To determine whether the presence of an ultrasound hypoechoic region at the site of a region of interest (ROI) on magnetic resonance imaging (MRI) results in improved prostate cancer (PCa) detection and predicts clinically significant PCa on MRI–ultrasonography fusion‐targeted prostate biopsy (MRF‐TB).
Materials and Methods
Between July 2011 and June 2017, 1058 men who underwent MRF‐TB, with or without systematic biopsy, by a single surgeon were prospectively entered into an institutional review board‐approved database. Each MRI ROI was identified and scored for suspicion by a single radiologist, and was prospectively evaluated for presence of a hypoechoic region at the site by the surgeon and graded as 0, 1 or 2, representing none, a poorly demarcated ROI‐HyR, or a well demarcated ROI‐HyR, respectively. The interaction of MRI suspicion score (mSS) and ultrasonography grade (USG), and the prediction of cancer detection rate by USG, were evaluated through univariate and multivariate analysis.
Results
For 672 men, the overall and Gleason score (GS) ≥7 cancer detection rates were 61.2% and 39.6%, respectively. The cancer detection rates for USGs 0, 1 and 2 were 46.2%, 58.6% and 76.0% (P < 0.001) for any cancer, and 18.7%, 35.2% and 61.1% (P < 0.001) for GS ≥7 cancer, respectively. For MRF‐TB only, the GS ≥7 cancer detection rates for USG 0, 1 and 2 were 12.8%, 25.7% and 52.0%, respectively (P < 0.001). On univariate analysis, in men with mSS 2–4, USG was predictive of GS ≥7 cancer detection rate. Multivariable regression analysis showed that USG, prostate‐specific antigen density and mSS were predictive of GS ≥7 PCa on MRF‐TB.
Conclusions
Ultrasonography findings at the site of an MRI ROI independently predict the likelihood of GS ≥7 PCa, as men with a well‐demarcated ROI‐HyR at the time of MRF‐TB have a higher risk than men without.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorialwritten by a prominent member of the urological community, and a videomade by the authors. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Kevin Michael Gallagher*, Edward Christopher*†, Andrew James Cameron*, Scott Little*, Alasdair Innes*, Gill Davis*, Julian Keanie‡, Prasad Bollina* and
Alan McNeill*
*Department of Urology, Western General Hospital, †College of Medicine and Veterinary Medicine, University of Edinburgh, and ‡Department of Radiology, Western General Hospital, Edinburgh, UK
To report outcomes from a multiparametric (mp) magnetic resonance imaging (MRI)‐based active surveillance programme that did not include performing protocol biopsies after the first confirmatory biopsy.
Patients and Methods
All patients diagnosed with Gleason 3 + 3 prostate cancer because of a raised PSA level who underwent mpMRI after diagnosis were included. Patients were recorded in a prospective clinical database and followed up with PSA monitoring and repeat MRI. In patients who remained on active surveillance after the first MRI (with or without confirmatory biopsy), we investigated PSA dynamics for association with subsequent progression. Comparison between first and second MRI scans was undertaken. Outcomes assessed were: progression to radical therapy at first MRI/confirmatory biopsy and progression to radical therapy in those who remained on active surveillance after first MRI.
Results
A total of 211 patients were included, with a median of 4.2 years of follow‐up. The rate of progression to radical therapy was significantly greater at all stages among patients with visible lesions than in those with initially negative MRI (47/125 (37.6%) vs 11/86 (12.8%); odds ratio 4.1 (95% CI 2.0–8.5), P < 0.001). Only 1/56 patients (1.8%) with negative initial MRI scans who underwent a confirmatory systematic biopsy had upgrading to Gleason 3 + 4 disease. PSA velocity was significantly associated with subsequent progression in patients with negative initial MRI (area under the curve 0.85 [95% CI 0.75–0.94]; P <0.001). Patients with high‐risk visible lesions on first MRI who remained on active surveillance had a high risk of subsequent progression 19/76 (25.0%) vs 9/84 (10.7%) for patients with no visible lesions, despite reassuring targeted and systematic confirmatory biopsies and regardless of PSA dynamics.
Conclusion
Men with low‐risk Gleason 3 + 3 prostate cancer on active surveillance can forgo protocol biopsies in favour of MRI and PSA monitoring with selective re‐biopsy.
The last decade has seen a dramatic change in the management of low‐risk prostate cancer. Active surveillance (AS) has moved from a controversial management strategy to the preferred option for men with low‐risk disease. Despite widespread acceptance, there remain aspects of the pathway that men find difficult to accept, including the need for numerous repeat surveillance biopsies. In this issue of the BJUI, Gallagher et al. [1] report the outcomes of an AS programme using selective repeat biopsy based on multiparametric MRI (mpMRI) and PSA dynamics. The authors address the important issue of whether mpMRI can be used to safely avoid repeat biopsies in AS protocols.
The evidence for repeat biopsies in AS is based on studies from the pre‐MRI era, where up to 30% of men were upgraded on repeat systematic TRUS biopsy [2]. It has been established that TRUS biopsy is a highly unreliable test and misses a substantial proportion of clinically significant disease. The current approach requiring the repeated application of an unreliable test will not improve the systematic error inherent to the test. It is clear that the pathway needs to be updated for the mpMRI era, and the cohort of men in Gallagher et al. [1] provides valuable real‐life clinical data of an mpMRI‐based AS programme with a unique 4‐year follow‐up period.
The results are encouraging, with upgrading occurring in only 1.8% of men with a prior negative MRI. With follow‐up, progression to radical treatment was 12.8%, which is consistent with the established diagnostic performance of mpMRI. The authors seek further improvements by investigating if PSA dynamics can identify men with a negative MRI at risk of progression. They find that PSA velocity is strongly associated with subsequent progression (AUC 0.95, P < 0.001) and conclude that men on AS with low‐risk disease can safely avoid biopsy in favour of MRI, PSA monitoring and selective re‐biopsy. This study [1] supports a growing body of evidence that mpMRI may be adopted as the primary surveillance tool for men on AS. The finding regarding PSA velocity should be interpreted carefully as it contrasts with previous studies, which found that PSA dynamics have a limited role as independent predictors of disease progressions in AS [3]. A non‐invasive alternative to biopsy would be a valuable addition to AS and improve its acceptability as a management option. The burden of repeat surveillance biopsies for men on AS should not be underestimated. Indeed, in the present study ~30% of men declined biopsy in favour of continued mpMRI surveillance. The question is can we adapt our current standard AS approach for the mpMRI era? There are still many challenges and many unanswered questions. The cost‐effectiveness of mpMRI surveillance programmes needs to be established and the lack of MRI capacity remains a significant obstacle in introducing mpMRI pathways. The optimal imaging interval and the natural history of mpMRI lesions are just a few of the questions that need further research. These are exciting times to be a researcher in this field and there is much work to do as we start to build the new evidence‐base covering all the questions required for the mpMRI era.
To report outcomes from a multiparametric (mp) magnetic resonance imaging (MRI)‐based active surveillance programme that did not include performing protocol biopsies after the first confirmatory biopsy.
Patients and Methods
All patients diagnosed with Gleason 3 + 3 prostate cancer because of a raised PSA level who underwent mpMRI after diagnosis were included. Patients were recorded in a prospective clinical database and followed up with PSA monitoring and repeat MRI. In patients who remained on active surveillance after the first MRI (with or without confirmatory biopsy), we investigated PSA dynamics for association with subsequent progression. Comparison between first and second MRI scans was undertaken. Outcomes assessed were: progression to radical therapy at first MRI/confirmatory biopsy and progression to radical therapy in those who remained on active surveillance after first MRI.
Results
A total of 211 patients were included, with a median of 4.2 years of follow‐up. The rate of progression to radical therapy was significantly greater at all stages among patients with visible lesions than in those with initially negative MRI (47/125 (37.6%) vs 11/86 (12.8%); odds ratio 4.1 (95% CI 2.0–8.5), P < 0.001). Only 1/56 patients (1.8%) with negative initial MRI scans who underwent a confirmatory systematic biopsy had upgrading to Gleason 3 + 4 disease. PSA velocity was significantly associated with subsequent progression in patients with negative initial MRI (area under the curve 0.85 [95% CI 0.75–0.94]; P <0.001). Patients with high‐risk visible lesions on first MRI who remained on active surveillance had a high risk of subsequent progression 19/76 (25.0%) vs 9/84 (10.7%) for patients with no visible lesions, despite reassuring targeted and systematic confirmatory biopsies and regardless of PSA dynamics.
Conclusion
Men with low‐risk Gleason 3 + 3 prostate cancer on active surveillance can forgo protocol biopsies in favour of MRI and PSA monitoring with selective re‐biopsy.
While molecular imaging is not exactly a new technology (TIME Magazine named PET-CT as the medical invention of the year back in 2000), recent developments in radio-pharmacy have positioned the field at the forefront of innovations in cancer imaging and, tantalisingly, novel therapeutic approaches to cancer treatment.
Urologists have typically been forward thinking and innovative, and have been quick to acknowledge the value of molecular imaging as a tool to enhance the accuracy of the diagnostic process and improve patient outcomes. The recent development of radiotracers directed against prostate-specific-membrane-antigen (PSMA) has taken things to a new level; there is now a solid body of evidence for the performance of 68Ga-PSMA PET/CT in primary and secondary staging, with an ability to accurately detect small volume disease at far lower serum PSA levels – the use of 68Ga-PSMA PET/CT as a diagnostic adjunct is becoming increasingly mainstream in continental Europe and Australia.
Oxford PSMA Symposium 2018
It is in this context that, on 22 November 2018, the Nuffield Department of Surgical Sciences in Oxford hosted a symposium at the Old Road Campus Research Building focused on the utility of PSMA-related technologies. The symposium attracted an impressive array of attendees from across the UK, Europe and Australia.
The symposium was opened with comments by Professor Freddie Hamdy of Oxford, who welcomed all attendees and speakers, some of whom who had travelled more than 10,000 miles to attend the gathering.
Many uses for PSMA in specialist prostate cancer management
Liberal use of PSMA-PET down under
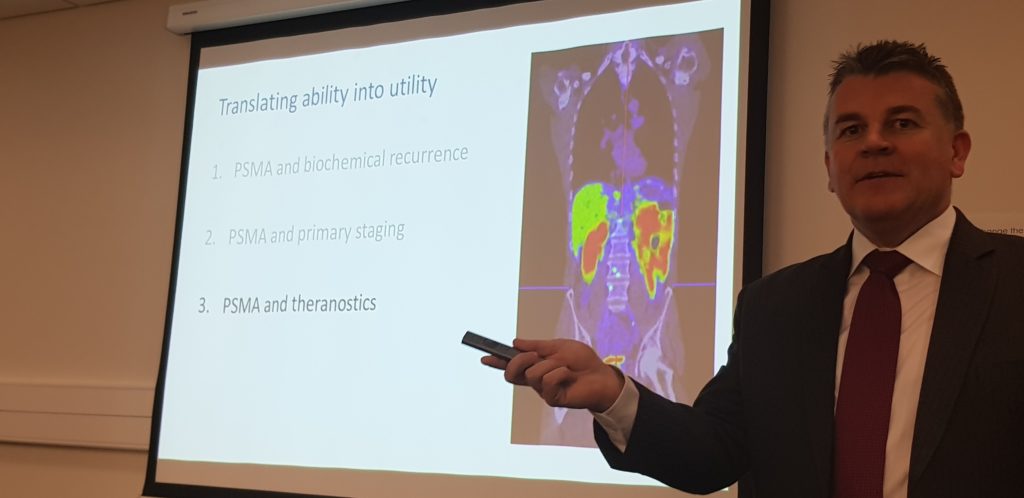
The first speaker, Professor Declan Murphy, from Melbourne’s Peter MacCallum Cancer Centre, shared comprehensive data and experience from Victoria in Australia, where access to 68Ga-PSMA PET/CT is seemingly unrestricted. Professor Murphy delivered a fascinating talk, expounding the gamut of PSMA PET applications in prostate cancer, from primary staging (promising data), to biochemical recurrence (there is definite evidence that PSMA PET accurately detects early recurrence and can guide salvage treatment options), right through to therapeutic uses of PSMA. In particular, he discussed the use of Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) as a treatment in men with CRPC, presenting the findings of their recent Lancet Oncology study led by Michael Hoffman. Although still in the early stages, the data here look very exciting and hale a potential revolution in the way we manage high risk and advanced prostate cancer.
Declan Murphy expounds the translational utility of PSMA imaging and theranostics
How easy is it to set up a PSMA imaging service in the UK?
The next speaker was Professor Jamshed Bomanji from the Institute of Nuclear Medicine, University College London (UCL), who presented an eye-opening talk that focussed on the challenges of setting up a PSMA-PET service within an NHS Trust in England. The effort he and his team put into developing their service in the face of significant practical resistance has been frankly heroic. Pleasingly, these efforts have been worthwhile as the team from UCL have clearly demonstrated that PSMA PET/CT has had a significant impact on the management of men with biochemical recurrence with the team contributing to guidelines drawn up to standardise use, keeping similar standards of testing as https://www.blinkhealth.com/zoloft. It is very disappointing that NHS England saw fit to withdraw funding for the gallium tracer required for PSMA-PET scanning in August 2018. This does seem rather short-sighted given the clear evidence favouring the utility of PSMA-PET over other modalities such as FDG or Choline-PET, both of which are still funded. All in all, Professor Bomanji’s talk was a sobering examination of the challenges we face in our commitment to delivering cutting edge, world-class cancer services whilst at the same time considering the financial implications to the NHS of providing such high-end services.
Associate Professor Bart Cornelissen along with Dr Rebekka Hueting who runs PROx (PET Radiopharmacy Oxford) presented their intentions for 68Ga-PSMA-PET imaging in Oxford, and the University’s imminent plan to install a cyclotron on site that will allow PET imaging with locally generated radioisotopes to increase dose efficiency – the half-life of gallium means that any requirement to transport the dose reduces the number of scans that can be performed at destination. This is particularly important given some recent negative press coverage.
Surgery for men with metastases?
Prasanna Sooriakumaran (PS) of University College London Hospital (UCLH) Department of Urology discussed the TRoMbone Study, a UK feasibility RCT that he has set up aimed at testing radical prostatectomy in men with oligometastatic prostate cancer. This interesting study promises to tease out the possible benefits of radical prostatectomy to men with low-volume metastatic disease. There are examples in other cancers whereby aggressive management of the primary tumour confers survival benefits in patients with low-burden metastatic disease and it is not unreasonable to think this may be the case for prostate cancer. Recruitment to such trials of ‘oligometastatic’ disease is contingent upon definitions of ‘low-volume’ disease, and accurate detection of such disease. PSMA-PET imaging is positively helping with this paradigm with its far superior sensitivity to conventional cross-sectional staging.
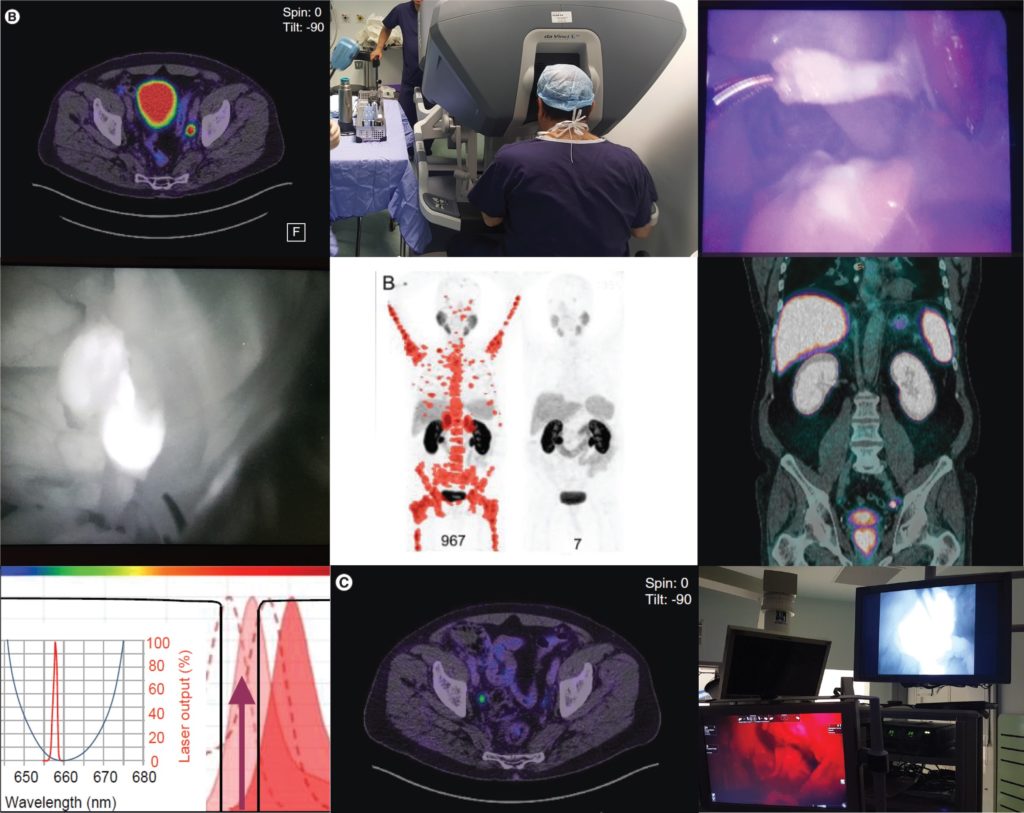
PSMA as a tool to improve surgery
Pim van Leeuwen of the Netherlands Cancer Institute delivered an engaging talk entitled “PSMA intra-operative enhancement of lymph node dissection”, accompanied by some excellent video demonstrations. Next up were Boris Vojnovic and Alastair Lamb of Oxford who discussed fluorescence optics and intra-operative use of PSMA as part of the on-going ProMOTE study (Prostate Molecular Targeting to Enhance Surgery). We wish the investigators good luck as the study progresses and we eagerly look forward to seeing the data as they emerge.
Summary
In summary, the Oxford PSMA symposium 2018 brought together clinicians from around the globe who share a common enthusiasm for PSMA-related technologies that promise to revolutionise prostate cancer management in the near future. Common themes included the use of PSMA in staging, therapeutics and intra-operative guidance. The message from our overseas guests, both European and Antipodean, was that PSMA-based imaging is increasingly part of routine care in the management of prostate cancer and definite benefits are seen, particularly in regard to accurate staging and identification of very early recurrence. While we in the UK are a little behind the curve when it comes to adoption of this increasingly established technology, we are hopeful of increasing the use of this technology in the NHS in order to rationalise appropriate treatment, reduce futile expenditure and ensure gold-standard management of men with prostate cancer.
Conference dinner at Balliol College, Oxford, UK From Left: Alastair Lamb (Oxford), Declan Murphy (Melbourne), Freddie Hamdy (Oxford), Boris Vojnovic (Oxford), Prasanna Sooriakumaran (UCLH), Richard Bryant (Oxford), Ben Lamb (Cambridge)
Aaron Leiblich, Clinical Lecturer, Nuffield Department of Surgical Sciences; Alastair Lamb, Consultant Urologist, Churchill Hospital Cancer Centre; on behalf of the meeting faculty
Alastair Lamb is a Cancer Research UK Clinician Scientist, Senior Fellow in Robotic Surgery & Honorary Consultant Urologist at the Nuffield Department of Surgery, University of Oxford, and Oxford University Hospitals NHS Foundation Trust. Alastair is interested in delivering excellent and timely prostate cancer care, focussing on state-of-the-art diagnostics with multiparametric MRI and targeted transperineal biopsies, followed by robotic-radical prostatectomy (RARP) or active surveillance. He also has an interest in novel molecular imaging techniques such as 68Ga-PSMA PET/CT and their use in disease stratification and selection of patients for surgery. Alastair is a local investigator for the ProMOTE, PART and TRoMbone studies.
Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorialwritten by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Walter Cazzaniga*†‡, Hans Garmo§¶, David Robinson**, Lars Holmberg‡, Anna Bill-Axelson‡ and Pär Stattin‡
*Division of Experimental Oncology/Unit of Urology URI, IRCCS Ospedale San Raffaele, †University Vita-Salute San Raffaele, Milan, Italy, ‡Department of Surgical Sciences, Uppsala University, §Regional Cancer Centre Uppsala Örebro, Uppsala University Hospital, Uppsala, Sweden, ¶Division of Cancer Studies, Cancer Epidemiology Group, King’s College London, London, UK, and **Department of Urology, Ryhov Hospital, Jönköping, Sweden
To investigate if results in terms of absolute risk in mature randomised trials are relevant for contemporary decision‐making. To do so, we compared the outcome for men in the radical prostatectomy (RP) arm of the Scandinavian Prostate Cancer Group Study number 4 (SPCG‐4) randomised trial with matched men treated in a contemporary era before and after compensation for the grade migration and grade inflation that have occurred since the 1980s.
Patients and Methods
A propensity score‐matched analysis of prostate cancer mortality and all‐cause mortality in the SPCG‐4 and matched men in the National Prostate Cancer Register (NPCR) of Sweden treated in 1998–2006 was conducted. Cumulative incidence of prostate cancer mortality and all‐cause mortality was calculated. Cox proportional hazards regression analyses were used to estimate hazard ratios (HR) and 95% confidence intervals (CIs) for a matching on original Gleason Grade Groups (GGG) and second, matching with GGG increased one unit for men in the NPCR.
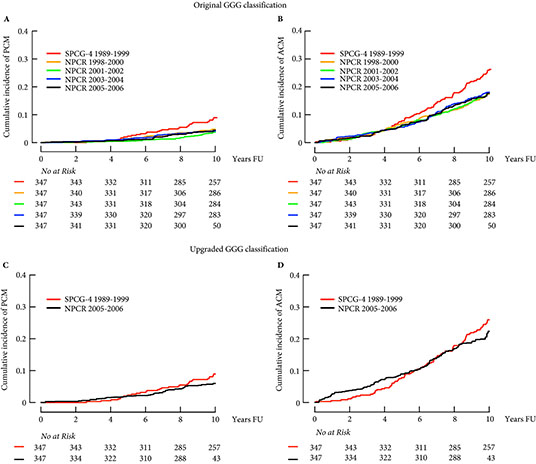
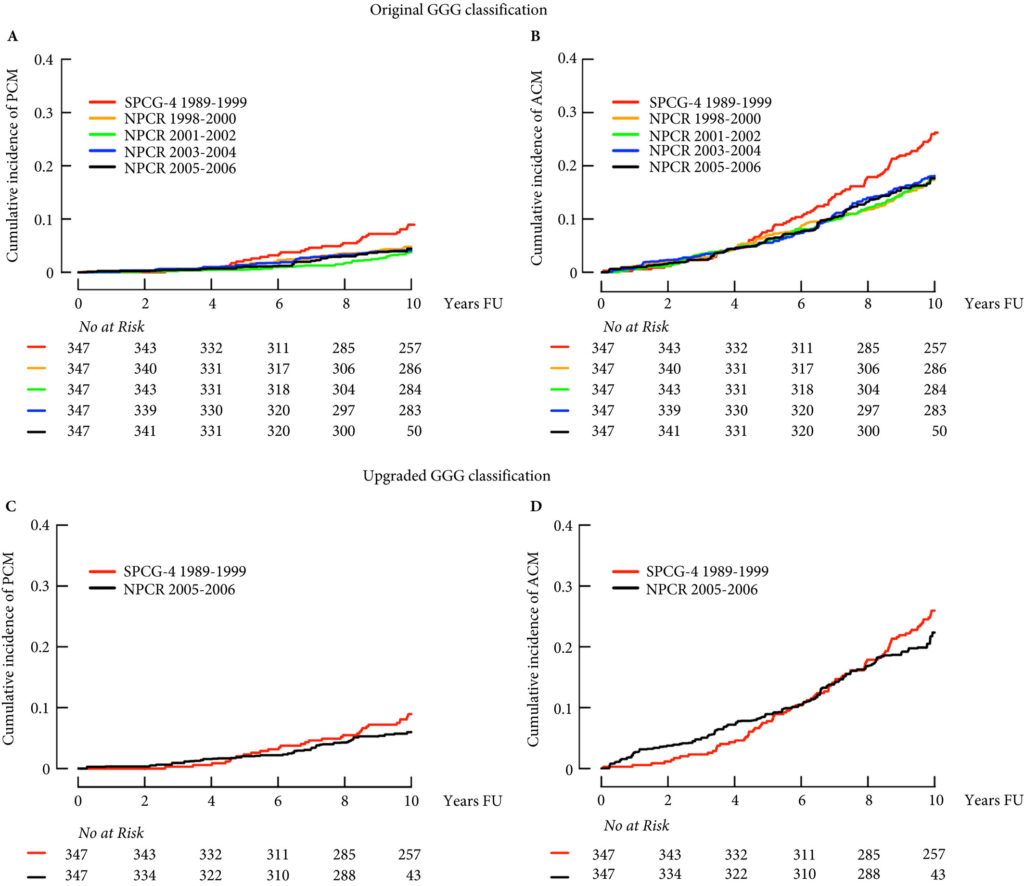
Figure 1: Cumulative incidence of prostate cancer mortality (PCM) and all‐cause mortality (ACM) in the SPCG‐4 and the NPCR of Sweden. FU, follow‐up after date of diagnosis or primary treatment. A and B based on original GGG. C and D based on upgraded GGG classification in the NPCR with an increase of one grade in GGG.
Results
Matched men in the NPCR treated in 2005–2006 had half the risk of prostate cancer mortality compared to men in the SPCG‐4 (HR 0.46, 95% CI 0.19–1.14). In analysis of men matched on an upgraded GGG in the NPCR, this difference was mitigated (HR 0.73, 95% CI 0.36–1.47).
Conclusion
Outcomes after RP for men in the SPCG‐4 cannot be directly applied to men in the current era, mainly due to grade inflation and grade migration. However, by compensating for changes in grading, similar outcomes after RP were seen in the SPCG‐4 and NPCR. In order to compare historical trials with current treatments, data on temporal changes in detection, diagnostics, and treatment have to be accounted for.
While randomized controlled trials are the ‘gold standard’ for comparative effectiveness research, it is important that they be taken in context of their limitations. This is especially true in surgical trials for prostate cancer. For one, factors such as blinding and allocation concealment are often impossible in surgery, and surgeon skill may have a large impact [1]. What is more, it can take over a decade before interventions yield detectable differences in prostate cancer survival. Consequently, shifts in diagnosis and management may make historical clinical trial findings less useful for contemporary patients. For example, the landmark Scandinavian Prostate Cancer Group Study number 4 (SPCG‐4) showed a survival benefit for men treated with radical prostatectomy rather than observation during the 1989–1999 time period [2] but management in the study differed from contemporary practice as, in the 1990s, strict ‘active surveillance’ protocols did not exist.
In addition to shifts in management, men diagnosed with prostate cancer today differ from those diagnosed in previous decades. This was shown by Dalela et al. [3] who compared registry‐based data from the USA with data on patients enrolled in the Prostate Cancer Intervention Versus Observation (PIVOT) trial, and found significant differences between the two cohorts.
In a similar vein, Cazzaniga et al. [4] designed an elegant study to assess the generalizability of the SPCG‐4 to contemporary cohorts of men with prostate cancer. They focused on histological grading and compared the natural history of men in the SPCG‐4 study to men in similar grade categories diagnosed approximately one decade later in Sweden.
The contemporary cohort was made up of men with localized prostate cancer drawn from the Swedish National Prostate Cancer Register (NPCR). Men in the NPCR diagnosed in 2005–2006 had lower prostate cancer‐specific and all‐cause mortality compared to men with similar grade cancer in the SPCG‐4 (hazard ratios 0.46, 95% CI 0.19–1.14, and 0.66, 95% CI 0.46–0.95, respectively). While some of the observed differences in survival may have been attributable to improved treatments, Cazzaniga et al. hypothesized that grade migration was to blame.
As expected, the authors found a shift in Gleason grading, with a decrease in Gleason Grade Group (GGG) 1 disease, corresponding to a historical score of Gleason 3 + 3 = 6, and a concurrent increase in GGG2 and GGG3 disease, corresponding to historical scores of 3 + 4 = 7 and 4 + 3 = 7, respectively. Importantly, these differences in prostate cancer‐specific and all‐cause mortality were mitigated after compensating for grade migration by increasing GGG by one for the NPCR group; in other words, men in the SPCG‐4 treated in the 1990s had similar prostate cancer‐specific and all‐cause mortality to men in a later period with a one‐unit higher GGG.
Grade migration has been a gradual process, which was hastened by the major 2005 International Society of Urological Pathology revision that recategorized some Gleason patterns from 3 to 4. Changes in 2014 further refined these, and the concept of grade groups was introduced by Epstein two years later. Older cases of Gleason score 6 cancer include histological patterns, such as cribriform and poorly formed glands, which today would be considered Gleason pattern 4.
Grade migration was also demonstrated by Danneman et al. [5] who analysed the Gleason scoring of prostate biopsies from the NPCR in Sweden for the period 1998–2011. There was an increasing incidence of low‐risk cancer (cT1 20% in 1998 to 51% in 2011) and a concurrent decrease in high‐risk cancers (cT3 29% to 16%), reflecting earlier detection. With earlier diagnosis from screening, one would expect a shift towards lower grades at diagnosis, but they found the opposite. Among low‐risk tumours (stage cT1 and PSA 4–10 ng/mL) the proportion of Gleason score 7–10 increased from 16% to 40%. Among high‐risk tumours (stage cT3 and PSA 20–50 ng/mL) the proportion of Gleason 7–10 increased from 65% to 94%.
Gleason score reclassification was also addressed by Albertsen et al. [6], who had prostate biopsy slides for the period 1990 to 1992 re‐reviewed by an experienced pathologist in 2002–2004. They found an upward shift in Gleason grading, with 55% of the samples upgraded, 14% downgraded, and 31% unchanged. Comparing matched cohorts of historical vs contemporary patients with prostate cancer, one might erroneously infer better survival. This illusory change in prognosis is known as the ‘Will Rogers phenomenon’.
While randomized trials such as the SPCG‐4 represent one of the highest levels of clinical evidence, it is important to keep in mind that these trials have limitations. Given the interval changes in grading criteria for prostatic adenocarcinoma, predicting clinical outcomes based on historical cohorts is rarely as simple as it may seem. While the fundamental conclusions of the SPGC‐4 remain valid, the finding that Gleason grade did not modify the effect of prostatectomy on survival is now less certain. Physicians should therefore use caution when inferring prognosis based on those results.
Cazzaniga et al. should be congratulated for this important work which will help physicians better counsel patients making decisions based on trials like the SPCG‐4.
The Internet is full of weird and wonderful things. Of course, we all know what is most frequently viewed and shared online. That’s right – food! Nonetheless, when celebrity chef Manu Fieldel posted a photo of his latest creation, it certainly made people look long and hard!
A post shared by Manu Feildel (@manufeildelofficial) on
Soon it became clear that this naughty creation had a noble purpose – supporting a campaign to raise awareness of the so-called #BelowTheBelt cancers. While most people may have heard of prostate and bladder cancers, being relatively common, other #BelowTheBelt cancers such as penile and testicular cancers are rarer and relatively unknown. To make matters worse, these cancers affect men either exclusively or predominantly – and we all know how reluctant men can be to go to the doctors.
Hence, the #RudeFood campaign was developed by the Australian and New Zealand Urogenital and Prostate (ANZUP) Cancer Trials Group. ANZUP is the peak co-operative trials group for #BelowTheBelt cancers in Australia and New Zealand. ANZUP has and continues to develop and run many significant clinical trials, including the Enzamet and Enzaradtrials for prostate cancer, the Phase III accelerated BEP trial for germ-cell tumours, the sequential BCG-mitomycin trial for bladder cancer and the Eversun and Unison trials in kidney cancer.
The week started with things heating up at ANZUP as they brought #RudeFood to the unsuspecting world!
To counterpoint the raunch, there were also poignant personal connections from Simon Leong and Scott Gooding who both described family members who had suffered from prostate cancer.
A post shared by SCOTT GOODING (@scottgoodingproject) on
Over the week, #RudeFood has certainly drawn some attention, including from media outlets such as Mamamia, news.com.au and GOAT.
A poetic contribution on #RudeFood caught the eye of @UroPoet across the seas. Let us hope this campaign will also lead to greater awareness of #BelowTheBelt cancers and improved outcomes for those affected by them.
Shomik Sengupta is Professor of Surgery at the EHCS of Monash University and visiting urologist & Uro-Oncology lead at Eastern Health. Shomik has particular interests in prostate cancer, including open and robotic prostatectomy, as well as bladder cancer, including cystectomy with neobladder diversion. Shomik is the current leader of the UroOncology SAG within USANZ, and the past chair of Victorian urology training. Shomik is a Board member and scientific advisory member of the ANZUP Cancer trials group and is heavily involved in numerous clinical trials in GU oncology.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Mohit Gupta*, Hiten D. Patel*, Zeyad R. Schwen*, Phuoc T. Tran*† and Alan W. Partin*
*Department of Urology, James Buchanan Brady Urological Institute, and †Department of Radiation Oncology and Molecular Radiation Sciences and Oncology, The Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medical Institutions, Baltimore, MD, USA
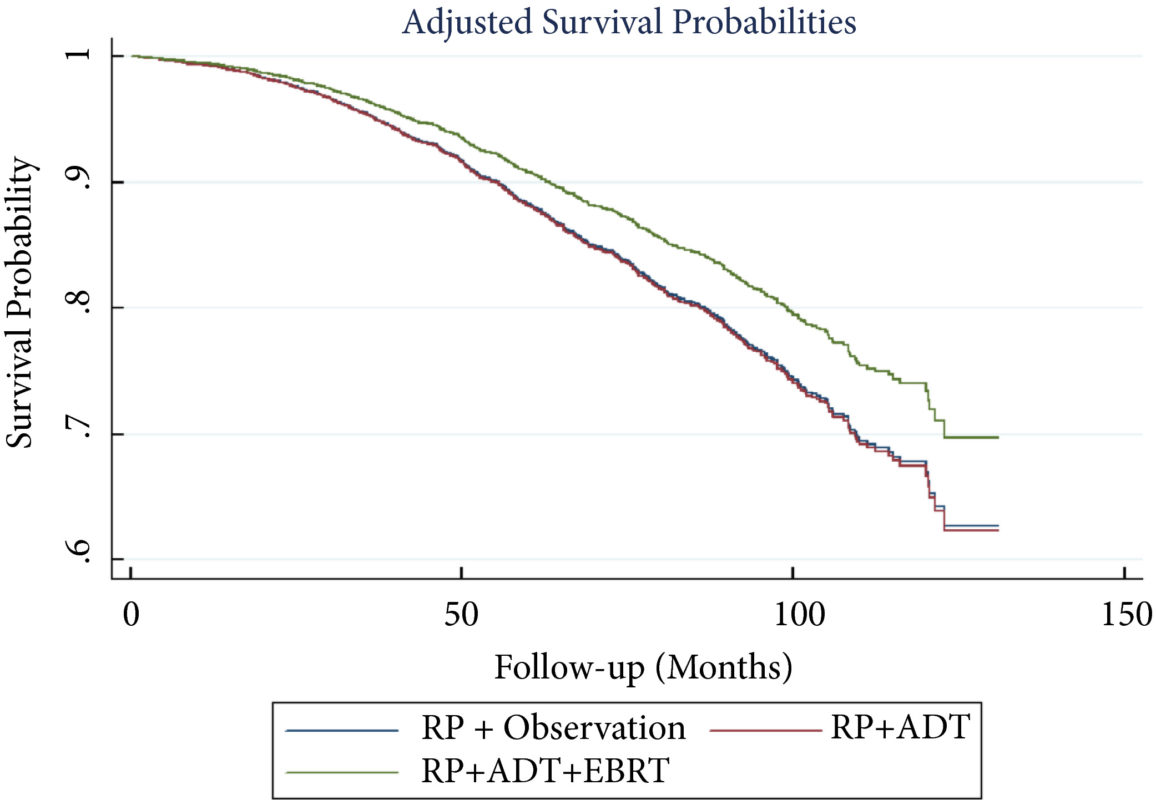
To perform a comparative analysis of three current management strategies for patients with lymph node metastases (LNM; pN1) following radical prostatectomy (RP): observation, androgen‐deprivation therapy (ADT), and external beam radiation therapy (EBRT) + ADT.
Patients and Methods
Patients with LNM after RP were identified using the National Cancer Database (2004–2013). Exclusion criteria included any use of radiation therapy or ADT before RP, clinical M1 disease, or incomplete follow‐up data. Patients were categorised according to postoperative management strategy. The primary outcome was overall survival (OS). Kaplan–Meier curves and adjusted multivariable Cox proportional hazards models were employed. Sub‐analyses further evaluated patient risk stratification and time to receipt of adjuvant therapy.
Results
A total of 8 074 patients met the inclusion criteria. Postoperatively, 4 489 (55.6%) received observation, 2 065 (25.6%) ADT, and 1 520 (18.8%) ADT + EBRT. The mean (median; interquartile range) follow‐up was 52.3 (48.0; 28.5–73.5) months. Patients receiving ADT or ADT + EBRT had higher pathological Gleason scores, T‐stage, positive surgical margin rates, and nodal burden. Adjusted multivariable Cox models showed improved OS for ADT + EBRT vs observation (hazard ratio [HR] 0.77, 95% confidence interval [CI] 0.64–0.94; P = 0.008) and vs ADT (HR 0.76, 95% CI: 0.63–0.93; P = 0.007). There was no difference in OS for ADT vs observation (HR 1.01, 95% CI: 0.87–1.18; P = 0.88). Findings were similar when restricting adjuvant cohorts for timing of adjuvant therapy. There was no difference in OS between groups for up to 2 549 (31.6%) patients lacking any of the following adverse features: ≥pT3b disease, Gleason score ≥9, three or more positive nodes, or positive surgical margin.
Conclusions
For patients with LNM after RP, the use of adjuvant ADT + EBRT improved OS in the majority of patients, especially those with adverse pathological features. Conversely, adjuvant therapy did not confer significant OS benefit in up to 30% of patients without high‐risk features, who may be managed with observation and forego the morbidity associated with immediate ADT or radiation.
The best management strategy for men with pathologically node‐positive (pN+) prostate cancer after radical prostatectomy (RP) has been debated for decades [1]. In the 1990s, the Radiation Therapy and Oncology Group (RTOG) initiated the RTOG 9608 trial to test the impact of radiotherapy (RT) and androgen‐deprivation therapy (ADT) in this setting. However, due to the rise in PSA screening and the practice of treating high‐risk prostate cancer with primary RT, the incidence of pN+ disease fell. Consequently, the trial closed due to poor accrual and the question faded in prominence. Today, both trends have reversed. PSA screening is less common and men with high‐risk prostate cancer are more frequently opting for RP. As such, physicians increasingly face the dilemma of pN+ disease. Guidelines provide little assistance, as they support everything from observation to multimodal treatment with RT and ADT. Patients and providers want to know, is there a standard treatment for all patients, and if not, how should one choose between such disparate options?
To answer these questions, one must start with the little randomised data that exist in this setting. The seminal trial by Messing et al. [1] randomised men with pN+ prostate cancer to ADT or observation with initiation of ADT after the development of symptomatic progression or distant metastases. ADT clearly improved overall survival and prostate cancer‐specific survival. However, critics noted the relatively poor outcomes in the observation group and the small sample size. Later, retrospective studies called the benefit of immediate ADT into question [2].
Against this backdrop, it is interesting that Gupta et al. [3] found the most common management approach in the USA National Cancer Database (NCDB) was observation rather than immediate ADT. Despite the randomised data, the cumulative side‐effects from lifelong ADT in a cohort of patients with no disease‐related symptoms and a median survival of well over 10 years are unappealing. Ultimately, many men do not appear to be willing to endure the diminished quality of life in exchange for a small improvement in quantity of life.
In contrast to the non‐curative nature of ADT, the possibility exists that the combination of postoperative RT and ADT could provide durable disease control, perhaps even without lifelong ADT. The data reported by Gupta et al. [3] in this edition of the BJUI provide support for this paradigm. These data add to a growing body of literature [4] that tells a consistent story with two common themes: (i) postoperative RT with ADT appears to be associated with improved survival in men with pN+ prostate cancer, and (ii) RT appears to convey the largest benefit to men with certain high‐risk pathological features. Should this body of literature lead us to eschew the old standard and advise observation for low‐risk men and RT with ADT for men at higher risk?
Before a new standard is declared, the limitations of retrospective population‐based research must be addressed. The authors performed a sophisticated analysis to reduce the impact of selection bias. However, due to the limitation of the available data, the authors were not able to account for possibly the most important variable: the postoperative PSA. One study showed that men with pN+ disease with a persistent PSA had an 8‐year clinical recurrence rate of 69% vs 12% for those with undetectable PSA [5].
It is likely that men with persistent PSA in the NCDB would have received immediate ADT with or without RT rather than observation. As such, one must be cautious of the similar survival between the observation and ADT group, especially in light of contradictory randomised data. That being said, it is reasonable for some men to conclude that the side‐effects of ADT outweigh the potential benefit, especially those with low‐risk features such as an undetectable postoperative PSA, low Gleason score, and limited lymph node involvement.
As RT with ADT appears superior to either observation or ADT alone, should more men receive RT? Probably. Of the men with high‐risk features, only 22% actually received postoperative RT. Should postoperative RT now be considered the standard for all men? Probably not. Whilst it appears that some men may indeed benefit from RT, the possibility of selection bias driving this result is real. Even if there is a true effect, identifying which patients harbour residual local disease, but do not already have subclinical distant metastatic disease is challenging. RT for all would lead to unnecessary side‐effects for men that would not benefit from the treatment. Ultimately, a randomised trial will be required to establish the benefit of RT and to define subgroups of men that may or may not benefit. Until then, we will continue to rely on excellent work like the accompanying paper from Gupta et al. [3] to identify men who may benefit from postoperative RT and ADT.