Between 2014 and 2015, 3742 radical cystectomies (RCs) were performed in the UK. The majority of these were open RCs (ORCs), and only 25% were performed with robot assistance. These data contrast starkly with the picture in radical prostatectomy (RP), for which most operations are robot assisted (79.4% of the 7673 in 2016). Given that most pelvic surgeons have access to robotic facilities (as shown by the RP trends) and urologists are typically early adopters, one must question why many surgeons have yet to be convinced by robot‐assisted RC (RARC). This question is particularly perplexing given that RC is a more morbid operation than RP and most patients with bladder cancer are considerably less fit than the average man with prostate cancer, and therefore, reductions in morbidity are especially rewarding in this cohort.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Mohit Gupta*, Hiten D. Patel*, Zeyad R. Schwen*, Phuoc T. Tran*† and Alan W. Partin*
*Department of Urology, James Buchanan Brady Urological Institute, and †Department of Radiation Oncology and Molecular Radiation Sciences and Oncology, The Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medical Institutions, Baltimore, MD, USA
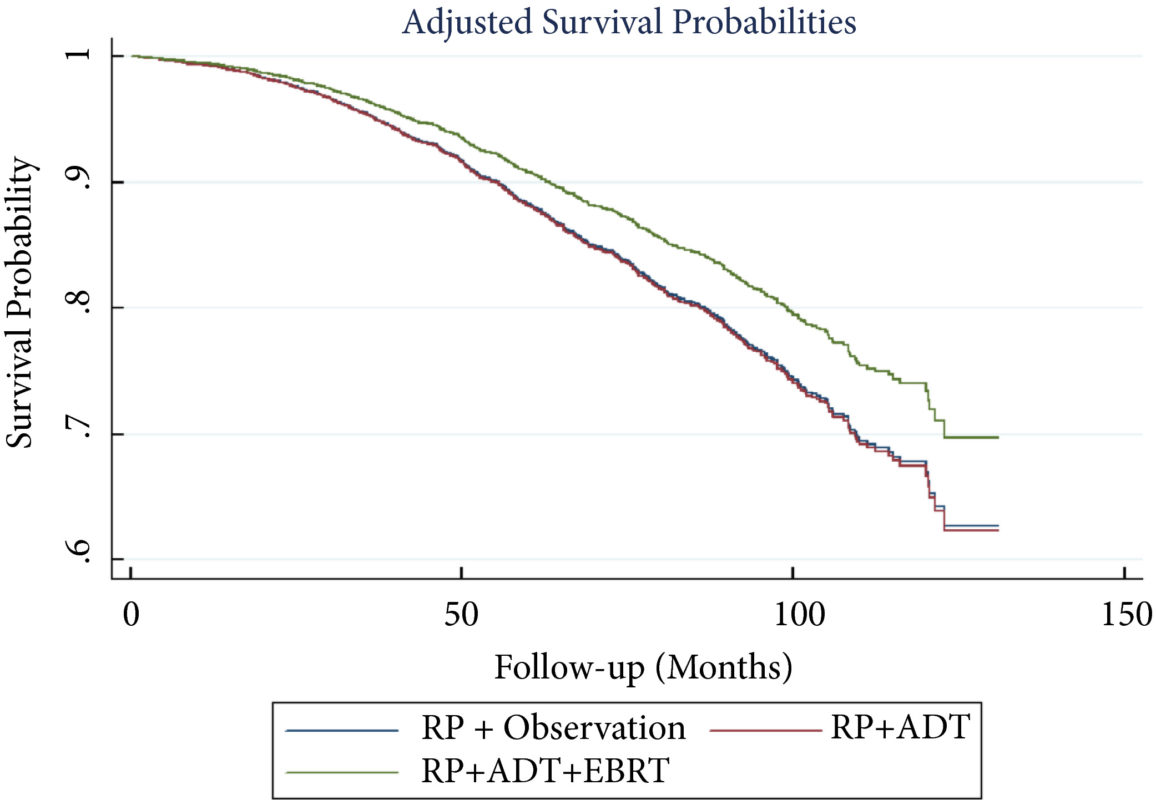
To perform a comparative analysis of three current management strategies for patients with lymph node metastases (LNM; pN1) following radical prostatectomy (RP): observation, androgen‐deprivation therapy (ADT), and external beam radiation therapy (EBRT) + ADT.
Patients and Methods
Patients with LNM after RP were identified using the National Cancer Database (2004–2013). Exclusion criteria included any use of radiation therapy or ADT before RP, clinical M1 disease, or incomplete follow‐up data. Patients were categorised according to postoperative management strategy. The primary outcome was overall survival (OS). Kaplan–Meier curves and adjusted multivariable Cox proportional hazards models were employed. Sub‐analyses further evaluated patient risk stratification and time to receipt of adjuvant therapy.
Results
A total of 8 074 patients met the inclusion criteria. Postoperatively, 4 489 (55.6%) received observation, 2 065 (25.6%) ADT, and 1 520 (18.8%) ADT + EBRT. The mean (median; interquartile range) follow‐up was 52.3 (48.0; 28.5–73.5) months. Patients receiving ADT or ADT + EBRT had higher pathological Gleason scores, T‐stage, positive surgical margin rates, and nodal burden. Adjusted multivariable Cox models showed improved OS for ADT + EBRT vs observation (hazard ratio [HR] 0.77, 95% confidence interval [CI] 0.64–0.94; P = 0.008) and vs ADT (HR 0.76, 95% CI: 0.63–0.93; P = 0.007). There was no difference in OS for ADT vs observation (HR 1.01, 95% CI: 0.87–1.18; P = 0.88). Findings were similar when restricting adjuvant cohorts for timing of adjuvant therapy. There was no difference in OS between groups for up to 2 549 (31.6%) patients lacking any of the following adverse features: ≥pT3b disease, Gleason score ≥9, three or more positive nodes, or positive surgical margin.
Conclusions
For patients with LNM after RP, the use of adjuvant ADT + EBRT improved OS in the majority of patients, especially those with adverse pathological features. Conversely, adjuvant therapy did not confer significant OS benefit in up to 30% of patients without high‐risk features, who may be managed with observation and forego the morbidity associated with immediate ADT or radiation.
The best management strategy for men with pathologically node‐positive (pN+) prostate cancer after radical prostatectomy (RP) has been debated for decades [1]. In the 1990s, the Radiation Therapy and Oncology Group (RTOG) initiated the RTOG 9608 trial to test the impact of radiotherapy (RT) and androgen‐deprivation therapy (ADT) in this setting. However, due to the rise in PSA screening and the practice of treating high‐risk prostate cancer with primary RT, the incidence of pN+ disease fell. Consequently, the trial closed due to poor accrual and the question faded in prominence. Today, both trends have reversed. PSA screening is less common and men with high‐risk prostate cancer are more frequently opting for RP. As such, physicians increasingly face the dilemma of pN+ disease. Guidelines provide little assistance, as they support everything from observation to multimodal treatment with RT and ADT. Patients and providers want to know, is there a standard treatment for all patients, and if not, how should one choose between such disparate options?
To answer these questions, one must start with the little randomised data that exist in this setting. The seminal trial by Messing et al. [1] randomised men with pN+ prostate cancer to ADT or observation with initiation of ADT after the development of symptomatic progression or distant metastases. ADT clearly improved overall survival and prostate cancer‐specific survival. However, critics noted the relatively poor outcomes in the observation group and the small sample size. Later, retrospective studies called the benefit of immediate ADT into question [2].
Against this backdrop, it is interesting that Gupta et al. [3] found the most common management approach in the USA National Cancer Database (NCDB) was observation rather than immediate ADT. Despite the randomised data, the cumulative side‐effects from lifelong ADT in a cohort of patients with no disease‐related symptoms and a median survival of well over 10 years are unappealing. Ultimately, many men do not appear to be willing to endure the diminished quality of life in exchange for a small improvement in quantity of life.
In contrast to the non‐curative nature of ADT, the possibility exists that the combination of postoperative RT and ADT could provide durable disease control, perhaps even without lifelong ADT. The data reported by Gupta et al. [3] in this edition of the BJUI provide support for this paradigm. These data add to a growing body of literature [4] that tells a consistent story with two common themes: (i) postoperative RT with ADT appears to be associated with improved survival in men with pN+ prostate cancer, and (ii) RT appears to convey the largest benefit to men with certain high‐risk pathological features. Should this body of literature lead us to eschew the old standard and advise observation for low‐risk men and RT with ADT for men at higher risk?
Before a new standard is declared, the limitations of retrospective population‐based research must be addressed. The authors performed a sophisticated analysis to reduce the impact of selection bias. However, due to the limitation of the available data, the authors were not able to account for possibly the most important variable: the postoperative PSA. One study showed that men with pN+ disease with a persistent PSA had an 8‐year clinical recurrence rate of 69% vs 12% for those with undetectable PSA [5].
It is likely that men with persistent PSA in the NCDB would have received immediate ADT with or without RT rather than observation. As such, one must be cautious of the similar survival between the observation and ADT group, especially in light of contradictory randomised data. That being said, it is reasonable for some men to conclude that the side‐effects of ADT outweigh the potential benefit, especially those with low‐risk features such as an undetectable postoperative PSA, low Gleason score, and limited lymph node involvement.
As RT with ADT appears superior to either observation or ADT alone, should more men receive RT? Probably. Of the men with high‐risk features, only 22% actually received postoperative RT. Should postoperative RT now be considered the standard for all men? Probably not. Whilst it appears that some men may indeed benefit from RT, the possibility of selection bias driving this result is real. Even if there is a true effect, identifying which patients harbour residual local disease, but do not already have subclinical distant metastatic disease is challenging. RT for all would lead to unnecessary side‐effects for men that would not benefit from the treatment. Ultimately, a randomised trial will be required to establish the benefit of RT and to define subgroups of men that may or may not benefit. Until then, we will continue to rely on excellent work like the accompanying paper from Gupta et al. [3] to identify men who may benefit from postoperative RT and ADT.
I had been using Twitter for a while but I never experienced the true power of this social media platform. It was a cold call from @VerranDeborah and @juliomayol when I started to notice the hashtag #SoMe4Surgery. I was pleasantly surprised and impressed by the active engagement of the #SoMe4Surgery participants. After participating in a #SoMe4Surgery live conversation event on #surgicalinfection, I finally realized the potential impact of a simple hashtag.
While I was amazed by how #SoMe4Surgery brought the surgical community together, many of the topics being discussed were not entirely relevant or specific to a urologist per se. I felt the need of a hashtag specific to Urology, and I quickly started to conceptualize and plan ahead in building up the #UroSoMe community. The #UroSoMe twitter account was officially registered in August 2018.
#UroSoMe stands for ‘Urology Social Media’. My initial thought about #UroSoMe was simple. I wanted to develop a hashtag specific to urology. I wanted to increase public awareness about different urological conditions. Most importantly, I wanted to bring the urology community closer together through this social media platform. I believe there is so much for us to learn from each other, and such interactions should never be bounded by physical or geographical restrictions. Coincidentally, I was invited to talk about social media at the 27th Malaysian Urological Conference 2018, and I decided to take this opportunity to introduce #UroSoMe to the urology community.
The initial response from the audience was promising. Even after the meeting, many urologists came to me for in-depth discussions about the opportunities and applications of social media in urology. I felt that #UroSoMe might really work and it was time to gather more people to establish the community. The first invitation sent in on 14 December 2018, which I often regard as the ‘start date’ of the #UroSoMe community.
By inviting and encouraging people around to use a common hashtag, the #UroSoMe community keeps growing. With increasing momentum, the first #LiveCaseDiscussions was planned. It was a pre-planned event for urologists to get ‘online’ and discuss about some posted cases. A polling had been held in advance, and the topic to be discussed was chosen to be ‘Stone’.
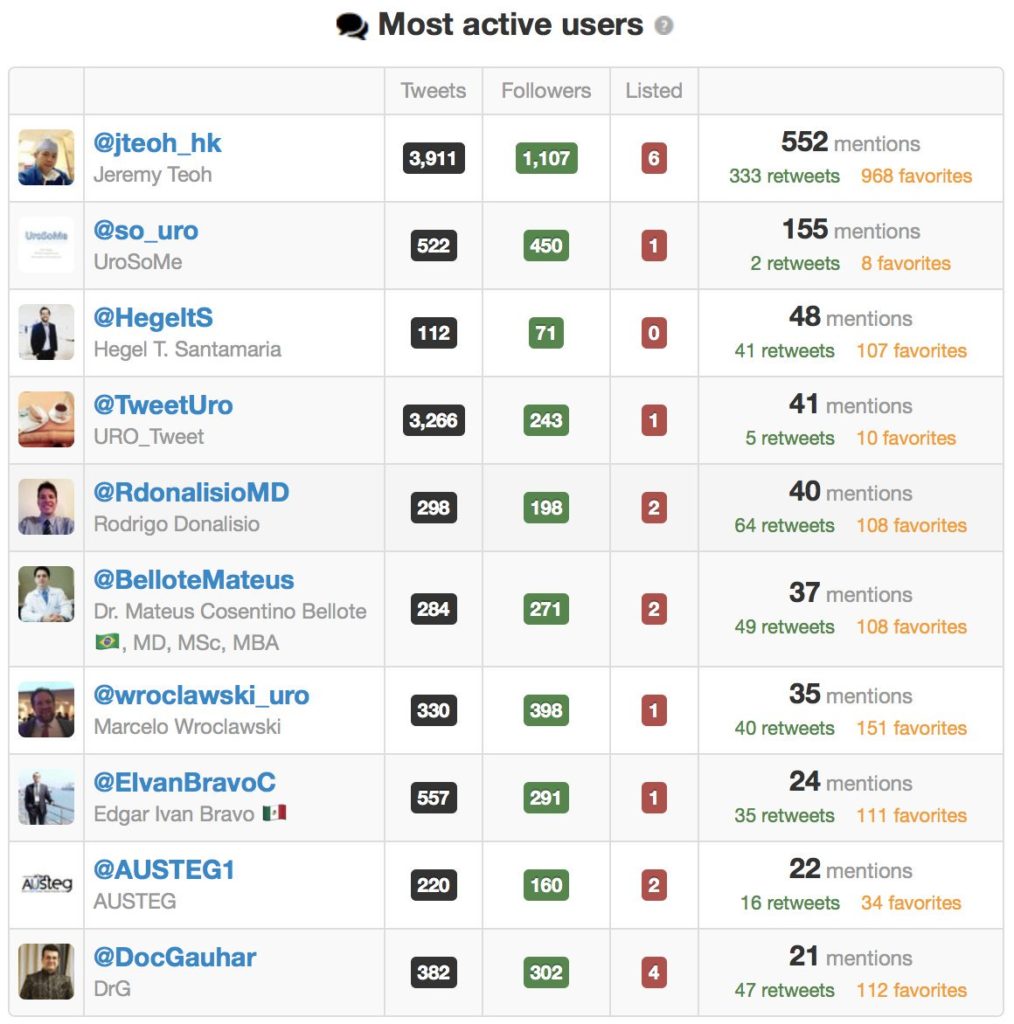
The #LiveCaseDiscussions was on air at 4pm (CET) on 5 January 2019. A total of 9 cases had been presented and discussed. Hosting this event was overwhelming with vigorous discussions among the participants. It took approximately 2 hours to ‘complete’ the event, but the conversations went on for the next few days. Special thanks must be given to the most active users. #UroSoMe and the first #LiveCaseDiscussions would never be successful without their tremendous support.
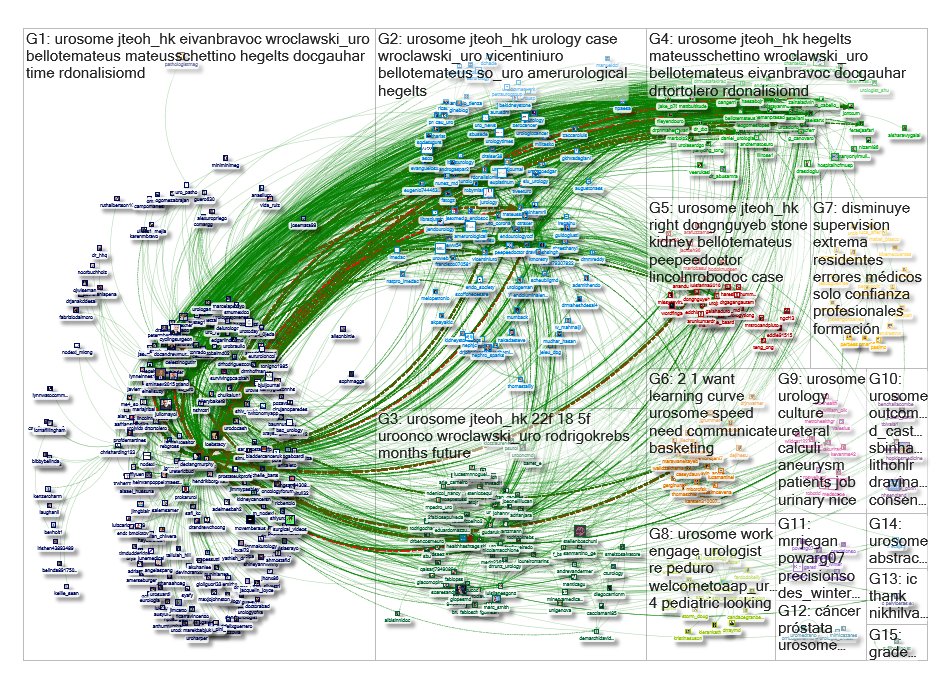
The immediate effect of the #UroSoMe #LiveCaseDiscussions event was overwhelming. This graph represents a network of 515 twitter users whose tweets contained the hashtag #UroSoMe. 6692 mentions, 1044 retweets and 617 replies were recorded within a 10-day period from 27 December 2018 to 6 January 2019. From a social science point of view, this picture represents a ‘tight crowd’, in which discussions are characterized by highly interconnected people with few isolated participants. I guess this is exactly how we feel about the urology community!
Apart from #LiveCaseDiscussions, the #UroSoMe working group is also keen to host events including #LiveForum, #LiveJournalClub and #LiveTeaching. This is only the beginning of #UroSoMe and we believe there is huge potential to be explored. It is only with your support that #UroSoMe can continue to grow. We look forward to meeting you on Twitter and,
hopefully, at #EAU19 and #AUA19 as well!
P.S. I must thank @juliomayol for the inspiration of #UroSoMe, @gmacscotland for his teaching on social media analytics, and @marc_smith for his support in NodeXL.
About the author:
Jeremy Teoh (@jteoh_hk) is a Urologist based in Hong Kong, China.
Giulia Lane M.D. is a Fellow in Neuro-urology and Pelvic Reconstruction in the Department of Urology at the University of Michigan; Kyle Johnson is a Urology Resident in the same department.
In this podcast they discuss the following BJUI Article of the Month:
To investigate the impact of implementing magnetic resonance imaging (MRI) and ultrasonography fusion technology on biopsy and prostate cancer (PCa) detection rates in men presenting with clinical suspicion for PCa in the clinical practice setting.
Patients and Methods
We performed a review of 1 808 consecutive men referred for elevated prostate‐specific antigen (PSA) level between 2011 and 2014. The study population was divided into two groups based on whether MRI was used as a risk stratification tool. Univariable and multivariable analyses of biopsy rates and overall and clinically significant PCa detection rates between groups were performed.
Results
The MRI and PSA‐only groups consisted of 1 020 and 788 patients, respectively. A total of 465 patients (45.6%) in the MRI group and 442 (56.1%) in the PSA‐only group underwent biopsy, corresponding to an 18.7% decrease in the proportion of patients receiving biopsy in the MRI group (P < 0.001). Overall PCa (56.8% vs 40.7%; P < 0.001) and clinically significant PCa detection (47.3% vs 31.0%; P < 0.001) was significantly higher in the MRI vs the PSA‐only group. In logistic regression analyses, the odds of overall PCa detection (odds ratio [OR] 1.74, 95% confidence interval [CI] 1.29–2.35; P < 0.001) and clinically significant PCa detection (OR 2.04, 95% CI 1.48–2.80; P < 0.001) were higher in the MRI than in the PSA‐only group after adjusting for clinically relevant PCa variables.
Conclusion
Among men presenting with clinical suspicion for PCa, addition of MRI increases detection of clinically significant cancers while reducing prostate biopsy rates when implemented in a clinical practice setting.
February’s cover shows Gapstow Bridge in Central Park, Manhattan: this stone version was constructed in 1896 replacing the earlier wooden version. It provides a welcome contrast to the modern skyscrapers which form part of the Manhattan skyline beautifully viewed to the South of the bridge. The bridge has been famously used in many films and TV shows, including Home Alone 2 and Dr Who.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Mihir Desai*, Mo Bidair†, Naeem Bhojani‡, Andrew Trainer§, Andrew Arther§, Eugene Kramolowsky¶, Leo Doumanian*, Dean Elterman**, Ronald P. Kaufman Jr.††, James Lingeman‡‡, Amy Krambeck‡‡, Gregg Eure§§, Gopal Badlani¶¶, Mark Plante***, Edward Uchio†††, Greg Gin†††, Larry Goldenberg‡‡‡, Ryan Paterson‡‡‡, Alan So‡‡‡, Mitch Humphreys§§§, Claus Roehrborn¶¶¶, Steven Kaplan****, Jay Motola**** and Kevin C. Zorn‡
*Institute of Urology, University of Southern California, Los Angeles, †San Diego Clinical Trials, San Diego, CA, USA, ‡University of Montreal Hospital Centre, University of Montreal, Montreal, QC, Canada, §Adult Paediatric Urology and Urogynecology, P.C., Omaha, NE, ¶Virginia Urology, Richmond, VA, USA, **University Health Network University of Toronto, Toronto, ON, Canada, ††Albany Medical College, Albany, NY, ‡‡Indiana University Health Physicians, Indianapolis, IN, §§Urology of Virginia, Virginia Beach, VA, ¶¶Wake Forest School of Medicine,Winston-Salem, NC, ***University of Vermont Medical Centre, Burlington, VT, †††VA Long Beach Healthcare System, Long Beach, CA, USA, ‡‡‡University of British Columbia, Vancouver, BC, Canada, §§§Mayo Clinic Arizona, Scottsdale, AZ, ¶¶¶Department of Urology, UT Southwestern Medical Centre, University of Texas Southwestern, Dallas, TX and ****Icahn School of Medicine at Mount Sinai, New York, NY, USA
To present early safety and feasibility data from a multicentre prospective study (WATER II) of aquablation in the treatment of symptomatic men with large‐volume benign prostatic hyperplasia (BPH).
Methods
Between September and December 2017, 101 men with moderate‐to‐severe BPH symptoms and prostate volume of 80–150 mL underwent aquablation in a prospective multicentre international clinical trial. Baseline demographics and standardized postoperative management variables were carefully recorded in a central independently monitored database. Surgeons answered analogue scale questionnaires on intra‐operative technical factors and postoperative management. Adverse events up to 1 month were adjudicated by an independent clinical events committee.
Results
The mean (range) prostate volume was 107 (80–150) mL. The mean (range) operating time was 37 (15–97) min and aquablation resection time was 8 (3–15) min. Adequate adenoma resection was achieved with a single pass in 34 patients and with additional passes in 67 patients (mean 1.8 treatment passes), all in a single operating session. Haemostasis was achieved using either a Foley balloon catheter placed in the bladder under traction (n = 98, mean duration 18 h) or direct tamponade using a balloon inflated in the prostate fossa (n = 3, mean duration 15 h). No patient required electrocautery for haemostasis at the time of the primary procedure. The mean length of stay after the procedure was 1.6 days (range same day to 6 days). The Clavien–Dindo grade ≥2 event rate observed at 1 month was 29.7%. Bleeding complications were recorded in 10 patients (9.9%) during the index procedure hospitalization prior to discharge, and included six (5.9%) peri‐operative transfusions.
Conclusions
Aquablation is feasible and safe in treating men with large prostates (80–150 mL). The 6‐month efficacy data are being accrued and will be presented in future publications (ClinicalTrials.gov number, NCT03123250).
The Asia Pacific Advanced Prostate Cancer Consensus Conference (APAC APCCC 2018) brought together 20 experts from 15 APAC countries to discuss the real‐world application of consensus statements from the second APCCC held in St Gallen in 2017 (APCCC 2017).
Findings
Differences in genetics, environment, lifestyle, diet and culture are all likely to influence the management of advanced prostate cancer in the APAC region when compared with the rest of the world. When considering the strong APCCC 2017 recommendation for the use of upfront docetaxel in metastatic castration‐naïve prostate cancer, the panel noted possible increased toxicity in Asian men receiving docetaxel, which would affect this recommendation in the APAC region. Although androgen receptor‐targeting agents appear to be well tolerated in Asian men with metastatic castration‐resistant prostate cancer, access to these drugs is very limited for financial reasons across the region. The meeting highlighted that cost and access to contemporary treatments and technologies are key factors influencing therapeutic decision‐making in the APAC region. Whilst lower cost/older treatments and technologies may be an option, issues of culture and patient or physician preference mean, these may not always be acceptable. Although generic products can reduce cost in some countries, costs may still be prohibitive for lower‐income patients or communities. The panellists noted the opportunity for a coordinated approach across the APAC region to address issues of access and cost. Developments in technologies and treatments are presenting new opportunities for the diagnosis and treatment of advanced prostate cancer. Differences in genetics and epidemiology affect the side‐effect profiles of some drugs and influence prescribing.
Conclusions
As the field continues to evolve, collaboration across the APAC region will be important to facilitate relevant research and collection and appraisal of data relevant to APAC populations. In the meantime, the APAC APCCC 2018 meeting highlighted the critical importance of a multidisciplinary team‐based approach to treatment planning and care, delivery of best‐practice care by clinicians with appropriate expertise, and the importance of patient information and support for informed patient choice.