Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community and a video prepared by the authors; we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this month, we recommend this one.
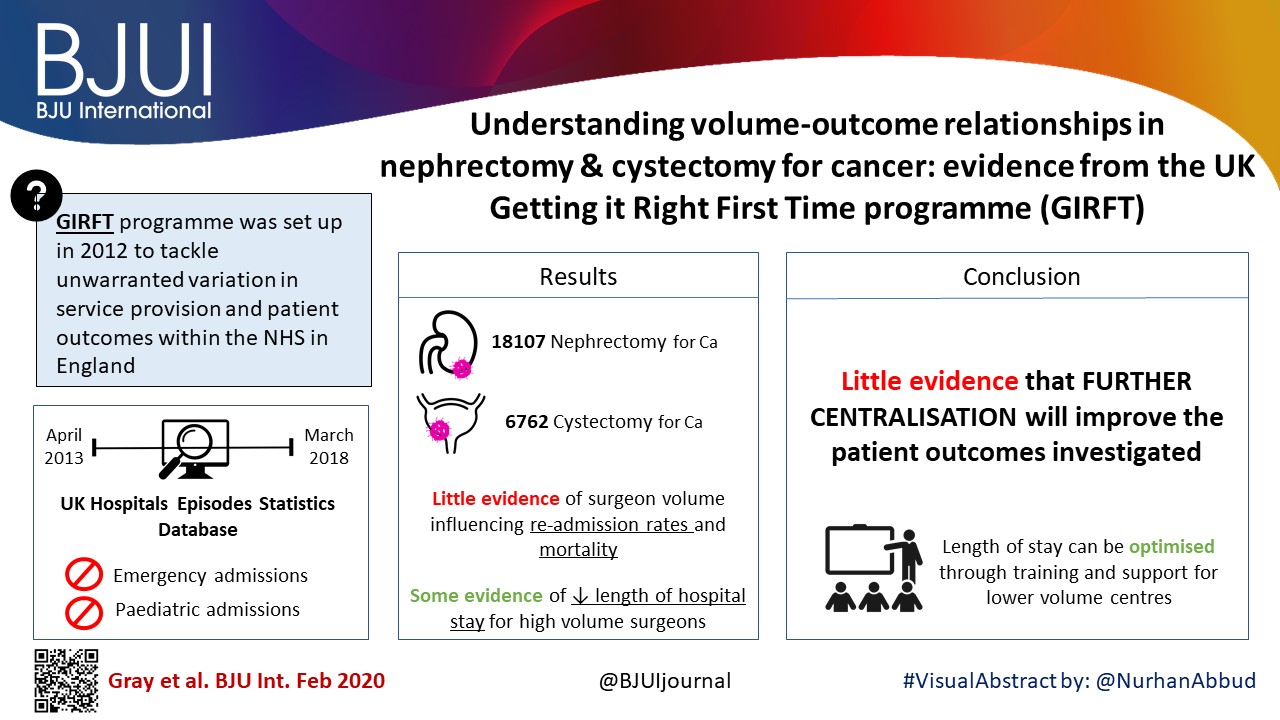
William K. Gray*, Jamie Day*, Tim W. R. Briggs* and Simon Harrison*†
*Getting it Right First Time Programme, NHS England and NHS Improvement, London, UK and †Pinderfields Hospital, Mid Yorkshire Hospitals NHS Trust, Wakefield, UK
To investigate volume–outcome relationships in nephrectomy and cystectomy for cancer.
Materials and Methods
Data were extracted from the UK Hospital Episodes Statistics database, which records data on all National Health Service (NHS) hospital admissions in England. Data were included for a 5‐year period (April 2013–March 2018 inclusive) and data on emergency and paediatric admissions were excluded. Data were extracted on the NHS trust and surgeon undertaking the procedure, the surgical technique used (open, laparoscopic or robot‐assisted) and length of hospital stay during the procedure. This dataset was supplemented by data on mortality from the UK Office for National Statistics. A number of volume thresholds and volume measures were investigated. Multilevel modelling was used to adjust for hierarchy and confounding factors.
Results
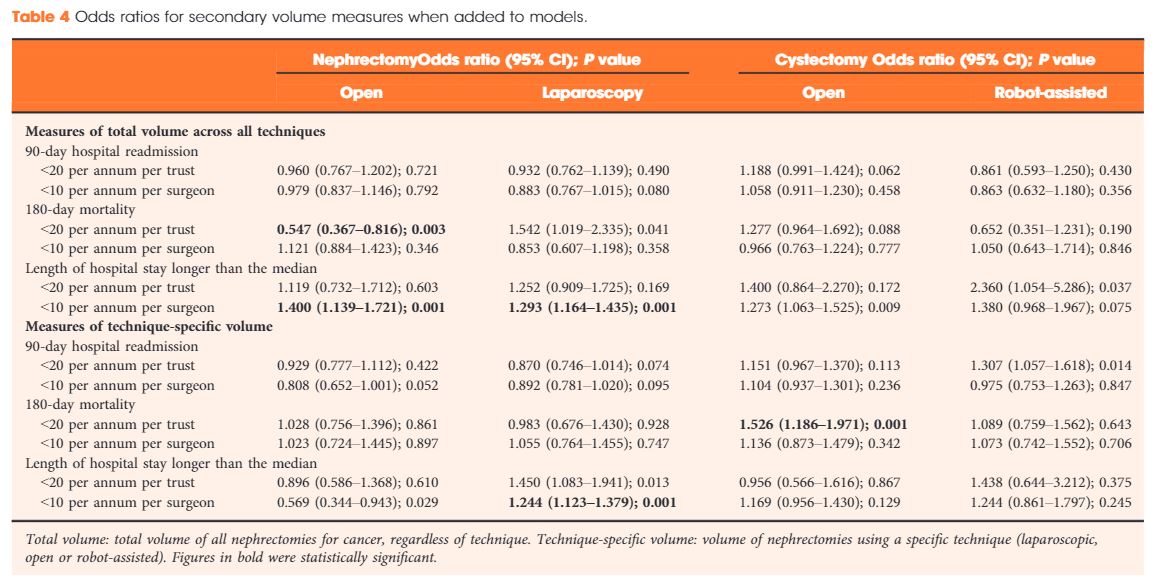
Data were available for 18 107 nephrectomy and 6762 cystectomy procedures for cancer. There was little evidence of trust or surgeon volume influencing readmission rates or mortality. There was some evidence of shorter length of hospital stay for high‐volume surgeons, although the volume measure and threshold used were important.
Conclusions
We found little evidence that further centralization of nephrectomy or cystectomy for cancer surgery will improve the patient outcomes investigated. It may be that length of stay can be optimized though training and support for lower‐volume centres, rather than further centralization.
To investigate volume–outcome relationships in nephrectomy and cystectomy for cancer.
Materials and Methods
Data were extracted from the UK Hospital Episodes Statistics database, which records data on all National Health Service (NHS) hospital admissions in the England. Data were included for a 5‐year period (April 2013–March 2018 inclusive) and data on emergency and paediatric admissions were excluded. Data were extracted on the NHS trust and surgeon undertaking the procedure, the surgical technique used (open, laparoscopic or robot‐assisted) and length of hospital stay during the procedure. This dataset was supplemented by data on mortality from the UK Office for National Statistics. A number of volume thresholds and volume measures were investigated. Multilevel modelling was used to adjust for hierarchy and confounding factors.
Results
Data were available for 18 107 nephrectomy and 6762 cystectomy procedures for cancer. There was little evidence of trust or surgeon volume influencing readmission rates or mortality. There was some evidence of shorter length of hospital stay for high‐volume surgeons, although the volume measure and threshold used were important.
Conclusions
We found little evidence that further centralization of nephrectomy or cystectomy for cancer surgery will improve the patient outcomes investigated. It may be that length of stay can be optimized though training and support for lower‐volume centres, rather than further centralization.
In this issue of BJUI Chiong et al [1] present the results of the Asia Pacific (APAC) Advanced Prostate Cancer Consensus Conference (APCCC) 2018, during which the implications of the APCCC 2017 findings were discussed in the context of the APAC region. For background, it is important to understand the concept of the original APCCC and why it was initiated [1,2,3].
The consensus conference aims to target areas of controversy in the clinical management of advanced prostate cancer where evidence is either limited or lacking or where interpretation of evidence is controversial. The expert consensus aims to complement existing clinical practice guidelines that are mostly based on high‐level evidence. The APCCC’s most prominent aim is knowledge translation, in the sense of improving care of men with advanced prostate cancer worldwide who are treated outside of centres of excellence. During the original APCCC in St Gallen, where 61 prostate cancer experts and scientists were assembled, the majority of the consensus questions were discussed; these had been prepared prior to the conference under the idealistic assumption that all diagnostic procedures and treatments (including expertise in their interpretation and application) mentioned were readily available. These assumptions have been specifically chosen, because availability of systemic treatment options for advanced prostate cancer, access to next‐generation imaging (whole‐body MRI and positron‐emission tomography [PET]) and expertise in molecular techniques and interpretation of results vary widely across the world. The original global APCCC did not generally address regional or country‐specific situations, but APCCC 2017 did have a special session and also voting questions for treatment options in countries with limited resources. Importantly, consensus recommendations may even inform and influence regulatory authorities, for example, if a specific treatment is considered to be the best option by the majority of experts and availability in a certain country is lacking.
The APAC APCCC 2018 consisted of 20 experts (mostly urologists) from 15 countries and discussed the findings and voting results of five of the 10 APCCC 2017 topics. Whether or not Turkey should be considered an APAC country is unclear. The most relevant observations were as set out below:
There is huge variation in access to drugs used for treatment of advanced prostate cancer in the APAC region. Australia and Hong Kong have access to almost all treatment options (notably cabazitaxel is not mentioned) compared with countries such as Vietnam or the Philippines, where there is limited availability of many compounds. Regarding imaging technologies (standard CT is not mentioned), there seems to be wide availability of next‐generation imaging such as whole‐body MRI and choline‐ or PSMA‐PET technologies; however, these imaging methods are often not reimbursed.
Pharmaco‐ethnic issues have so far not been considered by the original APCCC and the APAC report clearly highlights the need to address such issues. The higher toxicity of docetaxel in Asian men may influence treatment recommendations, especially in situations such as low‐volume metastatic castration‐naïve prostate cancer, where the role of early addition of docetaxel to androgen deprivation therapy is less clear.
The authors of the APAC meeting state that ketoconazole and bicalutamide are still widely used despite the proven superiority of enzalutamide vs bicalutamide. A possible reason for this is the lack of reimbursement in some APAC countries.
There is an obvious need for clinical trials in the APAC region because of variations in genetics, genomics, epidemiology and pharmaco‐ethnicity. Such trials may answer questions about toxicity/tolerability and also optimal use of resources in the context of economic limitations.
In summary, the APAC APCCC 2018 is an excellent example of how the global APCCC findings should be discussed and integrated on a regional or even country‐specific level. The authors are therefore to be congratulated for their efforts and for writing up the discussions. The next APCCC (2019; apccc.org) will take up a number of points raised by the APAC meeting, namely, more panel experts from APAC countries and pharmaco‐ethnic topics.
Olá! The 37th Congress of the Société d’Urologie (SIU) was held in Lisbon, a beautiful, historic city (19th-22nd October 2017). It is the first time the congress has been held here. We were told by the co-hosts during the opening ceremony that Portugal has a history of finding new routes and building bridges to other cultures, which they hoped to emulate at the Congress. The iconic 24 de Abril Bridge, the largest in Europe, was visible from the Congress Centre serving as a visual reminder of bridges being made during this congress.
The SIU is unique as it is a truly international association with no country or continent affiliation; it has 7000 members from 130 countries and 24 directors from every continent. Therefore the congress brings urologists from all over the world together. The words “Together, United, Stronger” said during the opening ceremony resonated as the ethos of the conference; and is especially pertinent in the current worldwide political climate. Furthermore, that the educational, global and philanthropic aspects of being part of such a society was highlighted as ways we can all help each other.
SIU 2017 had an engaging scientific programme providing a valuable educational experience to attendees over the four days. It covered the breadth of urology and we were honoured to listen to such notable speakers. The navigable congress centre (as well as the congress being a smaller meeting, as compared to EAU, AUA) meant delegates could easily attend whatever took their interest. The Scientific Programme included Plenary sessions, Master Classes, debates, ‘controversies’ sessions, instructional courses, poster presentations, the SIU Nurses’ Symposium and hosted urological organisation meetings. There were also Industry supported sessions and an Exhibition Hall.
The social programme allowed relaxation and networking amongst colleagues; plus sampling local Portuguese wines, food and an insight into Portuguese culture. The opening ceremony included a Fado performance. The SIU night held at Pátio da Galé in the PraÇa do Comércio was the pinnacle of the social aspect of the conference. The refreshments were plentiful and delicious, there were gelato stands as well as enough Pastel de Nata to feed a small army! A typical brass band, ceramic station, football net and DJ kept people entertained until we were told to leave. The SIU President’s Dinner held in the Queluz Palace was an amazing night in impressive surroundings for invited guests.
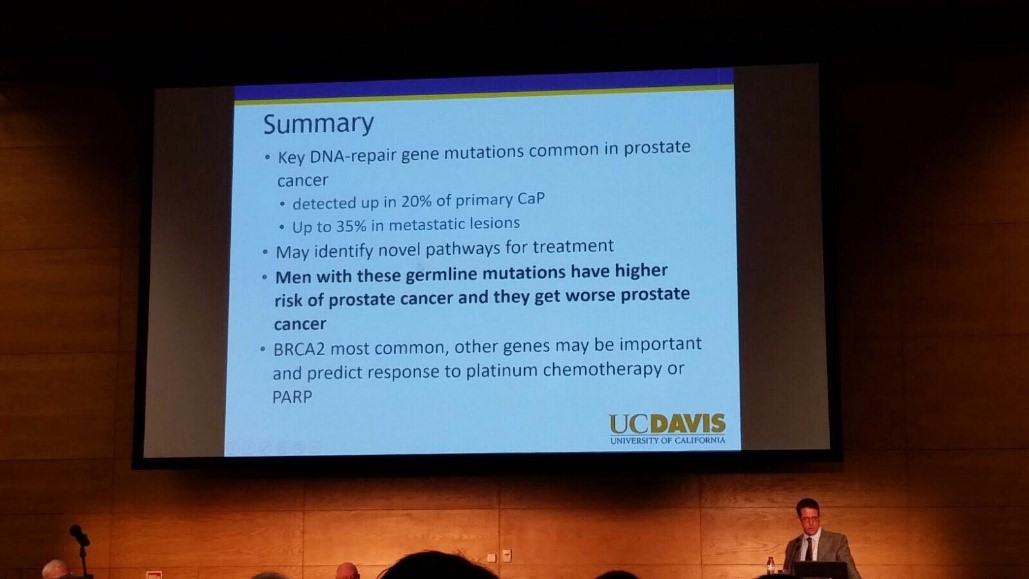
The fully attended WUOF session on the first day brought experts in the field of Urological cancers to provide their views on the changing paradigms and new treatments. All talks provided succinct, expert opinion. The presentation by Marc Dall’Era on the genetics of prostate cancer and link with the BRACA gene was particularly informative; especially as these men get worse cancer: pictured. Genetic counselling of patients diagnosed with prostate cancer may need to increase in the future. Genomics was discussed in other cancer sessions too; it’s growing availability, reducing costs and correlation with difference in outcomes between patients must surely strengthen the argument for more personalised medicine.
I also particularly enjoyed the presentation by Tony Finelli who unraveled the notion of ‘surgical outcome’ which is often used to analyse the quality of surgery; this is then used in arguments for high volume centres. He suggested instead that assessing quality needs Quality Indicators and one alone isn’t sufficient. His group in Canada used their national database to propose 32 Quality Indicators, which are valid, reliable, feasible and useable; they found that higher quality had lower mortality and morbidity. Patient centred care, patient selection, high quality surgery and recovery was a common theme in other sessions too.
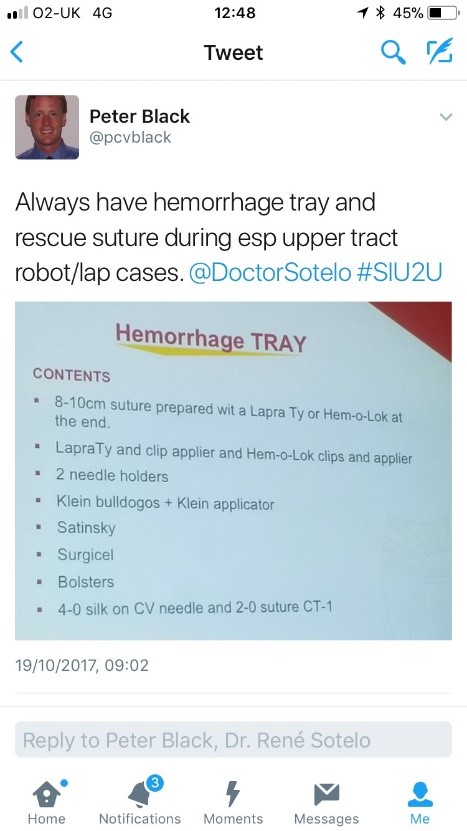
The SIU Innovators Symposium didn’t disappoint; highlights included Dr Sotelo’s presentation of ‘sticky situations’ in robotic surgery. His operative videos showed all the things you really don’t want to see whilst operating, however he and the panel provided tips in order to avoid or correct these operative mistakes. Dr Sotelo’s advice regarding having a ‘haemorrhage tray’ present was ingenious and useful: pictured. Thank you to Dr Sotelo and Dr Knudsen who shared their operative videos with us in order to provide this learning; mistakes in surgery should be shared to avoid others making the same mistakes. The symposium also invited two influential leaders, Professor Prokar Dasgupta, editor BJUI, and Professor Arnulf Stenzl to give their approach on leadership. Prof Stenzl suggested it was easier to explain how not to be a bad leader as he has learnt more from his mistakes than from successes. Prof Dasgupta suggested his leadership style was to be collaborative, trusting team members to deliver, democratic and transformative; also that he, as a leader, wanted to “help other people do well”.
SIU had a strong presence of trainees; many attending to present their academic work during the moderated poster sessions, listen to worldwide experts and of course network with others from around the world and generating future collaborations. One session ‘Sage Advice from the Wise’ was particularly aimed at trainees’ where Urological trainees met 10 experts (all wise, but certainly not old!). We were able to discuss career plans, ask questions about fellowships and talk about the advantages of academia alongside clinical practice. There was also a Residents Rapid Fire Q&A which was won by Dr Avinash Odugoudar: pictured.
Urological cancer treatment featured heavily on the programme. One particularly inspiring talk on advanced testicular cancer by one of the leading surgeons in Europe, Axel Heidenreich, really expanded our horizons of just what can be achieved operatively for patients with metastatic disease, including aortic resection and Whipple’s procedure. It proves that big, open surgery does exist in urology for the right patients; requiring expertise and courageous surgical skills but offering patients treatment despite disseminated disease. One session included debating the use of routine radiation for positive surgical margins in prostate cancer. The presentations by Dr Dall’Ezra and Dr Briganti actually came to very similar conclusions. Both wanted to avoid over treatment and championed a risk stratified approach with emphasis on patient selection; as not all those with positive margins recur. It was suggested that choosing those at greatest risk of recurrence for example the site(s) of positive margin, high Gleason score, early rise in PSA (even if remains less than 0.5) and ultra-sensitive PSA can help to stratify need for adjuvant radiotherapy; or alternatively monitor with option for salvage treatment.
Robotic assisted surgery for prostatectomy, cystectomy and nephrectomy was debated freely throughout the congress. Most quoted recent evidence that there is no clear advantage with regards to blood loss, LOS, long term outcomes and survival; but very different costs. Dr Mihir Desai argued that if you already had the robot you should encourage high volume surgery, but that departments have a responsibility to put the robot to good use; not for simple cases, but rather be reserved for difficult operations so the real advantages of robotic assisted surgery will be better appreciated. Criticism was made of RCTs not being the right research method for comparing surgical techniques as it leads to comparison of individuals not techniques. We eagerly anticipate the iROC study. An important point made regarding robotic cystectomy was that it must include intra-corporeal bladder formation, otherwise many of the advantages of the minimally invasive part are lost. Laparoscopic surgery was argued as not old fashioned; but rather an efficient and cost effective method of minimal access surgery without compromising on outcomes. However open surgery is still an option in many hospitals worldwide; a question from the audience included the dilemma faced by departments whose similar outcomes between open and laparoscopic procedures do not justify the switch to laparoscopy.
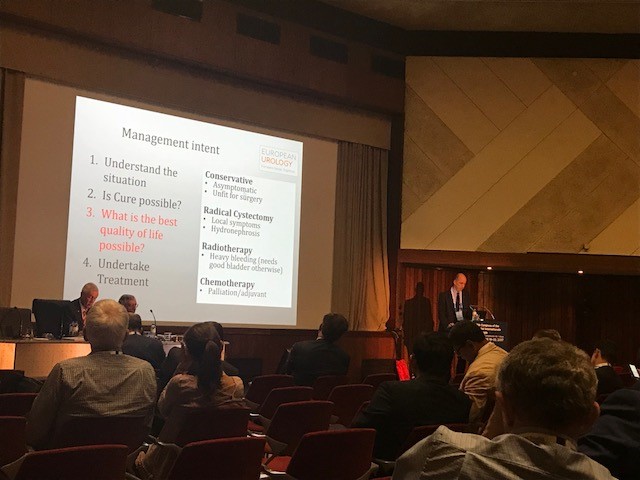
Prof Catto, editor of European Journal of urology delivered a compelling presentation of the advantages of radical cystectomy over radiotherapy for locally advanced bladder cancer. He also mentioned the importance of surgical planning and management intent: pictured. In some cases he does pre-operative MRI, however a PET scan when organised, doesn’t necessarily change his management. He also presented a plenary lecture on risk factors for upper tract TCC which confirmed smoking as the number one risk as well as occupation. However combustion occupations and amine-relate occupations show a difference in cancer aggression suggesting the biology of the cancer is different. Like others, he wanted to aim for personalised treatment of cancer with specific treatments according to genotype.
Debating the merits of surgery was a common theme in several sessions, perhaps unsurprisingly. However a particular highlight was the debate of medical vs surgical theory for lichen sclerosis (LS). The clear and compelling argument by Bradley Erickson for medical treatment rested on 10 points, which included: that LS is an inflammatory condition and these are not necessarily managed by surgery, the dermatologist and gynaecologist manage LS without surgery, LS in the urethra demonstrates squamous change which is reversible and lastly that we don’t really fully understand this disease yet.
Female urology was the first plenary session of the congress and the use of mesh unsurprisingly featured in other sessions, included one entitled ‘controversies in urology’. The clear message from Dr Badlani was to know the anatomy and not to ‘have a go’ at continence surgery, it needs expertise. He and his panel presented difficult cases including mesh seen at cystoscopy, operative video of hydro-dissection and an image of compete extrusion which led the audience to wonder if it had even been placed correctly in the first place!?
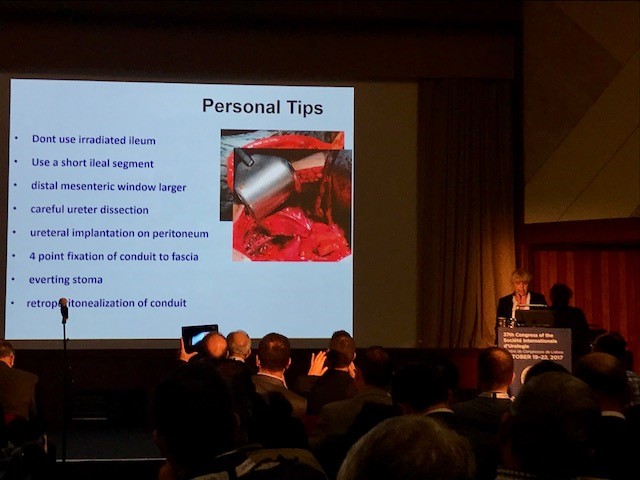
In the joint SIU-GURS meeting panel members each presented a challenging case from their experience of reconstructive surgery and ileal conduit formation; then this was discussed amongst the panel. There was an amazing X-ray of a huge stone in an ileal conduit due to stasis of urine, confirming the need to avoid long conduits. A fear held by many was early failure of the anastomosis; when debating when to re-operate, I particularly liked the phrase “three months to let the belly cool down” said with an American drawl. Margit Fisch shared her top tips of surgery: pictured. An insight into managing continence in patients with Spina Bifida was succinctly presented by Sean P. Elliot; he advised that the patients needed to be ‘proud of their stoma’ and that each needed an individual surgical plan but holistic approach.
Endourology and stone sessions were well attended and each explored different treatment modalities for stone management. Plus the congress offered masterclasses for ureteroscopic techniques, the joint SIU-Endourology session, poster sessions and a ‘controversies session’ debating URS vs Mini-perc. There was also an instructional course on lasers and flexible ureteroscopic technique. Experienced surgeons from across the globe argued for and against the role of ESWL vs RIRS vs PCNL in modern practice. Aside from patient and stone factors there was an appreciable point made of the importance of surgeon experience and available resources of the institution. Non-surgical aspects of stones were also presented, such as diet and hydration in stone disease. Advances in stone surgery, including a robotic assisted ureteroscope was particular enlightening and futuristic; however brought up the inevitable dilemma of clinical need for such technology at a time of financial restraint facing many healthcare systems.
Andrology sessions included a joint SIU-ISSM session, a master class on urethral stricture disease, video session on male reconstruction and poster session on sexual function and dysfunction. There was a debate on the role of the urologist in the management of male infertility and improving sperm. The (interesting) use of an acronym F.A.S.T was described by host urologist from Portugal Dr Pedro Vendeira: pictured. This is in relation to the follow up of non-responders to PDE-5 inhibitors, of which non responders were those who had tried these medications more than eight times. He described a 50% drop out of the use of these drugs due to cost, side effects and co-morbidities. The difficulty of treating Peyronies was discussed by Dr Moncada who confirmed the absence of the role for medical therapies, except use of PDE-5 inhibitors to strengthen erections. There was a role for ‘ penile rehabilitation’ which included a (peculiar) traction device. He presented his and the EAU indications for surgery and he stressed the importance of managing patient expectation and informed consent.
In conclusion, the SIU Congress was both informative and enjoyable. Our co-hosts promises: of warmth, friendship and the Portuguese tradition of sharing wine were delivered alongside a beneficial education programme. Those that did not attend can access abstracts and lectures online via the SIU@U platform.
SIU are also increasing their activities with the following initiatives: ‘B2B’ bench to bedside, ‘Uro-Technology’ training and ‘U-care’ a global urological research collaboration. SIU also wants to build on the opportunities for global education and global health; plus help colleagues without same level of resources.
Thank you to the SIU organisers for a successful congress! Thank you to the presenters and speakers for their expertise and dedication to academia in urology; and congratulations to all the prize winners. I’m sure the next SIU Congress 2018 in South Korea will be equally successful.
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying comment written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Recent advances in immuno-oncology and its application to urological cancers
Recent advances in immuno-oncology have the potential to transform the practice of medical oncology. Antibodies directed against negative regulators of T-cell function (checkpoint inhibitors), engineered cell therapies and innate immune stimulators, such as oncolytic viruses, are effective in a wide range of cancers. Immune‘based therapies have had a clinically meaningful impact on the treatment of advanced melanoma, and the lessons regarding use of single agents and combinations in melanoma may be applicable to the treatment of urological cancers. Checkpoint inhibitors, cytokine therapy and therapeutic vaccines are already showing promise in urothelial bladder cancer, renal cell carcinoma and prostate cancer. Critical areas of future immuno-oncology research include the prospective identification of patients who will respond to current immune-based cancer therapies and the identification of new therapeutic agents that promote immune priming in tumours, and increase the rate of durable clinical responses.
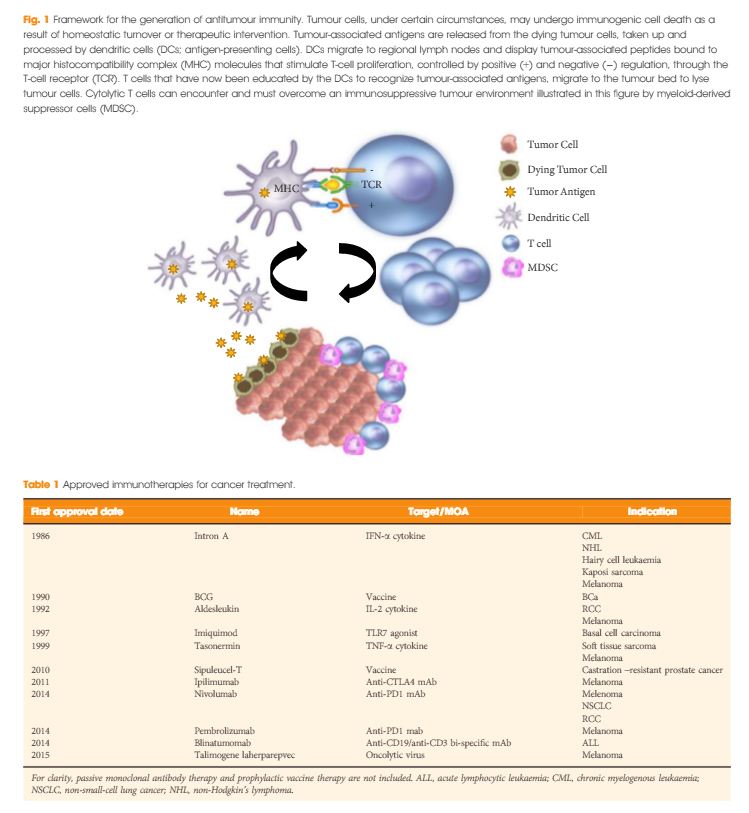
In the last few years there have been concerted attempts at using the power of the immune system as an effective treatment option for cancer. This has become possible as our understanding of the workings of the immune system has improved. Tumours form because of failure of the organism to destroy a rogue, mutated cell in an appropriate way. Once the tumour is formed it can further develop when the immune system fails to contain and control it and certain equilibrium is lost in favour of the tumour. This is referred to as the immune editing theory. At this point of failure of the immune system, tumour growth and progression become possible and tumours develop various mechanisms to evade the immune systems surveillance. Therefore, a mechanism to restore the lost equilibrium or to tip it in favour of the immune system would be a new modality in anti-cancer treatment. The initial approach was to use stimulators of the immune system systemically such as interleukin 2 and interferon γ i.v. in patients with metastatic cancers including melanoma and renal cancers [1]. A sustained response was shown in 22% of patients with metastatic kidney cancer, lasting for over a year. Although this treatment was not a resounding success, it did highlight an approach that could yield a durable tumour regression in a minority of cases. As our understanding of the immune system–tumour interaction further developed, new research focused on a specific mechanism in the immune system that seems to be exploited by tumours. This is an activation-inhibition mechanism, which controls the extent of adaptive immune response to invading organisms or to mutated cancer cells. In healthy individuals, this mechanism is a ‘safety’ feature allowing cessation of the immune response once it has performed its task. This is controlled by ‘receptor’ molecules at the T-cell surface and their corresponding ‘ligands’ at the surface of the cells interacting with the T-cell, which can be an antigen presenting cell or a tumour cell surface. This mechanism is called the immune checkpoint [2] (Fig. 1). Cytotoxic T lymphocyte antigen 4 (CTLA-4) and programmed death 1 (PD-1) are the most well-known checkpoints but there are up to 20 others (and counting) [2]. Their main role is to inhibit an immune response by blocking the activation of T-cells when those cells are presented with a foreign antigen or cancer proteins. This inhibition leads to immune ‘tolerance’ of the presence of cancer cells. So the policeman (T cell) is oblivious to the robbery in front of him. Thus an anti-tumour treatment strategy to disrupt the immune checkpoints seems to be a valid one (Table 1).
Figure 1. Blocking checkpoint inhibitors with antibodies is the new immunotherapy strategy to unlock T-cell activation and improve anti-tumour immune response. MHC, major histocompatibility complex; PD-L1, programmed death ligand 1; TCR, T-cell antigen receptor.
Table 1. A selected group of trials of immune checkpoint inhibitors in urological cancers
Tumour
Phase
Treatment
N
Results
Trial.gov identifier
mCRPC, metastatic castrate-resistant prostate cancer; PD-L1, programmed death ligand 1. The total number of current trials of immune checkpoint inhibitors is 46 for lung, breast, ovarian, rectal, prostate, pancreatic, bladder, renal cancers and melanoma.
mCRPC
1
Dendritic cell therapy and ipilimumab
20
Recruiting
NCT02423928
All advanced solid tumours
1
Various combinations of ipilimumab, nivolumab and pembrolizumab
122
Recruiting
NCT02467361
RCC
3
Nivolumab vs everolimus
822
Recruiting
NCT01668784
RCC
3
Atezolizumab (anti PD-L1)
70
Good safety profile with antitumour activity
NCT01375842
mCRPC
3
Ipilimumab vs placebo
799
No improvement of survival in treatment group
NCT00861614
Urothelial
2
Gemcitabine, cisplatin and ipilimumab combinations
36
Recruiting
NCT01524991
In recent years, a plethora of various inhibitors in the form of monoclonal antibodies to the checkpoint molecules were developed and to date three at least have been approved by the USA Food and Drug Administration (FDA) – ipilimumab (Yervoy), nivolumab (Opdivo), and pembrolizumab (Keytruda). They are anti-CTLA4 and anti-PD-1 antibodies. At least another eight checkpoint inhibitors are being developed. These agents have been shown to have survival benefit in some malignancies and limited benefit in others. However, the breakthrough seems to be happening in the treatment of metastatic malignant melanomas where immune checkpoint inhibitors treatment may become the standard of care. Patients with metastatic malignant melanoma who were treated with ipilimumab had a median survival of ~11 months; however, 22% of patients survived for ≥3 years with a plateau in the survival curve and in a subset of patients up to 10 years [3]. This success has not yet been replicated in prostate cancer [4]. In a more recent clinical trial involving patients with melanoma who progressed, nivolumab showed survival benefit of 72% at 1 year as compared with 42% with dacarbazine [5]. The latest approach is to combine anti-CTLA-4 and anti-PD-1 in one treatment regime as they are expected to act synergistically to remove the inhibition to the immune response, and clinical results seem to show survival benefit for combined therapy [6]. Combination of different treatment methods may potentiate the ‘abscopal effect’, which is seen when local radiation therapy can cause regression of tumour distant to the radiation site. This seems to be mediated by the immune system and potentiated by checkpoint inhibitors. Until now checkpoint inhibitors were used in patients with end-stage metastatic cancer, but recently anti-CTLA-4 has been trialled in pre-radical cystectomy patients not as a neoadjuvant therapy but rather to monitor immune response and surgical safety [2]. It is likely that checkpoint inhibitors will have a place in cancer treatment including urological cancers. However, this new class of anti-cancer treatment comes with a price. The emerging risks and side-effect profile of checkpoint inhibitors are completely different from those seen with the conventional chemotherapy and radiotherapy. Those side-effects are related to the activation of the immune system. Although most are not uncommon, they can occasionally have devastating effect on the patients. These side-effects include autoimmune conditions like dermatitis, mild colitis, and occasionally hepatitis. A severe form of colitis resulting in perforation has been reported. Unfortunately, the rate of adverse effects seems to correlate with positive clinical response. A list of some of the side-effects is summarised in Table 2. Treatment is usually with steroids, and clinicians are starting to develop strategies to minimise those risks.
Table 2. Autoimmune-based adverse effects that are associated with immune checkpoint inhibitors treatment. Most are tolerated. Severe ones are rare but can be devastating. Treatment is usually with steroids [2, 5, 6]
Adverse effects
Common
Rare
Diarrhoea
Severe colitis – colonic perforation
Pruritus/dermatitis
Adrenal insufficiency
Rash
Panhypopituitarism
Colitis
Hepatitis
Fatigue
Uveitis
Decreased appetite
Temporal arteritis
The cost of checkpoint inhibitors remains relatively high and a full treatment course of ipilimumab costs >£18 000. One dose of pembrolizumab can cost >£3 500. However, the National Institute for Health and Care excellence (NICE) in the UK deemed this to be cost-effective and approved it for patients with metastatic melanoma that has progressed despite ipilimumab treatment.
Will the 21st century be the era for immunotherapy? It is still too early to tell. At present it remains rather expensive and beyond the means of many patients with cancer.
After briefly venturing to tropical Cairns in 2015, the Asia-Pacific Prostate Cancer Conference returned to its traditional home in Melbourne for its 17th edition in 2016 (#APCC16). The meeting has previously featured the who’s who of prostate cancer and this year was no different with an all-star multidisciplinary faculty consisting of 18 international members in addition to our local experts. The meeting was well attended by over the 750 delegates from all parts of the globe and remains one of the largest prostate cancer educational events worldwide.
Conference president Professor Tony Costello opened the conference with the famous Whitmore aphorisms and outlined the impressive progress and discoveries we have made in the field over the last century. The first case of prostate cancer was described in 1853 in the London Hospital and was noted by the surgeon to be a “very rare disease” whereas now it is known to be the most commonly diagnosed malignancy amongst men. Pleasingly, research and emphasis on men’s health has grown with the disease highlighted by the newly completed, world-class Parkville Biomedical precinct in Melbourne, which includes “The Royal Men’s Hospital” (@APCR). Melbourne’s Lord Mayor (@LordMayorMelb) also dropped-by to reiterate his support for the meeting and the advancements made in men’s health.
In what is becoming an annual tradition, honourary Melbournian and Australian, Dr Stacy Loeb (@LoebStacy) once again got the sessions off to a flying start by delivering the ‘prostate cancer year in review’ which was an excellent overview of the abstracts produced over the last 12 months. The male attendees in particular were excited by the recent paper suggesting that more than 21 ejaculations per month acted as a protective factor for the development of prostate cancer. Although confounding factors may have played a role in the association seen, these were easily over-looked and its results were accepted as gospel and promoted as a public health message. The abstract featured the following day on the home page of The Australian Financial Review (https://www.afr.com/lifestyle/health/mens-health/tell-your-partner-frequency-counts-even-against-cancer-20160831-gr5fs4) – who knew that the answer to the world economic problems was so simple!
The meeting did however become more scientific as we heard from a range of international and local experts on the challenges of trying to find the balance of precision oncology in a time of tumour heterogeneity. It was clear that the future has arrived with recent advances in the field of genomics and biomarkers. These discoveries appear to be only the tip of the iceberg and further research holds the key in understanding tumour behavior in order to tailor treatment on a patient-to-patient level. Having witnessed a variety of experts from all parts of the globe present their finding there is little doubt that a major breakthrough is just around the corner. A special mention to Dr Niall Corcoran whose research was of such high quality that A/Prof Henry Woo (@DrHWoo) raised the white flag early in the Melbourne vs. Sydney inter-city rivalry.
The named lectures of #APCC16 were highlights of the conference. Keeping with the theme of the first morning, Dr Martin Gleave delivered the 4th Patrick C Walsh lecture titled ‘Two Tales of Precision Oncology.” Prof Peter Wiklund gave the inaugural ERUS lecture on the role of surgery for high risk and metastatic prostate cancer.
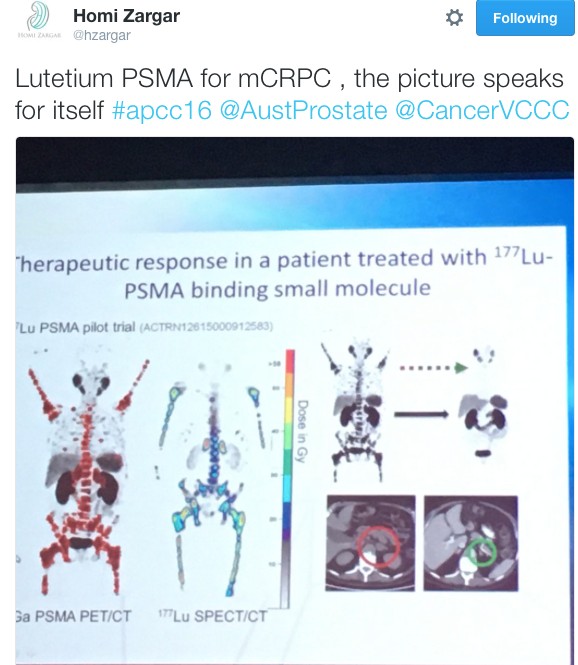
It wouldn’t have been a prostate cancer conference without the age-old debate of surgery vs. radiotherapy being revisited. Over three days Dr Robert Nam presented a series of talks on Canadian long-term outcomes and meta-analysis showing favourable results for team surgery. He also predicted that the highly anticipated ProtecT randomised trial due in the NEJM would show no difference ensuring the debate prolongs into the future and vowed to “eat my shorts” if the trial demonstrated a result favouring either modality. Dr John Violet flew the flag strongly for radiation oncologists in presenting the promising outcomes for 177Lu-PSMA in the mCRPC setting. Similarly, Dr Andrew Kneebone presented a compelling case for stereotactic radiation for oligometastatic disease.
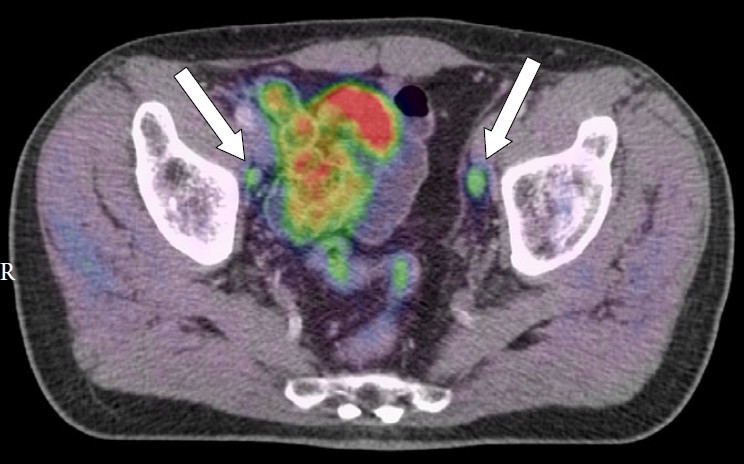
Imaging of the prostate was a hot topic throughout the conference. The excitement around PSMA-PET was at a climax following The Victorian Comprehensive Cancer Centre’s (@VCCC) experience that was presented by Associate Professors Michael Hofman (@DrMHofman) and Nathan Lawrentschuk (@lawrentschuk). The proceeding panel discussion focused on how to best utilise the technology and the role it currently plays in the prostate cancer landscape. Despite not being FDA approved, its role in evaluating recurrence appears to be entrenched with data to support its superiority over other modalities but it was also proposed that it might have a place in initial staging of high-risk cancer. The advancement of PSMA over conventional imaging also raised the question of how we now interpret previous trials such as CHAARTED and STAMPEDE whose results are based on superseded technology.
The hype surrounding PSMA-PET only just eclipsed that of mpMRI in the imaging landscape. Professor Philip Stricker presented a nomogram, which integrated MRI in determining who to biopsy and Dr Rob Reiter reported a terrific novel study of using 3D modeling to compare MRI results to final histopathology to determine correlation but did caution us with performing targeted biopsies alone which risks missing clinically significant cancers. Dr Nam also chimed in with a pilot study of using MRI as a screening test.
Suspense was built until Friday for the highly anticipated session on open vs. robotic surgery featuring the first presentation of the Brisbane RCT. The results of the trial have been already widely debated in the urological community and a discussion similar to the recent BJUI blog (https://www.bjuinternational.com/bjui-blog/its-not-about-the-machine-stupid/) ensued. Regardless of individual opinions on the trial, there is no dispute about the volume of work required to conduct a surgical randomised trial and there was wide praise for the efforts of the Brisbane team. Prof Peter Wiklund and Dr Homi Zargar (@hzargar) also reported the Swedish and Victorian experience respectively. The overall consensus was that robotic surgery offers the benefit of minimally invasive surgery but it is the surgeon rather than the modality, which has the most significant impact on outcomes.
There was a strong multi-disciplinary theme throughout the conference. The Nursing & Allied Health and Translational Science streams both had strong contingents attending. The quality of research presented and engagement amongst attendee was of the highest standard. This was exemplified by the session ‘MDT 2020’, which was a case-centred discussion by a panel of experts from a variety of professions and highlighted the value of a multidisciplinary approach in patient care.
The social program of #APCC16 was not overshadowed by its academic counterpart. The conference dinner was held at The Glasshouse where the food was exquisite and entertainment was provided by three waiters come tenors. Their classical renditions were received by guests with napkin twirling and swinging wine glasses. The frivolities were thoroughly enjoyed by all.
We would like to congratulate all attendees and their teams on the abstracts presented throughout the conference. The BJUI once again proudly supported the meeting with all accepted abstracts published in a special supplements issue and BJUI Associate Editors Declan Murphy (@declanmurphy), John Davis, and Nathan Lawrentschuk being prominent figures throughout the conference. A special mention to the poster prize winners from this year:
Clinical Urology: Jonathan Kam – Do multi-parametric MRI guided biopsies add value to the standard systematic prostate needle biopsy? – early experience in an Australian regional centre
Nursing & Allied Health: Thea Richardson – An Androgen Deprivation Therapy Clinic: An integrative approach to treatment
Translational Science: Natalie Kurganovs – Identifying the origins and drivers of castration resistant prostate cancer
On behalf of all the delegates, we thank the entire international and local faculty who shared their knowledge over the conference and devote their time to improving men’s health. Furthermore, meetings such as this would not occur without the unheralded behind the scenes work. We extend our thanks to president Prof Costello, the convenors of the streams (A/Prof Declan Murphy, Dr Niall Corcoran, A/Prof Chris Hovens, Ms Helen Crowe (@helenrcrowe) & Mr Dave Gray (@DavidGrayAust)) and the APCC committee. We also graciously thank our sponsors without whom none of this would be possible and are vital to further advancements in men’s health.
Last but not least, given the rich history of social media seen at this conference, it would be remiss not to acknowledge another #SoMe landmark. Melbourne has previously been responsible in welcoming urology SoMe royalty, Dr Stacy Loeb, to the twitter world and this year the twitterati were introduced to Dr Peter Carroll (@pcarroll_). He managed to send out 4 tweets and eclipse 100 followers before the end of the conference.
#APCC17 will return to Melbourne on 30th of August 2017 – we hope to see you there!
Dr Niranjan Sathianathen (@NiranjanJS) is a researcher at Peter MacCallum Cancer Centre, Melbourne.