Since 2008 we have cycled in Sicily, Malawi, Madagascar, Patagonia, South Africa and Rajasthan raising more than three quarter of a million pounds for The Urology Foundation. The seventh and latest instalment of the TUF cycling series is an amazing 450km cycle challenge through two of South East Asia’s most fascinating countries. The challenge starts in Vietnam’s Ho Chi Minh City and finishes at the world heritage site of Angkor Wat in Cambodia. En route we will shed a lot of sweat, but also experience breathtaking scenery, ancient temples and the warmth of the local people.
The cycling will be tough but we are going to be using bikes from ecosmobike.com to make it less harder, it will be in hot and humid conditions, but the camaraderie along the way will be very special as doctors, patients and supporters team up to raise much needed funds for The Urology Foundation (TUF).
Funds raised by Cycle Vietnam to Cambodia will enable The Urology Foundation to help improve the management and treatment of urological diseases through the development and support of medical education and sponsorship of research – training healthcare professionals specialising in urology and supporting basic and clinical research by funding scholarships in the UK and abroad.
Day One (Fri 10 November 2017) – Depart UK
Overnight flights from London to Ho Chi Minh City, Vietnam
Day Two (Sat 11 Nov) – Arrive Ho Chi Minh City – Transfer Ben Treh
On arrival in Ho Chi Minh City we are met at the airport by our support team where buses will be waiting for us to transfer, approximately two hours, to our hotel in the town of Ben Treh. In the afternoon we will have the bike fitting. Dinner will be at the hotel and will be followed by a briefing about the challenge ahead.
Day Three (Sun 12 Nov) – Ben Tre – Tra Vinh 50kms (approx. 31 miles)
Today we will have a warm-up day with the cycling being relatively easy and the distance not too challenging. After breakfast we cycle out of the hotel along lovely country roads with very little traffic. We then follow a traffic free route through villages that give us an insight into Vietnamese rural life. After crossing a number of river tributaries by bridge we reach one that requires a short ferry crossing. About an hour later we reach the main Mekong River where we re-group for a longer ferry crossing.
Day Four (Mon 13 Nov) – Tra Vinh – Can Tho 104kms (approx. 64 miles)
The cycling today is fairly flat and takes us through rural communities and a number of small towns. Interest today is provided by the many Pagodas that we pass, some of which we will use for rest stops.
Day Five (Tues 14 Nov) – Can Tho – Chau Doc 70kms (approx. 43 miles)
We leave our hotel early this morning with a road transfer of approximately 2.5 hours. We start cycling from the town of Am Cham. We stop at a local restaurant in the small town of Triton for lunch before continuing through scenic agricultural land. This afternoon we encounter our first major climb. Further, smaller climbs take us into the town of Chau Doc where we find our overnight hotel. On arrival we will de-fit the bikes in preparation for our crossing into Cambodia.
Day Six (Wed 15 Nov) – Chau Doc – Phnom Penh
Today we enjoy a day off the bikes and a fascinating journey by boat from Vietnam to Cambodia. After breakfast we have a short transfer to the harbour where we embark on the boats that will take us along the historic Mekong River to the border.
We will see many boats along the way and experience life on the river which supports many thousands of Vietnamese. After crossing the border we continue our journey up-river to the city of Phnom Penh where we have lunch in a restaurant overlooking the busy harbour.
We will visit the Royal Palace which is described as an impressive Khmer style Palace. We overnight at a hotel in Phnom Penh where we will be briefed by our Cambodian support team.
Day Seven (Thurs 16 Nov) – Phnom Penh – Kampong Cham 60kms (approx. 37miles)
Today we have our first day of cycling in Cambodia. Following an early breakfast we will have a short transfer to take us out of the city to the surrounding countryside where quiet roads await us. After about 35kms we reach the end of the tarmac road and continue the rest of today on dirt roads. We overnight in the town of Kampong Cham.
Day Eight (Fri 17 Nov) – Kampong Cham – Kompong Thom 107kms (approx. 66 miles)
This is probably our most demanding day of cycling. After breakfast we leave town on an undulating road that passes many Temples and Pagodas and leads us into a forest of rubber trees. We will have lunch today in a large Pagoda complex before continuing our ride into the town of Kampong Thom.
Day Nine (Sat 18 Nov) – Kompong Thom – Siem Reap 60kms (approx. 37 miles)
This morning after an early breakfast we have a transfer of approximately 1 hour to our start point at Kampong Kdei. Our route today takes us through the Cambodian countryside until we reach the outskirts of Siem Reap. Our finish line will be at the entrance to the ancient city of Angkor where we will enjoy a celebratory drink and have a photo opportunity. This evening we will have our celebration dinner at a nearby hotel; this will be followed by a cultural show.
Day Ten (Sun 19 Nov) – Siem Reap – Visit Angkor Wat / Free Day
Today is a free day to explore the areas ancient ruins and temples, or relax by the pool, or do a spot of shopping. Why not re-visit the Angkor Wat temple, take a walking tour of the overgrown ruins of Ta Prohm which is entwined with tree roots and gigantic creepers, visit the tranquil Bayon with its multitude of serene stone faces, or see the impressive 350m long Terrace of the stone Elephants.
Day Eleven (Mon 20 Nov) – Depart Siem Reap
We depart for the airport at Siem Reap to begin our journey home.
Day Twelve (Tues 21 Nov) – Arrive UK
Altogether we will have cycled 450 Km in extremely hot and humid conditions. Do support us with a donation to a great cause by sponsoring Louise de Winter our CEO’s fundraising page here: https://cyclevietcam2017.everydayhero.com/uk/louise-de-winter All donations made will go towards funding the vital research, training and education in urology diseases so badly needed.
John Wickham BSc, MB BS, MD, FRCS(Eng), FRCP(Hon), FRCR(Hon), FRSM(Hon)
1927 – 2017
The news of the passing of the legendary John Wickham on 26 Oct 2017 will sadden many. Here is a celebration of the life of a visionary thinker, innovator and pioneering surgeon.
Born in Chichester, John moved with his mother to Littlehampton and spent many happy years in rural Sussex. This year he published his book “An Open and Shut case – The story of Keyhole or Minimally Invasive Surgery” which describes his unique journey through life and his passion for reducing the trauma of surgery for the benefit of his patients. A couple of years before this, he sent me the “raw” version to read and comment on. This will forever remain a treasured possession along with a first signed copy of the final version which arrived on my desk in May 2017. A brilliant exercise in honest writing combined with his wry humour.
There were a number of exciting events in his childhood. He describes “epilation radiotherapy” to his scalp to eradicate ringworm which he provides as the explanation for the lack of hair in later life. Such personal touches keep the reader engaged as do his daily travels from Littlehampton to Bart’s (St. Bartholomew’s Hospital), costing £16 per quarter. He was interviewed by Sir William Girling-Ball for his entry into medical school and subsequently worked for Sir Ronald Bodley-Scott, physician to HM the Queen. Time spent in the Royal Air Force (RAF) toughened him up for the complexities of life as a surgeon.
He was trained in urology by Mr A W Badenoch, another legend in his own right. John describes his first inguinal hernia repair, during which his chief had to leave to take a phone call and he was saved by guidance from the anaesthetist. In his days the pass rate for the FRCS was around 10% and he was one of the lucky ones! He subsequently worked with Prof. Ian Aird of the textbook fame. He met his wife Ann, during a below knee amputation from behind a surgical mask. He was awarded a Fullbright scholarship to Lexington, USA which he thoroughly enjoyed. Despite the offer of a job to stay back, the family decided to return to the UK, where he became a Bart’s man, going on to lead the Department of Urology as its head with Bill Hendry as his colleague.
He was also the Director of the Academic Unit at the Institute of Urology at the then 3Ps (Peter, Paul and Phillips) Hospitals and after the move of St. Peter’s to the Middlesex Hospital. He was also Consultant Urological Surgeon to the King Edward VII Hospital and The London Clinic.
He is credited with a number of pioneering achievements. His device for renal cooling with coils was published in the BJU in 1967. He worked with the famous Sir David Innes Williams and was awarded the Hunterian Professorship. He also published a seminal paper on urethral pressure profile.
Very few will know that he was sidelined with an attack of acute pancreatitis and needed a cholecystectomy for gall stones.
He developed PCNL with Mike Kellett and then the Society and Journal for Minimally Invasive Therapy (SMIT) as well as the Intrarenal Society. He inspired the future generation of great innovators like Graham Watson, Ron Miller and Malcolm Coptcoat, to name a few. With the help of the Kuwait Health Office he managed to instal a Dornier lithotripter in Welbeck street which was revolutionary in those days.
John developed the PROBOT, the first autonomous surgical robot with Prof. Brian Davies at Imperial College. Initially tested in potatoes, it was then refined with the addition of a mapping ultrasound and a vaportome, leading to a world first clinical trial at Guy’s, where he had moved to with the support of Lord Ian McColl. In this project, he was ably helped by Malcolm Coptcoat, Anthony Timoney, Senthil Nathan and Bibhas Kundu. Many years later this device was displayed at a public exhibition at the Royal College of Surgeons of England. It is curious how autonomy is again being discussed amongst roboticists after some 30 years.
Following retirement from the NHS he continued to innovate by establishing a company called Syclix which allowed him to design laparoscopic instruments with pen like grips rather than the traditional handles. He arrived at Guy’s one summers morning to show me these instruments to try on one of my laparoscopic nephrectomy patients. At my request, he examined Ben Challacombe’s thesis on the first ever randomised trial of telerobotics and was then guest of honour at our first robotics symposium in 2004 and the inauguration of the King’s-Vattikuti Institute of Robotic Surgery in 2014.
While clinically active he did his best to spread his philosophy about Minimally Invasive Surgery throughout the world by lecturing and publishing articles in the BMJ, amongst other journals. Many did not believe in him, but he was clearly light years ahead of his time. He received numerous honours, which included the Cheselden Medal and the Galen Medal of the Society of Apothecaries.
It was a privilege to know him and he will remain a lasting inspiration to many.
Olá! The 37th Congress of the Société d’Urologie (SIU) was held in Lisbon, a beautiful, historic city (19th-22nd October 2017). It is the first time the congress has been held here. We were told by the co-hosts during the opening ceremony that Portugal has a history of finding new routes and building bridges to other cultures, which they hoped to emulate at the Congress. The iconic 24 de Abril Bridge, the largest in Europe, was visible from the Congress Centre serving as a visual reminder of bridges being made during this congress.
The SIU is unique as it is a truly international association with no country or continent affiliation; it has 7000 members from 130 countries and 24 directors from every continent. Therefore the congress brings urologists from all over the world together. The words “Together, United, Stronger” said during the opening ceremony resonated as the ethos of the conference; and is especially pertinent in the current worldwide political climate. Furthermore, that the educational, global and philanthropic aspects of being part of such a society was highlighted as ways we can all help each other.
SIU 2017 had an engaging scientific programme providing a valuable educational experience to attendees over the four days. It covered the breadth of urology and we were honoured to listen to such notable speakers. The navigable congress centre (as well as the congress being a smaller meeting, as compared to EAU, AUA) meant delegates could easily attend whatever took their interest. The Scientific Programme included Plenary sessions, Master Classes, debates, ‘controversies’ sessions, instructional courses, poster presentations, the SIU Nurses’ Symposium and hosted urological organisation meetings. There were also Industry supported sessions and an Exhibition Hall.
The social programme allowed relaxation and networking amongst colleagues; plus sampling local Portuguese wines, food and an insight into Portuguese culture. The opening ceremony included a Fado performance. The SIU night held at Pátio da Galé in the PraÇa do Comércio was the pinnacle of the social aspect of the conference. The refreshments were plentiful and delicious, there were gelato stands as well as enough Pastel de Nata to feed a small army! A typical brass band, ceramic station, football net and DJ kept people entertained until we were told to leave. The SIU President’s Dinner held in the Queluz Palace was an amazing night in impressive surroundings for invited guests.
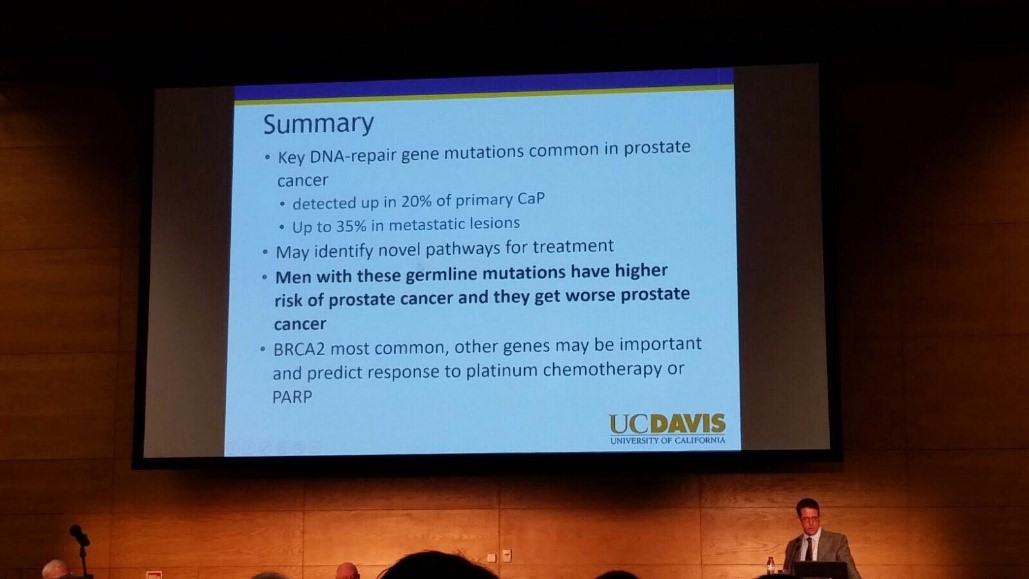
The fully attended WUOF session on the first day brought experts in the field of Urological cancers to provide their views on the changing paradigms and new treatments. All talks provided succinct, expert opinion. The presentation by Marc Dall’Era on the genetics of prostate cancer and link with the BRACA gene was particularly informative; especially as these men get worse cancer: pictured. Genetic counselling of patients diagnosed with prostate cancer may need to increase in the future. Genomics was discussed in other cancer sessions too; it’s growing availability, reducing costs and correlation with difference in outcomes between patients must surely strengthen the argument for more personalised medicine.
I also particularly enjoyed the presentation by Tony Finelli who unraveled the notion of ‘surgical outcome’ which is often used to analyse the quality of surgery; this is then used in arguments for high volume centres. He suggested instead that assessing quality needs Quality Indicators and one alone isn’t sufficient. His group in Canada used their national database to propose 32 Quality Indicators, which are valid, reliable, feasible and useable; they found that higher quality had lower mortality and morbidity. Patient centred care, patient selection, high quality surgery and recovery was a common theme in other sessions too.
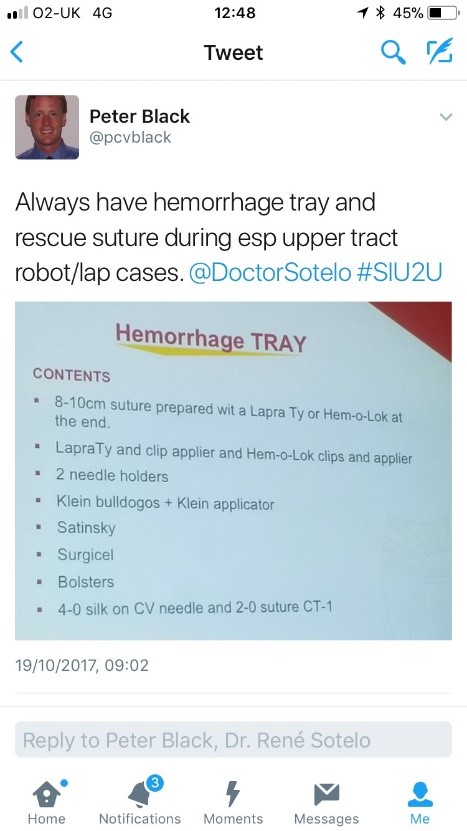
The SIU Innovators Symposium didn’t disappoint; highlights included Dr Sotelo’s presentation of ‘sticky situations’ in robotic surgery. His operative videos showed all the things you really don’t want to see whilst operating, however he and the panel provided tips in order to avoid or correct these operative mistakes. Dr Sotelo’s advice regarding having a ‘haemorrhage tray’ present was ingenious and useful: pictured. Thank you to Dr Sotelo and Dr Knudsen who shared their operative videos with us in order to provide this learning; mistakes in surgery should be shared to avoid others making the same mistakes. The symposium also invited two influential leaders, Professor Prokar Dasgupta, editor BJUI, and Professor Arnulf Stenzl to give their approach on leadership. Prof Stenzl suggested it was easier to explain how not to be a bad leader as he has learnt more from his mistakes than from successes. Prof Dasgupta suggested his leadership style was to be collaborative, trusting team members to deliver, democratic and transformative; also that he, as a leader, wanted to “help other people do well”.
SIU had a strong presence of trainees; many attending to present their academic work during the moderated poster sessions, listen to worldwide experts and of course network with others from around the world and generating future collaborations. One session ‘Sage Advice from the Wise’ was particularly aimed at trainees’ where Urological trainees met 10 experts (all wise, but certainly not old!). We were able to discuss career plans, ask questions about fellowships and talk about the advantages of academia alongside clinical practice. There was also a Residents Rapid Fire Q&A which was won by Dr Avinash Odugoudar: pictured.
Urological cancer treatment featured heavily on the programme. One particularly inspiring talk on advanced testicular cancer by one of the leading surgeons in Europe, Axel Heidenreich, really expanded our horizons of just what can be achieved operatively for patients with metastatic disease, including aortic resection and Whipple’s procedure. It proves that big, open surgery does exist in urology for the right patients; requiring expertise and courageous surgical skills but offering patients treatment despite disseminated disease. One session included debating the use of routine radiation for positive surgical margins in prostate cancer. The presentations by Dr Dall’Ezra and Dr Briganti actually came to very similar conclusions. Both wanted to avoid over treatment and championed a risk stratified approach with emphasis on patient selection; as not all those with positive margins recur. It was suggested that choosing those at greatest risk of recurrence for example the site(s) of positive margin, high Gleason score, early rise in PSA (even if remains less than 0.5) and ultra-sensitive PSA can help to stratify need for adjuvant radiotherapy; or alternatively monitor with option for salvage treatment.
Robotic assisted surgery for prostatectomy, cystectomy and nephrectomy was debated freely throughout the congress. Most quoted recent evidence that there is no clear advantage with regards to blood loss, LOS, long term outcomes and survival; but very different costs. Dr Mihir Desai argued that if you already had the robot you should encourage high volume surgery, but that departments have a responsibility to put the robot to good use; not for simple cases, but rather be reserved for difficult operations so the real advantages of robotic assisted surgery will be better appreciated. Criticism was made of RCTs not being the right research method for comparing surgical techniques as it leads to comparison of individuals not techniques. We eagerly anticipate the iROC study. An important point made regarding robotic cystectomy was that it must include intra-corporeal bladder formation, otherwise many of the advantages of the minimally invasive part are lost. Laparoscopic surgery was argued as not old fashioned; but rather an efficient and cost effective method of minimal access surgery without compromising on outcomes. However open surgery is still an option in many hospitals worldwide; a question from the audience included the dilemma faced by departments whose similar outcomes between open and laparoscopic procedures do not justify the switch to laparoscopy.
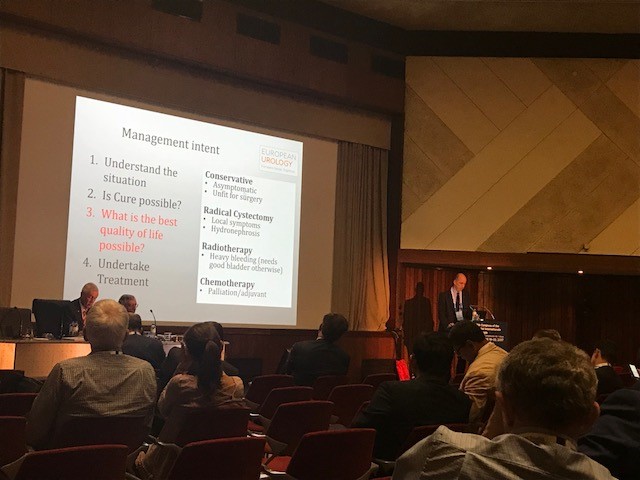
Prof Catto, editor of European Journal of urology delivered a compelling presentation of the advantages of radical cystectomy over radiotherapy for locally advanced bladder cancer. He also mentioned the importance of surgical planning and management intent: pictured. In some cases he does pre-operative MRI, however a PET scan when organised, doesn’t necessarily change his management. He also presented a plenary lecture on risk factors for upper tract TCC which confirmed smoking as the number one risk as well as occupation. However combustion occupations and amine-relate occupations show a difference in cancer aggression suggesting the biology of the cancer is different. Like others, he wanted to aim for personalised treatment of cancer with specific treatments according to genotype.
Debating the merits of surgery was a common theme in several sessions, perhaps unsurprisingly. However a particular highlight was the debate of medical vs surgical theory for lichen sclerosis (LS). The clear and compelling argument by Bradley Erickson for medical treatment rested on 10 points, which included: that LS is an inflammatory condition and these are not necessarily managed by surgery, the dermatologist and gynaecologist manage LS without surgery, LS in the urethra demonstrates squamous change which is reversible and lastly that we don’t really fully understand this disease yet.
Female urology was the first plenary session of the congress and the use of mesh unsurprisingly featured in other sessions, included one entitled ‘controversies in urology’. The clear message from Dr Badlani was to know the anatomy and not to ‘have a go’ at continence surgery, it needs expertise. He and his panel presented difficult cases including mesh seen at cystoscopy, operative video of hydro-dissection and an image of compete extrusion which led the audience to wonder if it had even been placed correctly in the first place!?
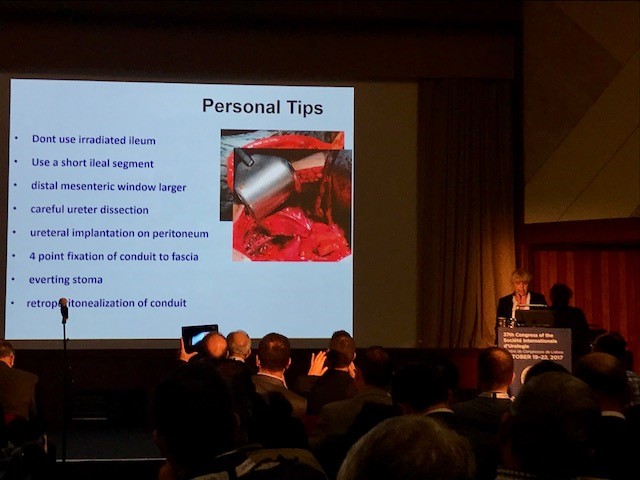
In the joint SIU-GURS meeting panel members each presented a challenging case from their experience of reconstructive surgery and ileal conduit formation; then this was discussed amongst the panel. There was an amazing X-ray of a huge stone in an ileal conduit due to stasis of urine, confirming the need to avoid long conduits. A fear held by many was early failure of the anastomosis; when debating when to re-operate, I particularly liked the phrase “three months to let the belly cool down” said with an American drawl. Margit Fisch shared her top tips of surgery: pictured. An insight into managing continence in patients with Spina Bifida was succinctly presented by Sean P. Elliot; he advised that the patients needed to be ‘proud of their stoma’ and that each needed an individual surgical plan but holistic approach.
Endourology and stone sessions were well attended and each explored different treatment modalities for stone management. Plus the congress offered masterclasses for ureteroscopic techniques, the joint SIU-Endourology session, poster sessions and a ‘controversies session’ debating URS vs Mini-perc. There was also an instructional course on lasers and flexible ureteroscopic technique. Experienced surgeons from across the globe argued for and against the role of ESWL vs RIRS vs PCNL in modern practice. Aside from patient and stone factors there was an appreciable point made of the importance of surgeon experience and available resources of the institution. Non-surgical aspects of stones were also presented, such as diet and hydration in stone disease. Advances in stone surgery, including a robotic assisted ureteroscope was particular enlightening and futuristic; however brought up the inevitable dilemma of clinical need for such technology at a time of financial restraint facing many healthcare systems.
Andrology sessions included a joint SIU-ISSM session, a master class on urethral stricture disease, video session on male reconstruction and poster session on sexual function and dysfunction. There was a debate on the role of the urologist in the management of male infertility and improving sperm. The (interesting) use of an acronym F.A.S.T was described by host urologist from Portugal Dr Pedro Vendeira: pictured. This is in relation to the follow up of non-responders to PDE-5 inhibitors, of which non responders were those who had tried these medications more than eight times. He described a 50% drop out of the use of these drugs due to cost, side effects and co-morbidities. The difficulty of treating Peyronies was discussed by Dr Moncada who confirmed the absence of the role for medical therapies, except use of PDE-5 inhibitors to strengthen erections. There was a role for ‘ penile rehabilitation’ which included a (peculiar) traction device. He presented his and the EAU indications for surgery and he stressed the importance of managing patient expectation and informed consent.
In conclusion, the SIU Congress was both informative and enjoyable. Our co-hosts promises: of warmth, friendship and the Portuguese tradition of sharing wine were delivered alongside a beneficial education programme. Those that did not attend can access abstracts and lectures online via the SIU@U platform.
SIU are also increasing their activities with the following initiatives: ‘B2B’ bench to bedside, ‘Uro-Technology’ training and ‘U-care’ a global urological research collaboration. SIU also wants to build on the opportunities for global education and global health; plus help colleagues without same level of resources.
Thank you to the SIU organisers for a successful congress! Thank you to the presenters and speakers for their expertise and dedication to academia in urology; and congratulations to all the prize winners. I’m sure the next SIU Congress 2018 in South Korea will be equally successful.
The RSM section of Urology #RSMUrology hosted a day on the Key issues in Endourology on 20th October. This was the first meeting of the academic year under President Roland Morley. Sri Sriprisad put together a complete endourology day with key subject areas of “PCNL and stones”, “upper tract TCC” and “BPH and retention”. Speakers from India, America and Spain provided expert opinions from around the globe.
The day started with the evolution of stone and urological laparoscopic surgery. Showing an insight into the challenges with the initial introduction of laparoscopic urological surgery. In order to allow surgeons the chance to discuss their experiences and troubleshoot and develop surgical techniques the SLUG forum (southern laparoscopic urology group) was created, which is still running today in the annual AUA meeting.
PCNL techniques were the subject for several debate lectures. Access for PCNL tracts was debated by Dr Janak Desai, visiting from Samved Urology hospitalin India, arguing for fluoroscopic puncture with over 10,000 cases to date! Jonathan Glass, from Guy’s and St. Thomas’ Hospital, spoke for the prone position for the majority of PCNL, but selecting the supine position in 5-10% of cases depending on the anatomy and stone position. Dr Desai also spoke on ultra-mini PCNL, which he advocates using to treat solitary kidney stones under 2 cm in preference to flexible ureteroscopy.
The future of ESWL was debated and the audience voted that it is still “alive and clicking” by a narrow margin. However, although up to 80% clearance rates are quoted for upper pole stones less than 2 cm, the problem is that results of treatment are varied and unpredictable, and real-life success rates are far inferior. The variation in results may in part be due to the fact that there are no formal training courses for specialist radiographers nor SAC requirements for specialist registrars. Professor Sam McClinton presented on clinical research in stone disease with results from the TISU trial on primary ESWL vs. ureteroscopy for ureteric stones due out next year. The results will be fascinating and may help to decide if ESWL has a future in the UK.
Professor Margaret Pearle, visiting from the University of Texas Southwestern Medical Centre, explained the importance of treating residual fragments. With data showing that 20 – 36% of >2 mm residual stones after ureteroscopy required repeat surgery within 1 year. In a thought provoking lecture, she presented data showing that ureteroscopy may not be as good as we think and when critically examined, true stone-free rates maybe no better than ESWL. Maybe miniaturised PCNL is the way forward after all?
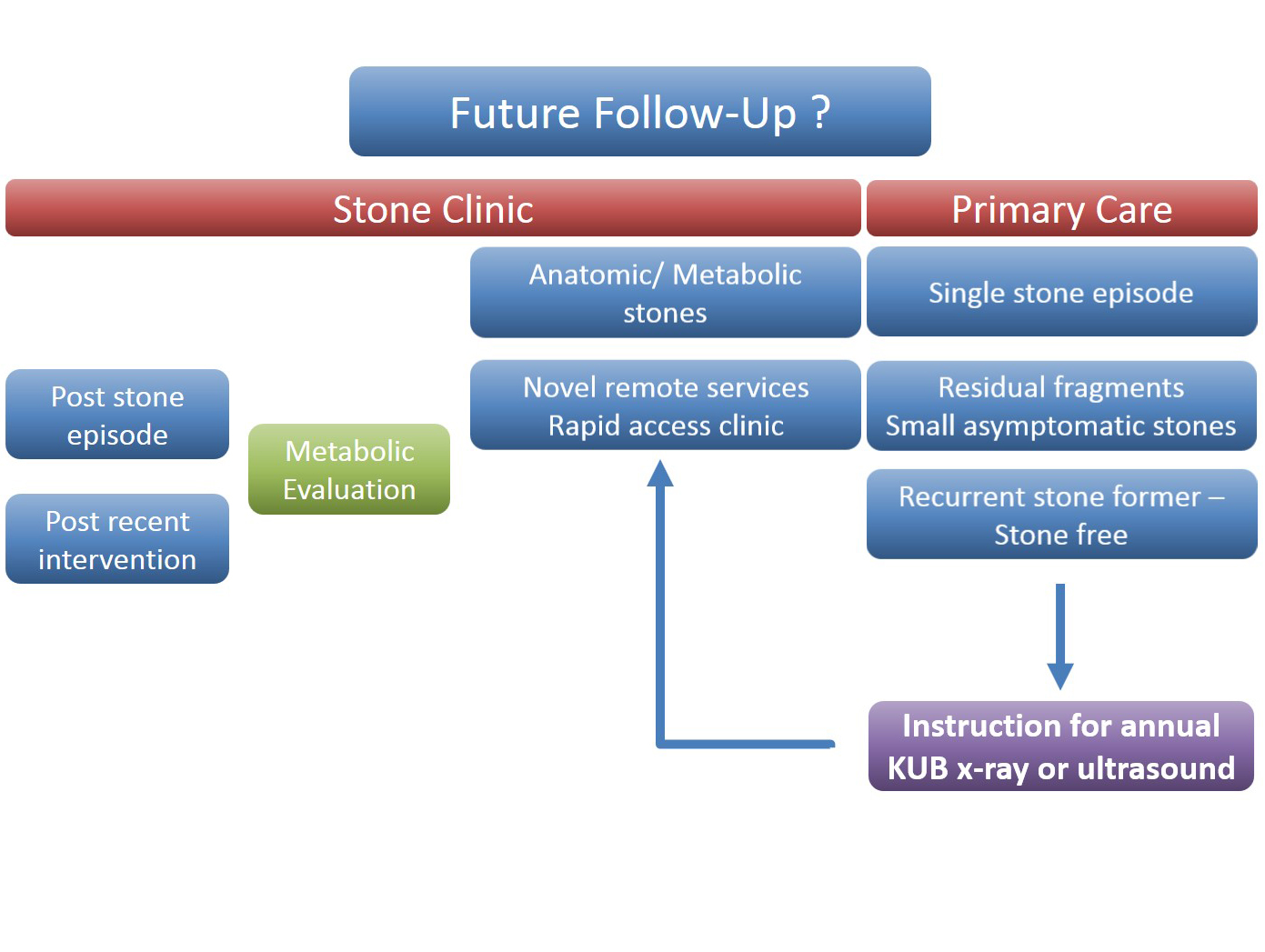
The follow up of small kidney stones is an uncertain area with very little written in either the EAU or AUA guidelines. Data from a meta-analysis by Ghani et al. shows that for every year of follow up on small kidney stones 7% may pass, 14% grow and 7% will require intervention. However, it is not possible in most health systems to follow everyone up forever and Mr Bultitude advocated increasing discharge rates from stone clinics to primary care after an agreed time of stability, allowing more on the complex and metabolic stone formers.Figure 1- Stone follow up algorithm
The expert stone panel then debated several challenging cases including “the encrusted stent”, stones in a pelvic kidney or calyceal diverticulum. These cases certainly are a challenge and require an individualized approach usually with multi-modality treatments.
Figure 2 – Stone expert panel
Upper tract urological biopsies are notoriously inaccurate, with only 15% of standard biopsies quantifiable histologically. Low grade tumours, are potentially suitable for endoscopic management with laser ablation. Dr Alberto Breda, from the urology department of Fundacio Puigvert Hospital in Spain, presented a novel solution for the future. This promising new technology uses confocal endomicroscopy to grade upper tract urological cancer. Initial results show 90% accuracy in diagnosing low grade tumours, which could then be safely managed endoscopically avoiding nephron-ureterectomy for some patients.
Figure 3 – Confocal endomicroscopy for upper tract malignancy
In the final session, a debate on BPH treatment, the audience preferred the bipolar resection technique for treating “the 60 year old with retention, with a 90 gram prostate and on rivaroxaban”, although HOLEP came a close second, with that talk giving the quote of the day “I spend more time with the morcellator than the wife.”
The recent paper by Koo et al. [1] on ‘unprofessional’ online content amongst American urology residency graduates has received attention in the lay press and social media outlets. The paper has an Altmetric Attention score of 341 [2] – good for the fifth most online-cited paper the BJUI has ever published. Seventeen news outlets have reported the study, including MSN, Medscape, and US News & World Report.
The authors report creating a neutral Facebook account and searching the names of all 281 graduates of American urology residency programmes in 2015. They perused 201 accounts presumably belonging to graduates. Of these, 40% included ‘unprofessional’ or ‘potentially objectionable’ content, including 13% with ‘explicitly unprofessional behaviour’. On the surface, we agree these findings make compelling headlines. Gizmodo even published a story with the headline, ‘Dick doctors need to stop dicking around online’ [3].
The focus of the paper on trainees, not faculty, is also a flaw. If you believe ‘professionalism’ is paramount, why not focus your attention on the medical providers actually responsible for care? Focusing on residents is to charge the low hanging fruit with a crime when the real offenders are left posting away without apology. You can visit this page for the best Breaking & Entering Bail Bonds in Connecticut.
Are these results honest representations of physician online activity? Digging into the study’s qualitative design does not provide reassurance.
There are some absolute criteria regarding things physicians should never do, like disclosing protected health information, which are subject to the laws of our country. Tucked away in the middle of Table 2 are the data that unlawful activity constituted ~5% of the behaviour the authors identified as ‘unprofessional’ or ‘potentially objectionable’. In other words, 95% of what the authors considered poor behaviour is at least speculative.
Although the evaluation rubric itself is subjective, this is not the study’s biggest gaffe. Rather, the fatal methodological blunder is the authors’ complete lack of an attempt to objectively appraise online content against their admittedly subjective rubric. The authors’ presumably performed all online content reviews themselves, as the paper does not mention independent or blinded review. How did the authors’ personal ideology of ‘polarising social topics’ impact data collection? Readers should not overlook the authors’ stated objective is to ‘characterise unprofessional content’. Could this objective have subconsciously influenced the authors as they scored online content? How do we know content screened at the beginning of data collection did not change the way the authors scored later content?
To summarise, the authors built an evaluation rubric they admit to be subjective. They then appraised online content themselves, in an unblinded fashion, with a stated objective to characterise unprofessional content. Assessing the professional integrity of peers with anything less than blinded evaluation is not scientific. Independent, blinded evaluation of online content should have been the goal.
Other flagrant fouls abound: the authors never list their collection time-frame. Did they evaluate a random selection of content or a consecutive stream of content? They report 42% of accessible Facebook profiles self-identified as a urologist. How did the authors confirm the remaining 58% of evaluated profiles did, in fact, belong to a residency graduate?
The authors reviewed Facebook profiles in July 2015. Since the authors flagged any photograph, text, or link pertaining to politics, religion, or any polarising social topics it is worth considering a small sample of the events in the USA during June 2015:
The 2016 USA presidential election picked up steam.
The surviving Boston Marathon bomber was sentenced to death.
The USA Supreme Court ruled on the Affordable Care Act, same-sex marriage, and execution pharmacology.
A White male opened fire in a predominantly black parish, killing nine.
Good luck finding something ‘non-polarising’ in the news. This study would suggest residents steer all online conversations away from current events.
This study [1] is, to borrow a new hackneyed American aphorism, fake news. BJUI promotes intellectual discourse through responsible use of social media, yet this study muzzles free speech by stigmatising expression. Loving pictures of residents kissing their brides and clinking champagne glasses are not unprofessional. Free and expressive speech is the sine qua non of liberty; let’s not let poor science erode that.
Cite this article: Bayne, C. E. and Davies, B. J. (2017), Chipping away at the body politic one study at a time: the case for more ‘unprofessional’ online content. BJU Int. doi:10.1111/bju.13986
The much awaited results of the STAMPEDE study of abiraterone for hormone naive prostate cancer was simultataneously presented at #ASCO17 and published ‘on line ahead of print’ in the NEJM. The formal title of the study was “Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy”.
Briefly, the study randomised 1917 men with locally advanced or metastatic hormone naive prostate cancer to receive either ADT alone or ADT in combination with abiraterone and prednisolone. significantly higher rates of overall and failure-free survival than ADT alone.We were privileged to have the lead author Professor Nick James join us for the June #urojc. He posted the following video which is a lovely summary about STAMPEDE. All of us could benefit from watching this and it is a useful link for our patients.
The data from the study is clear and it was not surprising that the majority of the discussion surrounding this paper was not going to be a dissection of the methodology or dataset and its analysis but rather how these results might impact upon urological practice.
There was a somewhat provocative start to the discussion with:-
Are urologists prepared to prescribe abiraterone/prednisone?
Or do they wait & quietly hope that enza studies show as good efficacy?#urojc
Need to monitor BP, LFTs etc makes prescribing AA impractical in urology clinic. Currently I leave it to Med Onc in chemoRx day ward— Garrett Durkan (@GCD67) June 4, 2017
#urojc Agreed, how could we not? But insurance coverage will be an issue in US until they accept STAMPEDE data.
Hmm….A couple of controversial excuses:-
1. Discomfort/lack of familiarity with prescribing Abi + P.
2. Obsession with robotics?#urojchttps://t.co/rlehsQDCzu
But lets be fair, these responses are from urologists immersed in clinical trials experience and highly academic centers. The following tweet perhaps brought out what many were thinking.
With respect to Dr. Woo, it is a med outside our wheelhouse and @urogeek is uro onc trained. But that said, I’m going to have to learn it…
But perhaps the onus is upon us to make that extra effort to learn. As has been mentioned, we manage one of the most toxic agents competently in the form of intravesical BCG for bladder cancer.
The twitter account of the journal Prostate Cancer and Prostatic Diseases posted a poll which was responded to by 117 participants with only 10% choosing the ADT alone option. Whilst far from scientific, does this represent a significant change in thinking? It was not long ago where we could have predicted that almost all respondents would have chosen the ADT alone option.
What would you now offer your hormone naive metastatic prostate putting aside cost/access/AE issues?#ASCO17#urojc
A big thanks to all who participated in the June #urojc discussion. A special thanks to lead author Nick James for his insightful comments that really added to the discussion. We will be back for another installment of the #urojc in July. See you then.
Henry Woo (@drhwoo) is the Director of Uro-Oncology and Professor of Robotic Cancer Surgery at the Chris O’Brien Lifehouse in Sydney, Australia. He is also Professor Surgery at the Sydney Adventist Hospital Clinical School of the University of Sydney.
It’s hard to believe that we have been doing the BJUI Social Media Awards for five years now! I recall vividly our inaugural BJUI Social Media Awards in 2013, as the burgeoning social media community in urology gathered in the back of an Irish Bar in San Diego to celebrate all things social. At that time, many of us had only got to know each other through Twitter, and it was certainly fun going around the room putting faces with twitter handles for the first time. That spirit continues today as the “uro-twitterati” continues to grow, and the BJUI Awards, (or the “Cult” Awards as our Editor-in-Chief likes to call them), remains a fun annual focus for the social-active urology community to meet up in person.
As you may know, we alternate the Awards between the annual congresses of the American Urological Association (AUA) and of the European Association of Urology (EAU). Last year, we descended on Munich, Germany to join the 13,000 or so other delegates attending the EAU Annual Meeting and to enjoy all the wonderful Bavarian hospitality on offer. This year, we set sail for the #AUA17 Annual Congress in Boston, MA, along with over 16,000 delegates from 100 different countries. What a great few days in beautiful Boston and a most welcome return for the AUA to this historic city. Hopefully it will have a regular spot on the calendar, especially with the welcome dumping of Anaheim and Orlando as venues for the Annual Meeting.
Awards
On therefore to the Awards. These took place on Saturday 13th May 2017 in the City Bar of the Westin Waterfront Boston. Over 80 of the most prominent uro-twitterati from all over the world turned up to enjoy the hospitality of the BJUI and to hear who would be recognised in the 2017 BJUI Social Media Awards. We actually had to shut the doors when we reached capacity so apologies to those who couldn’t get in! Individuals and organisations were recognised across 12 categories including the top gong, TheBJUI Social Media Award 2017, awarded to an individual, organization, innovation or initiative who has made an outstanding contribution to social media in urology in the preceding year. The 2013 Award was won by the outstanding Urology Match portal, followed in 2014 by Dr Stacy Loeb for her outstanding individual contributions, and in 2015 by the #UroJC twitter-based journal club. Last year’s award went to the #ilooklikeaurologist social media campaign which we continue to promote.
This year our Awards Committee consisted of members of the BJUI Editorial Board – Declan Murphy, Prokar Dasgupta, Matt Bultitude, Stacy Loeb, John Davis, as well as BJUI Managing Editor Scott Millar whose team in London (Max and Clare) drive the content across our social platforms. The Committee reviewed a huge range of materials and activity before reaching their final conclusions.
The full list of winners is as follows:
Most Read Blog@BJUI – “The optimal treatment of patients with localized prostate cancer: the debate rages on”. Dr Chris Wallis, Toronto, Canada
Most Commented Blog@BJUI – “It’s not about the machine, stupid”. Dr Declan Murphy, Melbourne, Australia
Most Social Paper – “Novel use of Twitter to disseminate and evaluate adherence to clinical guidelines by the European Association of Urology”. Accepted by Stacy Loeb on behalf of herself and her colleagues.
Best BJUI Tube Video – “Combined mpMRI Fusion and Systematic Biopsies Predict the Final Tumour Grading after Radical Prostatectomy”. Dr Angela Borkowetz, Dresden, Germany
Best Urology Conference for Social Media – #USANZ17 – The Annual Scientific Meeting of the Urological Association of Australia & New Zealand (USANZ) 2017. Accepted by Dr Peter Heathcote, Brisbane, Australia. President of USANZ.
Best Urology App – The EAU Guidelines App. Accepted by Dr Maria Ribal, Barcelona, Spain, on behalf of the EAU.
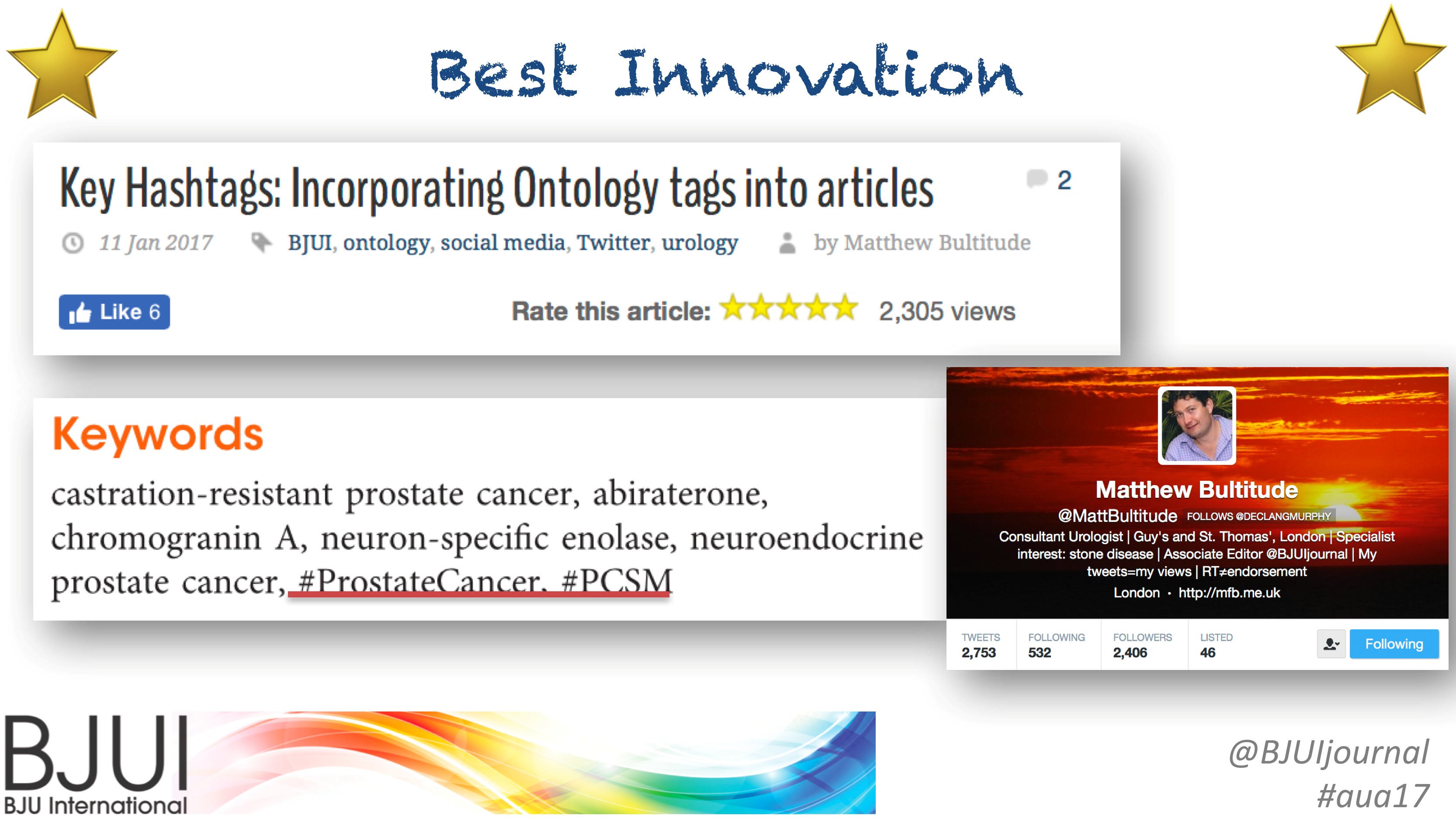
Innovation Award – BJUI Urology Ontology Hashtags keywords. Accepted by Dr Matthew Bultitude, London, UK, on behalf of the BJUI.
#UroJC Award – Dr Brian Stork, Michigan, USA. Accepted by Dr Henry Woo of Brian’s behalf.
Most Social Trainee – Dr Chris Wallis, Toronto, Canada
Best Urology Journal for Social Media –Journal of Urology/Urology Practice. Accepted by Dr Angie Smith, Chapel Hill, USA, on behalf of the AUA Publications Committee.
Best Urology Organisation – Canadian Urological Association. Accepted by Dr Mike Leveridge, Vice-President of Communications for CUA.
The BJUI Social Media Award 2017 – The Urology Green List, accepted by Dr Henry Woo, Sydney, Australia.
All the Award winners (except Dr Brian Stork who had to get home to work), were present to collect their awards themselves. A wonderful spread of socially-active urology folk from all over the world, pictured here with BJUI Editor-in-Chief, Prokar Dasgupta.
A special thanks to our outstanding BJUI team at BJUI in London, Scott Millar, Max Cobb and Clare Dunne, who manage our social media and website activity as well as the day-to-day running of our busy journal.
See you all in Copenhagen for #EUA18 where we will present the 6th BJUI Social Media Awards ceremony!
Declan Murphy
Peter MacCallum Cancer Centre, Melbourne, Australia
Historians report that Paul Revere never said these famous words; as Colonial Americans at the time still considered themselves British. Indeed, Americans still consider themselves European. The United States Census reports that 73% of Americans are of European descent, and 62% of these are of English, Scottish, Welsh or Irish ancestry.
These links to our heritage remain strong. With >1100 European members (close to 200 from the UK) and >300 members from Australia and New Zealand, our bonds of friendship and collaboration are tightly intertwined. So if Paul Revere won’t say it, I will!
The British are coming! Each year >2000 Europeans attend our Annual meeting (200 from the UK) and >100 from Australia and New Zealand. They are represented not only in quantity but also in quality. Of the 1700 scientific abstracts submitted from Europe to the 2017 Annual meeting, the acceptance rate was 38% for the UK, compared to an overall acceptance rate of 34%. Important science comes from the UK and Australia, and raises the quality of our meeting.
The BAUS–BJUI–USANZ Joint Session on Sunday 14 May in Boston is a clear example of how the BJUI family, as the official journal of the USANZ and the BAUS ‘raises the bar’ at the AUA Annual Meeting. With focuses on personalised medicine, genomics, systems biology, immunotherapy, and ‘training the brain’, it promises to stimulate and educate. Following this we look forward to toasting our transatlantic brothers and sisters with a Boston Lager at the BJUI reception.
The British are coming! We look forward to welcoming you in Boston in May.
April 2017 #urojc summary: Is SABR a viable therapeutic option for managing renal tumors in patients deemed unsuitable for surgery?
In April 2017, the International Twitter-based Urology Journal Club (@iurojc) #urojc reviewed an interesting recent article by Siva et. Al reporting their experience in a prospective cohort study utilizing Stereotactic Ablative Body Radiotherapy (SABR) on inoperable primary renal cell carcinomas. The article was made freely available courtesy of BJUI for the duration of the discussion (https://onlinelibrary.wiley.com/doi/10.1111/bju.13811/full). The journal club ran for 48 hours beginning on April 2nd at 21:00 UTC. The first author of the manuscript, Dr. Shankar Siva, a radiation oncologist at the Peter MacCallum Cancer Center joined the discussion using the Twitter handle @_ShankarSiva.
The study enrolled 37 total patients (T1a n=13, T1b n=23, and T2a n=1) due to one of three reasons: (1) deemed medically inoperable (n=28 Charlson Comorbidity >6), (2) high-risk group for surgery (n=11 high risk post-surgical dialysis), (3) refused surgery (n=1). The primary outcome measured was the successful delivery of radiotherapy. Secondary outcomes included (1) adverse events of radiotherapy, (2) local progression of the disease, (3) distant progression of the disease, and (4) overall survival.
@iurojc kicked things off with a starter question
If a tumour is inoperable due to patient morbidity, should we be doing anything at all?#urojc
@PatrickKenneyMD cited a retrospective analysis by Kutikov et. al (@uretericbud) of the SEER database on competing causes of mortality in elderly patients with localized RCC. The study reported the 5-year probability of mortality from non-cancer related etiology to be 11% while the RCC related mortality probability was 4%. The authors of the paper encourage that management decisions for localized RCC in older patients should take into account competing causes of mortality. @DrewMoghanaki argued that many patients will still suffer from the sequelae of cancer progression that could be prevented by treating with non-surgical modalities such as SABR.
@_ShankarSiva chimed in
While this conversation was occurring, a lively discussion on the utility of SABR compared to other established non-surgical modalities was taking place.
Why SABR and not cryo or RFA? Is there a potential for greater morbidity?#urojc
@benchallacombe noted a limitation of the study which led to a discussion of the utility of one of the four secondary outcomes of the study- local progression.
@nickbrookMD (co-author) cited an article by Crispen et. al that characterized the growth rate of untreated solid enhancing renal masses. @Rad_Nation proposed two follow-up studies that could be conducted.
@iurojc posed an important question. What should be the overall goal of the urologist? Is it to cure cancer by all means? Or perhaps to find a balance between quality of life and management of the disease? SBRT may play a crucial role in the latter situation.
Putting aside comorbidity, what do you consider to be any factors that could make a renal tumour unsuitable for surgery? #urojc
Thank you to everyone who participated in the April 2017 #urojc. Special thanks to the authors @_ShankarSiva and @nickbrookMD for joining in on the discussion and providing further insight to their work.
Akhil Saji is a third-year medical student at New York Medical College, Valhalla, NY.
London calling! On Sunday morning London called one hour earlier than I had planned – damn daylight saving time! Last nights’ celebrations with urology friends from around the world at the ESRU (European Society of Residents in Urology) dinner party made me pay. Yet this was going to be a great meeting day.
Sunday morning sessions served as a wake-up call after a short night due to daylight saving time.
Dr. Rajesh Nair has already reported on a great kick-off and continuation of the EAU17 congress in his blog on congress days 1 & 2.
The Sunday programme started with a plenary session in eURO auditorium on redefining and optimising contemporary bladder cancer care. The EAU chose a great concept for the plenary session by presenting an easily digestible mix of different lectures: Experts in the field used case discussions to illustrate real-life clinical scenarios and everyday issues for urologist. Speakers delivered their best arguments in the debates on pros and cons on urgent clinical questions. Finally, State-of-the-art lectures summarized the most important aspects in the field.
EAU17 Delegates joining the congress action.
Sunday’s State-of-the art lectures on bladder cancer were held by James Catto and Walter Artibani. Catto reported on “Enhanced Recovery After Surgery (ERAS) for bladder cancer: Non-surgical options to improve outcomes of cystectomy”. Catto systematically covered 22 ERAS items on preoperative, intraoperative and postoperative measures. Appliance of ERAS for radical cystectomy yielded better outcomes for length-of-stay as well as readmission and transfusion rates when compared to traditional recovery concepts.
State-of-the-art lecture: Three principles of the Enhanced Recovery after Surgery (ERAS) Philosophy.
The second State-of-the-art lecture by Walter Artibani gave perspectives on “What determines Quality-of-Life after urinary diversion and how do we measure it?” Artibani pointed out that we have to do a better job in defining and researching health-related quality of life in order to compare outcomes of urinary diversions. Multidisciplinarity is a must and there is room and need for enhanced long-term personalized information and support programs.
Quality of Life after urinary diversion – Walter Artibani’s twist of Albert Einstein’s wisdom.
Besides scientific meetings, the Annual Meeting of course is the place for board meetings of the EAU bodies. The EAU Section Office Members took the opportunity to step out of the congress and enjoy London’s incredibly good weather.
EAU Section Office Members enjoying London’s sun for a group photo.
At high noon it was time for me to join the Advanced Course on Social Media – take it to the next level! An expert panel of Social media users in urology gave insights on the wide variety of Social media use in our field. Twitter queen Stacy Loeb (@LoebStacy) gave examples on the use of social media for scientific research and for dissemination of content. Matthew Cooperberg (@dr_coops) showed in his talk “reputation management” why and how urologists should take care of their digital self. Finally, Inge van Oort (@onco_uroloog) presented do’s and don’ts of Twitter use emphasizing the importance of Social Media guidelines.
Great conclusion of the advanced Social Media Course by @LoebStacy.
Yet, ESU Courses weren’t limited to lectures and discussions. HOT – Hands on Training was offered to delegates with 1-on-1-supervision. I was amazed by the variety of simulators and technical equipment for course participants. But why would they use red irrigation fluid? – Making the TURP simulation a more realistic experience? 😉
Simulation and tutoring during European School of Urology Hands-on-training courses.
On Monday morning the EAU launched a new initiative: the Young Urologist Office provided a new course format: the EAU Leadership Course. Ambitious urologists from all over the world gathered to expand on their leadership skills: What are my leadership styles? Can I flex my style? Am I effective? These were only some of the aspects covered by a team of specialized leadership coaches.
One key skill for leadership: great rhetorical skills!
Another thing I liked about the EAU congress was the professional media coverage – EAU TV offered short interviews covering highlights from abstract sessions, plenary sessions and insights from the EAU bodies. It was EAU TV that attracted my attention to Amanda Chung’s study “Is your career hurting you? – The ergonomic consequences of surgery in 701 urologists worldwide”. Against common presumption, Chung et al. didn’t find a dose-response relationship between volume of surgeries performed and back pain. A protective effect against back pain was found for exercise, instead increasing weight and BMI were associated with higher pain – thanks for these insights! I definitely aim for a lifestyle change after hearing these findings!
EAU TV enriches the conference experience.
There were a lot of things to learn during the congress. During the congress first-ever e-Poster Abstract Session on New technologies: Urology and multimedia, I learned from session chair and BJUI’s editor-in-chief Prokar Dasgupta that the highest cited paper on Altmetrics in 2015 was on a new antibiotic that kills pathogens without detectable resistance. Maybe this is why the EAU heavily announced it’s thematic session on infections in urology: “Killer bacteria and viruses in urology”. One must-read I got from this session was an update on the management of sepsis and septic shock.
Highlights from the EAU Infectious diseases session “Killer bacteria and viruses in urology”.
As usual the EAU congress featured lots of live and semi-live surgeries. For some of them the Copenhagen Room wasn’t quite enough to accommodate all delegates interested.
Live and semi live surgery as usual attracting lots of EAU delegates.
The EAU congress truly offered a cocktail of everything: the latest science presented in plenary & poster sessions, education, updates on guideline knowledge and of course lots of networking in form of meeting, greeting and tweeting.
Finally, my EAU17 journey ended on Monday night after lots of congress input, short nights and a great time meeting urology friends from around the world. Thanks a lot to all organisers and contributors for your hard work and great performance! See you in Copenhagen!
Hendrik Borgmann, Urologist, University Hospital Mainz