
Article of the Week: More PLND template at RP detects metastases in the common iliac region and in the fossa of Marcille
Every Month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
More extended lymph node dissection template at radical prostatectomy detects metastases in the common iliac region and in the fossa of Marcille
Abstract
Objectives
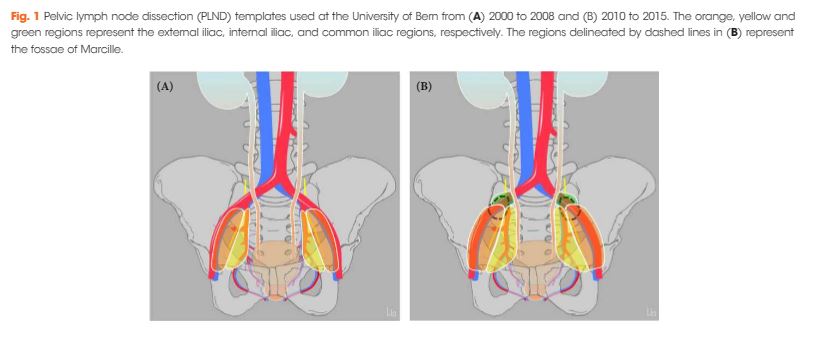
To assess the effect of adding lymph nodes (LNs) located along the common iliac vessels and in the fossa of Marcille to the extended pelvic LN dissection (PLND) template at radical prostatectomy (RP).
Patients and Methods
A total of 485 patients underwent RP and PLND at a referral centre between 2000 and 2008 (historical cohort: classic extended PLND template) and a total of 268 patients between 2010 and 2015 (contemporary cohort: extended PLND template including LNs located along the common iliac vessels and in the fossa of Marcille). Descriptive analyses were used to compare baseline, pathological, complication and functional data between the two cohorts. A logistic regression model was used to assess the template’s effect on the probability of detecting LN metastases.
Results
Of 80 patients in the historical cohort with pN+ disease, the sole location of metastasis was the external iliac/obturator fossa in 23 (29%), and the internal iliac in 18 (23%), while 39 patients (49%) had metastases in both locations. Of 72 patients in the contemporary cohort with pN+ disease, the sole location of metastasis was the external iliac/obturator fossa in 17 patients (24%), the internal iliac in 24 patients (33%), and the common iliac in one patient (1%), while 30 patients (42%) had metastases in >1 location (including fossa of Marcille in five patients). Among all 46 patients in the contemporary cohort with ≤2 metastases, three had one or both metastases in the common iliac region or the fossa of Marcille. The adjusted probability of detecting LN metastases was higher, but not significantly so, in the contemporary cohort. There were no differences between the two cohorts in complication rates and functional outcomes.
Conclusion
A more extended template detects LN metastases in the common iliac region and the fossa of Marcille and is not associated with a higher risk of complications; however, the overall probability of detecting LN metastases was not significantly higher.
