolic proteins and hence alter their function. Because of their direct effect on cell growth and death, HDACs have recently been attractive targets for anti-cancer drug development. Currently, there are > 100 clinical trials recruiting patients to investigate the clinical efficacy of HDAC inhibitors, most of which are non-selective HDAC inhibitors, bearing in mind that there are 11 isoforms of HDACs.
HDAC inhibitors have been suggested to have anti-fibrotic effects in the lung, liver, kidney and skin. They have been shown to reduce myofibroblast transformation and fibroblast activation, and counteract TGF-β actions and extracellular matrix production [2]. Although the exact mode of action of HDAC inhibitors in fibrosis is not clear, it has been suggested that HDAC inhibitors might repress the TGF-β pathway and interfere with phosphorylation and activation of STAT3, a key transcription factor in inflammatory pathways. Among all the isoforms of HDAC, HDAC-2 has been implicated in pathogenesis of fibrosis, firstly in kidney fibrosis [3] and later in Peyronie’s disease [4]. Currently available small-molecule HDAC inhibitors target more than one isoform of HDAC; to our knowledge isoform-selective small-molecule inhibitors are not available yet. Kwon et al. [1] have solved this problem using small hairpin silencing RNA to target HDAC-2 specifically. Although the clinical feasibility of such a silencing RNA approach remains to be tested, their study nevertheless gives an important indication for HDAC-2 as a possible target for fibrotic diseases, such as Peyronie’s. No doubt further research and development will be required to validate this target and develop small-molecule inhibitors selective for HDAC-2.
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers, or just click the ‘submit’ button below.
It has been another successful year for the BJUI. Our impact factor has gone up, the new design theme of ‘places’, featuring the location of the ‘Article of the Month’ on the front cover, has been well received and our web statistics have gone from strength to strength. Despite these successes, as a surgeon-scientist, I occasionally find that I am questioning myself, particularly where surgical science is concerned.
One such moment came recently while I was performing a live nerve-sparing robot-assisted radical cystectomy (RARC) during the European Association of Urology Robotic Urology Section (ERUS) 2014 meeting in Amsterdam. Open RC (ORC) is a morbid procedure and in cohort studies we thought that we had halved the complication rates with laparoscopy and lowered them even further with robotics. However, these results have not been replicated in randomised controlled trials. A letter in the NEJM comparing ORC and RARC showed no difference in outcomes, especially complication rates. Many feel that perhaps there was a difference in the experience of surgeons performing ORC and RARC, although the article itself mentions that this was not the case. Our own CORAL (randomised controlled trial of open, robotic and laparoscopic radical cystectomy) study comparing ORC, laparoscopic RC and RARC demonstrated no difference in 90-day complication rates, although all diversions were performed extracorporeally. In this issue of the BJUI, we present another randomised trial of ORC vs RARC showing no significant differences in health-related quality of life with scores returning to baseline after 3 months. We now await the results of the multicentre RAZOR (randomized open vs robotic cystectomy) study, which is expected to recruit fully this year. As I performed live, I could not help thinking about the negative results of these trials, which came up during my discussions with the audience. It is often good to question yourself rather than have blind faith without the scientific evidence.
Now for some positive news. It is becoming increasingly obvious that perhaps choline positron emission tomography (PET) will soon replace bone scans for detecting metastasis in prostate cancer. As tracer technology develops further, the death of traditional bone scanning in coming years seems imminent.
Finally, we have some exciting science for your reading pleasure. While the management of Peyronie’s disease has largely centred on various surgical techniques, there may be a new treatment for the plaque itself just over the horizon. The answer – ‘small hairpin RNA’; these can inhibit histone deacetylase 2 and induce plaque regression. Currently reported in a rat model, Phase I studies cannot be far away.