Article of the week: Using MRI to select and monitor active surveillance CaP patients
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Multiparametric magnetic resonance imaging findings in men with low-risk prostate cancer followed using active surveillance
Jeffrey K. Mullins*, David Bonekamp†, Patricia Landis*, Hosne Begum†, Alan W. Partin*, Jonathan I. Epstein*‡, H. Ballentine Carter* and Katarzyna J. Macura*†
*James Buchanan Brady Urological Institute, †Russell H. Morgan Department of Radiology, and ‡Department of Pathology, Johns Hopkins Medical Institutions, Baltimore, MD, USA
OBJECTIVE
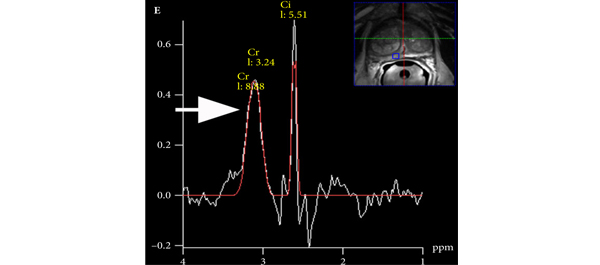
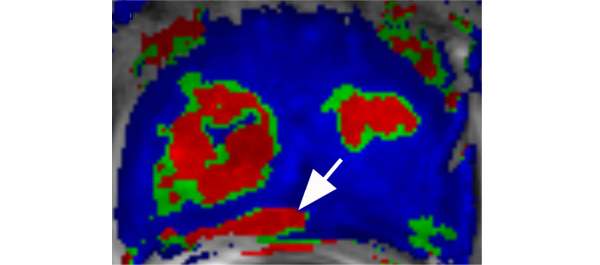
• To assess the performance of multiparametric magnetic resonance imaging (MRI) in identifying pathological-index (path-index) lesions, defined as cancer present in the same prostate sextant in two separate surveillance biopsies, in men followed within an active surveillance (AS) programme for low-risk prostate cancer (CaP) with extended follow-up.
MATERIALS AND METHODS
• A total of 50 men, representing >215 person-years of follow-up in an AS programme, who were referred for prostate MRI were randomly chosen to have their images reviewed by a radiologist with expertise in prostate MRI, who was blinded to biopsy results.
• Index lesions on MRI were defined as a single suspicious lesion ≥10 mm or >2 lesions in a given prostate sextant. Lesions on MRI were considered suspicious if ≥2 abnormal parameters co-registered anatomically. Path-index lesions were defined as cancer present in a given prostate sextant on two separate biopsy sessions.
• Sensitivity and specificity were calculated to test the performance of MRI for identifying path-index lesions.
• Clinical and pathological features were compared between men with and without a MRI-index lesion.
RESULTS
• A total of 31 path-index and 13 MRI-index lesions were detected in 22 and 10 patients, respectively.
• Multiparametric MRI demonstrated excellent specificity and negative predictive value (0.974 and 0.897, respectively) for the detection of path-index lesions. Sensitivity (0.19) and positive predictive value (0.46) were considerably lower.
• Patients with an index lesion on MRI were younger and less likely to have met the ‘Epstein’ criteria for very low-risk CaP.
• Compared with men without an MRI lesion, a significant increase in biopsy reclassification was noted for men with a MRI lesion (40 vs 12.5%, P = 0.04).
CONCLUSIONS
• A non-suspicious MRI was highly correlated with a lack of path-index lesions in an AS population.
• Multiparametric MRI may be useful in both the selection and monitoring of patients undergoing AS.
Read Previous Articles of the Week