Article of the week: Fit to a T-cell: measuring host immunity in renal cell carcinoma
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video of Dr. Scala discussing her article.
If you only have time to read one article this week, it should be this one.
Regulatory T cells, interleukin (IL)-6, IL-8, Vascular endothelial growth factor (VEGF), CXCL10, CXCL11, epidermal growth factor (EGF) and hepatocyte growth factor (HGF) as surrogate markers of host immunity in patients with renal cell carcinoma
Marianeve Polimeno, Maria Napolitano, Susan Costantini*, Luigi Portella, Arianna Esposito, Francesca Capone*, Eliana Guerriero*, AnnaMaria Trotta, Serena Zanotta, Luigi Pucci†, Nicola Longo†, Sisto Perdonà‡, Sandro Pignata‡, Giuseppe Castello* and Stefania Scala
Oncological Immunology, National Cancer Institute ‘G. Pascale’, *National Cancer Institute ‘G. Pascale’ Cancer Research Center, Mercogliano, Avellino, †Genitourinary Oncology and Rare Cancer Center, Federico II University, ‡Department of Urology, National Cancer Institute ‘G. Pascale’, Naples, Italy
M.P. and M.N. contributed equally to this work.
OBJECTIVE
• To identify a phenotype that could be informative and prognostic in patients with renal cell carcinoma (RCC) peripheral blood was evaluated for TH1, TH2, regulatory T cells (Tregs), natural killer (NK) and NKT cells and for cytokines/chemokines.
PATIENTS AND METHODS
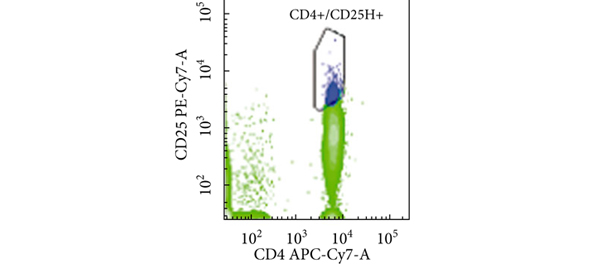
• Peripheral blood from 77 patients with RCC and 40 healthy controls was evaluated by flow cytometry using monoclonal antibodies against CD4, CD25, FoxP3, CD45RA, CD45RO, CD152, CD184, CD279, CD3, CD16, CD56, CD161, CD158a, CD4, CD26, CD30, CD183 and CD184.
• A concomitant evaluation of 38 molecules was conducted in patients’ serum using a multiplex biometric ELISA-based immunoassay.
RESULTS
• The number of NK cells CD3−/CD16+, CD3−/CD16+/CD161+ (NK) and CD3−/CD16+/CD161+/CD158a+ (NK- Kir 2+) was greater in the patients with RCC (P < 0.05); and the number of Treg cells CD4+/CD25high+/FOXP3+ and the subset CD4+/CD25high+/FOXP3+/CD45RA+ (naïve) and CD45R0+(memory) cells, were greater in the patients with RCC (P < 0.001).
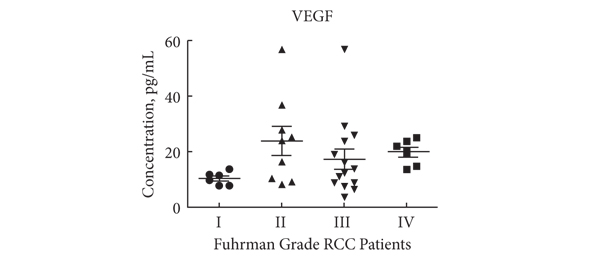
• An increase in the following was observed in the serum of patients with RCC compared with healthy controls: interleukin (IL)-4, IL-6, IL-8, IL-10, G-CSF, CXCL10, CXCL11, hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF). According to Ingenuity Pathway Analysis (IPA), CXCL10, IL-6, IL-8, epidermal growth factor (EGF), HGF and VEGF were associated with a network that controls cellular movement, tissue development and cellular growth.
• Kaplan–Meier analysis for disease-free survival showed that high numbers of CD4+/CD25high+/FOXP3+/CD45RA+ (Treg naïve) and low numbers of CD3−/CD16+/CD161+/CD158a+ (NK-Kir+) cells predict short disease-free survival in patients with RCC.
CONCLUSION
• Concomitant evaluation of Treg (CD4+/CD25high+/FOXP3+ and CD4+/CD25high+/FOXP3+/CD45RA+) and of six soluble factors (IL-6, IL-8 ,VEGF, CXCL10, CXCL11, EGF, HGF) might be a surrogate marker of host immunity in patients with RCC.
Read Previous Articles of the Week