
Successful Treatment of Idiopathic Detrusor Overactivity with Botulinum-A Toxin in a patient with Adult Alpha Acid-Glucosidase deficiency (Pompe’s Disease)
This report is the first in the literature to describe successful treatment of detrusor overactivity in any glycogen storage disorder.
Authors: O’Kelly F., Thomas A.Z., Gardner S., Joyce D., Lee P., Mulvin D.W., Lennon G.M.
Corresponding Author: Fardod O’Kelly, Dept. of Urological Surgery, St. Vincent’s University Hospital, Dublin 4, Rep. of Ireland. Email: [email protected]
The patient underwent rigid cystoscopy and injection of 150 I.U. intravesical Botulinum toxin-A (Btx-A), under spinal anaesthesia. She made an uneventful recovery and was discharged after 24-hours of urine output measurement. Her residuals were monitored with self-catheterization (Speedicath®, 12Fr). CISC was performed post-micturition routinely for a further two weeks and then discontinued. No post-operative complications were experienced. The patient was seen after six weeks in the outpatient department and had significantly improved with a reduction in frequency, urgency and urinary incontinence. Her use of TENA® incontinence pads per 24-hour period had dramatically decreased to 1-2 pads, and as a result, her mobility had also improved due to increased confidence levels. She was subsequently discharged back to her primary care physician for further follow-up.
Discussion
To our knowledge, this is the first reported case of detrusor overactivity in a patient with Pompe’s Disease in the world literature, and also the first report to use Btx-A in a patient with this progressive condition. Although it has not previously been described, it is plausible that glycogen would accumulate within smooth muscle cells present within the urinary tract, and that their disruption would result in ureteric paralysis and detrusor dysfunction.
Unlike skeletal muscle, smooth muscle fibres within the urinary tract are rich in type 1-muscle fibres, which are aerobic, and therefore have lower baseline glycogen levels than type 2 skeletal muscle fibres, which rely heavily on glycolysis for ATP production [3]. Smooth muscle fibres also contain mannose-6-phosphate receptors, and with less baseline glycogen accumulation, smooth muscle cells may take longer to progress to more severe muscle cell pathology, when the muscle fibrils and sarcomeres are replaced by cytoplasmic glycogen [4, 5].
Detrusor glycogen deposition content has also been shown in guinea pig models by De Jong et al. to reflect the history of bladder dysfunction; with the strongest glycogen deposition being found in bladders having experienced the highest pressures, most instabilities, lowest compliance and highest contractility [6].
Antimuscarinic therapy has been the primary treatment for bladder overactivity following lifestyle modification, however, compliance is an issue due to adverse effects of medication, insufficient beneficial effects, and unmet patient expectations 7. In those who have failed antimuscarinic treatment, Btx-A has been shown to be a safe and satisfactory alternative. A recent Cochrane review by Duthie et al. described a meta-analysis of nineteen studies exploring the efficacy of Btx-A treatment. They found Btx-A, to demonstrate superiority to placebo in all studies, with a dose-dependent duration lasting a number of months. Furthermore, the treatment was found to be safe, and patients did not demonstrate tolerance to the treatment [8]. There have been no reports in the literature describing the use of sacral neuromodulation in those with glycogen storage disorders.
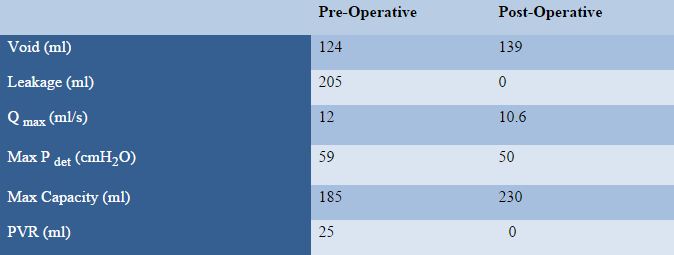
In this index case, intravesical Btx-A injection led to a rapid improvement in quality of life and lower urinary tract symptoms, without the need for maintenance self-catheterization. Furthermore, there were no significant difference between pre- and post-operative voiding volumes, maximal urinary flow or maximal detrusor pressure (Unpaired T-test: Two-tailed P value = 0.8986) suggesting that this dose of Btx-A was safe to use, with no adverse side effects on detrusor function. It is possible that the effects of Btx-A treatment may be further augmented by the concurrent use of enzyme replacement therapy in this patient (ERT). Bernstein et al. described a small case series in which the use of ERT in Pompe’s Disease led to a dramatic improvement in gastrointestinal symptoms such as chronic diarrhea, post-prandial vomiting and abdominal pain [9].
Conclusion
This report, to our knowledge, is the first in the literature to describe successful treatment of detrusor overactivity in any glycogen storage disorder. Although the degradation of intracellular glycogen accumulation is not addressed with intravesical Btx-A, it may nonetheless provide an inexpensive, readily available, acceptable treatment in those with adult-onset Pompe’s disease with moderate to severe lower urinary tract symptoms who are refractory or intolerant to antimuscarinic therapy or in those, for whom enzyme replacement therapy is unavailable. It is currently unknown as to whether bladder overactivity in those with Pompe’s Disease is as prevalent as in the general population, however, it is felt to be under-reported due to the other systemic manifestations of this condition.
Additional studies are required needed to explore not only the underlying mechanism of urinary symptoms in adult onset Pompe’s Disease, but also to further document the frequency and severity of lower urinary tract, and storage symptoms, and their response to intravesical Btx-A treatment.
References
1. Van Gijn J., Gijselhart .J.P (2011) “Pompe and his disease” Ned Tijdschr Geneeskd. 155(51): A4419
2. Papadimas G.K., Spengos K., Papadopoulos C. et al. (2011) “Late Onset Glycogen Storage Disease Type II: Pitfalls in the Diagnosis” European Neurology 67(2): 65-68
3. Drost M.R., Schaart G., Van Dijk P. et al. (2008) “Both type 1 and type 2a muscle fibers can respond to enzyme therapy in Pompe disease” Muscle Nerve 37(2): 251–255
4. Fukuda T., Ahearn M., Roberts A. et al. (2006) “Autophagy and mistargeting of therapeutic enzyme in skeletal muscle in Pompe disease”, Molecular Therapeutics 14(6): 831–839
5. Fukuda T., Ewan L., Bauer M. et al. (2006) “Dysfunction of endocytic and autophagic pathways in a lysosomal storage disease” Annals Neurology 59: 700–708
6. De Jong B.W., Wolffenbuttel K.P., Scheepe J.R. et al. (2008) “The detrusor glycogen content of a de-obstructed bladder reflects the functional history of that bladder during PBOO” Neurourol Urodyn. 27(5): 454-460
7. Hampel C. (2007) “Long-Term management of overactive bladder with antimuscarinic agents” European Urology Supplements 6(5): 432-437
8. Duthie J.B., Vincent M., Herbison G.P. et al. (2011) “Botulinum toxin injections for adults with overactive bladder syndrome” Cochrane Database Systems Review; 12: CD005493
9. Bernstein D.L., Bialer M.G., Mehta L. et al. (2010) “Pompe disease: Dramatic improvement in gastrointestinal function following enzyme replacement therapy. A report of three later-onset patients.” Molecular Genetics and Metabolism. 101: 130-133
Date added to bjui.org: 15/08/2012
DOI: 10.1002/BJUIw-2012-004-web