What’s the Diagnosis?
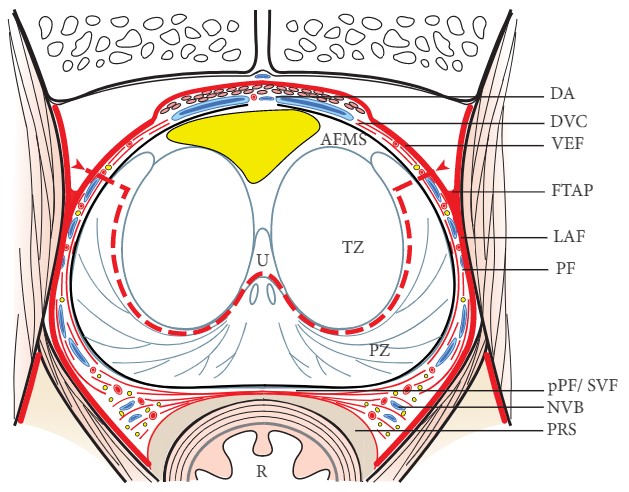
This image is taken from Villers et al, BJUI 2017 who describe the step-by-step technique of partial anterior prostatectomy.
No such quiz/survey/poll
This image is taken from Villers et al, BJUI 2017 who describe the step-by-step technique of partial anterior prostatectomy.
No such quiz/survey/poll
 Ever since 2002, I have performed live surgery almost every year where it is transmitted to an audience eager to learn. This year I was invited by Markus Hohenfellner to the unique conference, Semi Live 2017 in Heidelberg. To say that it was an eye opener is perhaps stating the obvious. One look at the program will show you that the worlds most respected Urological surgeons had been invited to participate, but with a difference. There was no live surgery. Instead videos of operations – open, laparoscopic and robotic were shared with the attendees “warts and all” as a learning experience. These were not videos designed to show the best parts of an operation. There were plenty of difficult moments, do’s and don’ts and troubleshooting, but all this was achieved without causing harm or potential harm to a single patient.
Ever since 2002, I have performed live surgery almost every year where it is transmitted to an audience eager to learn. This year I was invited by Markus Hohenfellner to the unique conference, Semi Live 2017 in Heidelberg. To say that it was an eye opener is perhaps stating the obvious. One look at the program will show you that the worlds most respected Urological surgeons had been invited to participate, but with a difference. There was no live surgery. Instead videos of operations – open, laparoscopic and robotic were shared with the attendees “warts and all” as a learning experience. These were not videos designed to show the best parts of an operation. There were plenty of difficult moments, do’s and don’ts and troubleshooting, but all this was achieved without causing harm or potential harm to a single patient.
My highlights were laparoscopic sacrocolpopexy (Gaston), robotic IVC thrombectomy up to the right atrium (Zhang) and reconstructive surgery for the buried penis (Santucci). The event takes place every 2 years and the videos are all available on the meeting app which can be downloaded here and is an outstanding educational resource.
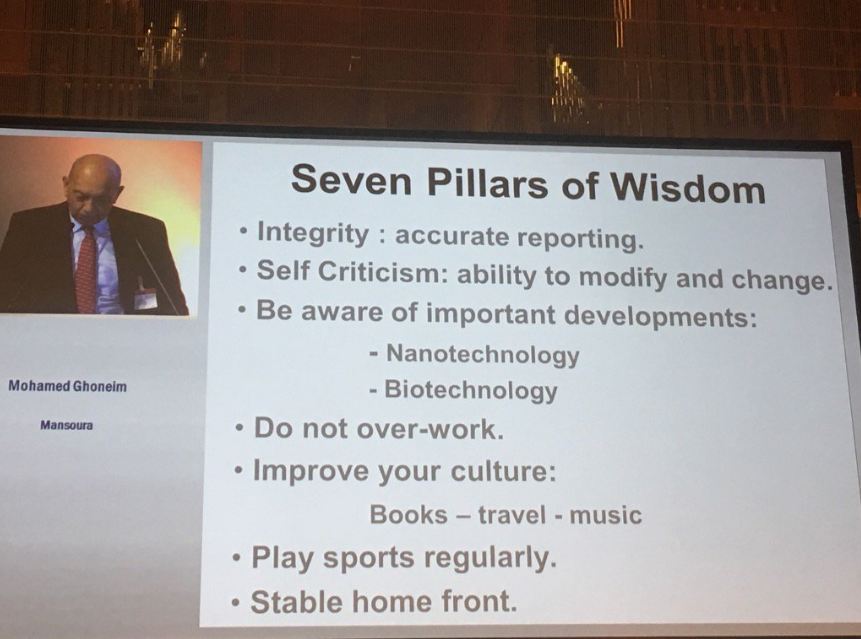
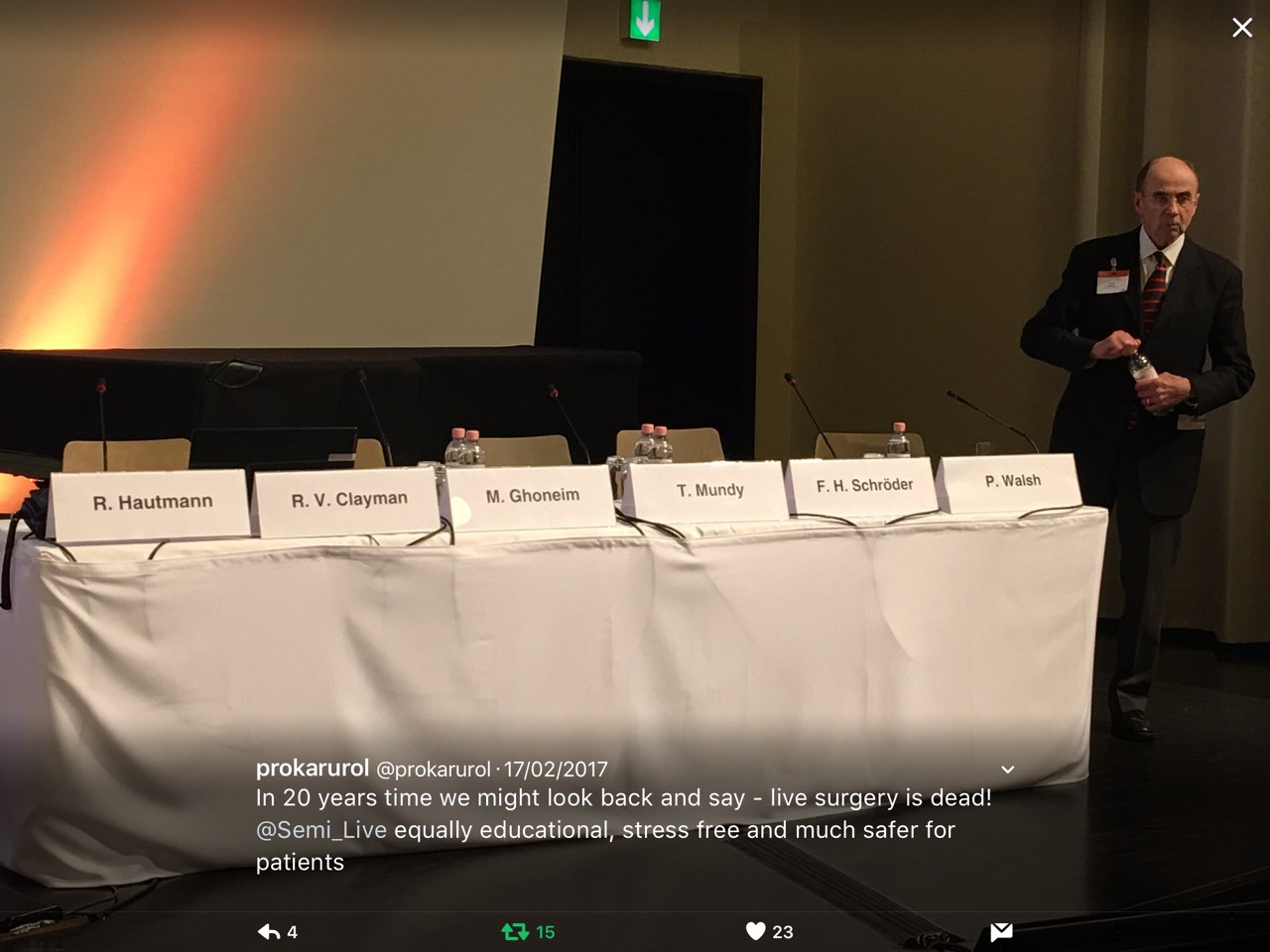
We were treated to a heritage session which included the superstars Walsh, Hautmann, Clayman, Mundy, Schroder and Ghoneim. This was followed by our host Markus Hohenfellner comparing and contrasting the art of Cystectomy and reconstruction by Ghoneim, Stenzl and Studer.
Open surgery is certainly not dead yet. The session ended with Seven Pillars of Wisdom from Egypt which turned out to be a big hit on Twitter.
The editor’s choice session, a new innovation for 2017, allowed me to showcase the Best of BJUI Step by Step, a section that has now replaced Surgery Illustrated with fully indexed and citable HD videos and short papers.
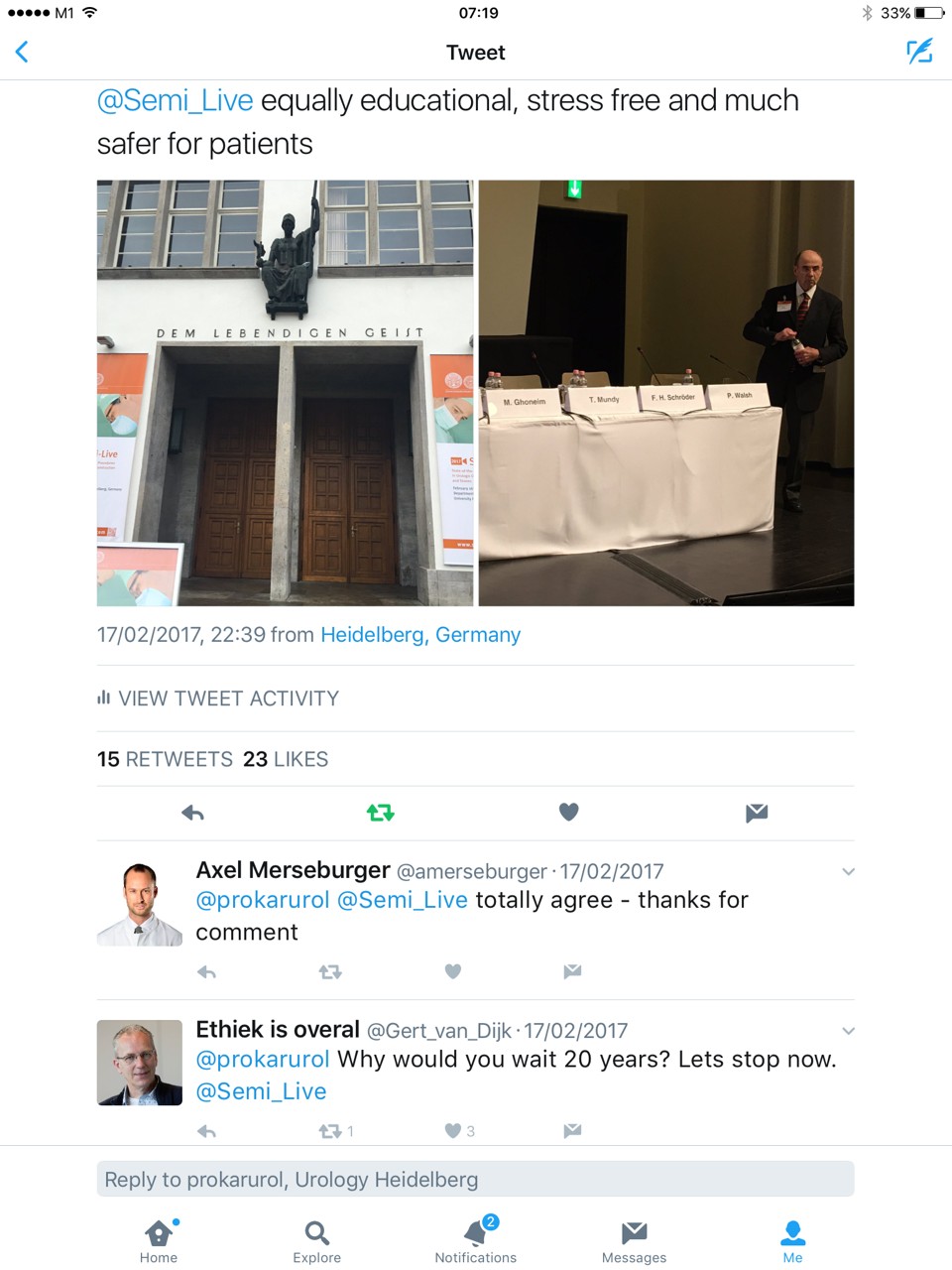
Many on Twitter seemed to agree that in 20 years time we might look back and say that it was not the right thing to do.
Surgeons do not operate “live” every day. Most doctors in a survey, would not subject themselves or their families to be patients during live surgery. Talk about hypocrisy!! Why should it be any different for our patients? Live surgery is NOT a blood sport practised in Roman times….
The counterpoint is that patients often have the services of the best surgeons during live surgery, recorded, edited videos are not quite the same and that the whole affair has become safer thanks to patient advocates and strict guidelines from some organisations like the EAU. Others have banned the practice for good reason. While the debate continues, I for one came away feeling that Semi-Live was as educational, less stressful and much safer for our patients.
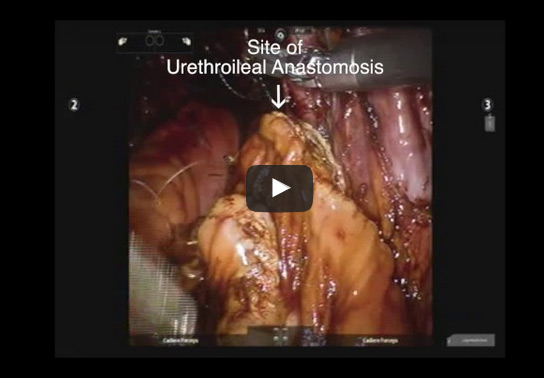
To describe our, step-by-step, technique for robotic intracorporeal neobladder formation.
The main surgical steps to forming the intracorporeal orthotopic ileal neobladder are: isolation of 65 cm of small bowel; small bowel anastomosis; bowel detubularisation; suture of the posterior wall of the neobladder; neobladder–urethral anastomosis and cross folding of the pouch; and uretero-enteral anastomosis. Improvements have been made to these steps to enhance time efficiency without compromising neobladder configuration.
Our technical improvements have resulted in an improvement in operative time from 450 to 360 min.
We describe an updated step-by-step technique of robot-assisted intracorporeal orthotopic ileal neobladder formation.

To outline our step-by-step technique for intracorporeal renal cooling during robot-assisted partial nephrectomy (RAPN).
Patient selection was performed during a preoperative clinic visit. Cases where we estimated during preoperative assessment that warm ischaemia time would be >30 min, as determined by whether the patient had a complex renal mass, were selected. The special equipment required for this procedure includes an Ecolab Hush Slush machine (Microtek Medical Inc., Columbus, MS, USA) a Mon-a-therm needle thermocouple device (Covidien, Mansfield, MA, USA) and six modified 20-mL syringes. Patients are arranged in a 60° modified flank position with the operating table flexed slightly at the level of the anterior superior iliac spine. For the introduction of a temperature probe and ice slush, an additional 12-mm trocar is placed along the mid-axillary line beneath the costal margin. Modified 10/20 mL syringes are prefilled with ice slush for instillation via an accessory trocar. Peri-operative and 6-month functional outcomes in the cold ischaemia group were compared with those of a cohort of patients who underwent RAPN with warm ischaemia in a 2:1 matched fashion. Matching was performed based on preoperative estimated glomerular filtration rate (GFR), ischaemia time and RENAL nephrometry score.
Strategies for successful intracorporeal renal cooling include: (i) placement of accessory port directly over the kidney; (ii) uniform ice consistency and modified syringes; (iii) sequential clamping of renal artery and vein; (iv) protection of the neighbouring intestine with a laparoscopic sponge; and (v) complete mobilization of the kidney. Kidney temperature is monitored via a needle thermocoupler device, while core body temperature is concurrently monitored via an oesophageal probe in real time. Renal function was assessed by serum creatinine level, estimated GFR (eGFR) and mercaptoacetyltriglycine (MAG-3) renal scan, peri-operatively and at 6-month follow-up. In the separate matched analysis, cold ischaemia during RAPN was found to be associated with a 12.9% improvement in preservation of postoperative eGFR. No difference was seen in either group at 6-month follow-up.
We conclude that RAPN with intracorporeal renal hypothermia using ice slush is technically feasible and may improve postoperative renal function in the short term. Our technique for intracorporeal hypotheramia is cost-effective, simple and highly reproducible.

To describe a novel, step-by-step approach to robot-assisted extended pelvic lymph node dissection (ePLND) at the time of robot-assisted radical prostatectomy (RARP) for intermediate–high risk prostate cancer.
The sequence of ePLND is at the beginning of the operation to take advantage of greater visibility of the deeper hypogastric planes. The urachus is left intact for an exposure/retraction point. The anatomy is described in terms of lymph nodes (LNs) that are easily retrieved vs those that require additional manipulation of the anatomy, and a determined surgeon. A representative cohort of 167 RARPs was queried for representative metrics that distinguish the ePLND: 146 primary cases and 21 with neoadjuvant systemic therapy.
The median (interquartile range, IQR) LN yield was 22 (16–28) for primary surgeries and 21 (16–23) for neoadjuvant cases. The percentage of cases with positive LNs (pN1) was 16.4% for primary and 29% for neoadjuvant. The hypogastric LNs were involved in 75% of pN1 primary cases and uniquely positive in 33%. Each side of ePLND took the attending surgeon a median (IQR) of 16 (13–20) min and trainees 25 (24–38) min.
Robot-assisted ePLND before RARP provides an anatomical approach to surgical extirpation mimicking the open approach. We think this sequence offers efficiency and efficacy advantages in high-risk and select intermediate-risk patients with prostate cancer undergoing RARP.
Andre Luis de Castro Abreu, Duke Bahn*, Sameer Chopra, Scott Leslie, Toru Matsugasumi, Inderbir S. Gill and Osamu Ukimura
USC Institute of Urology, Catherine and Joseph Aresty Department of Urology, Center for Prostate Cancer Focal Therapy, Keck School of Medicine, University of Southern California, Los Angeles, and *Prostate Institute of America, Community Memorial Hospital, Ventura, CA, USA
How to Cite: de Castro Abreu, A. L., Bahn, D., Chopra, S., Leslie, S., Matsugasumi, T., Gill, I. S. and Ukimura, O. (2014), Real-time transrectal ultrasonography-guided hands-free technique for focal cryoablation of the prostate. BJU International, 114: 784–789. doi: 10.1111/bju.12795
To describe, step-by-step, our hands-free technique for focal cryoablation of prostate cancer.
After detailed discussion of its limitations and benefits, consent was obtained to perform focal cryoablation in patients with biopsy-proven unilateral low- to intermediate-risk prostate cancer. The procedure was performed transperineally, using a hands-free technique (without an external grid template) under real-time bi-plane transrectal ultrasonography (TRUS) guidance, using an argon/helium-gas-based third generation cryoablation system. Follow-up consisted of validated questionnaires, physical examination, PSA measures, multiparametric TRUS and/or magnetic resonance imaging (MRI) and mandatory biopsy.
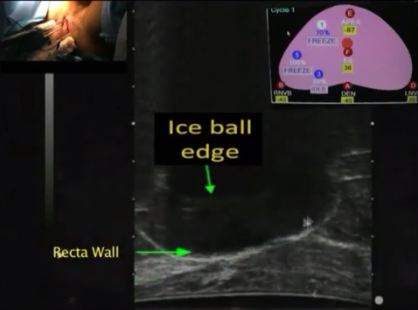
The important steps for achieving safety, satisfactory oncological and functional outcomes included: patient selection, including TRUS/MRI fusion target biopsy; thermocouple and cryoprobe placement with a hands-free technique, allowing delivery in unrestricted angulations according to the prostatic contour, the course of the neurovascular bundle and the rectal wall angle; and hands-free bi-plane TRUS probe manipulation to facilitate real-time monitoring of anatomical landmarks at the ideal angle of the image plane. To achieve a lethal temperature in the known cancer area, while preserving the urinary sphincter, neurovascular bundle, urethra and rectal wall, continuous intraoperative control of the thermocouple temperatures was necessary, as were real-time TRUS monitoring of ice-ball size, control of the energy delivered and the use of a warming urethral catheter.
We have described step-by-step the focal cryoablation of prostate cancer using a hands-free technique. This technique facilitates the effective delivery of cryoprobes and the intra-operative real-time quick manipulation of the TRUS probe.

Khurshid R. Ghani, James Porter*, Mani Menon and Craig Rogers
Vattikuti Urology Institute, Henry Ford Hospital, Detroit, MI, and *Department of Urology, Swedish Urology Group, Seattle, WA, USA
To describe a step-by-step guide for successful implementation of the retroperitoneal approach to robotic partial nephrectomy (RPN)
The patient is placed in the flank position and the table fully flexed to increase the space between the 12th rib and iliac crest. Access to the retroperitoneal space is obtained using a balloon-dilating device. Ports include a 12-mm camera port, two 8-mm robotic ports and a 12-mm assistant port placed in the anterior axillary line cephalad to the anterior superior iliac spine, and 7–8 cm caudal to the ipsilateral robotic port.
Positioning and port placement strategies for successful technique include: (i) Docking robot directly over the patient’s head parallel to the spine; (ii) incision for camera port ≈1.9 cm (1 fingerbreadth) above the iliac crest, lateral to the triangle of Petit; (iii) Seldinger technique insertion of kidney-shaped balloon dilator into retroperitoneal space; (iv) Maximising distance between all ports; (v) Ensuring camera arm is placed in the outer part of the ‘sweet spot’.
The retroperitoneal approach to RPN permits direct access to the renal hilum, no need for bowel mobilisation and excellent visualisation of posteriorly located tumours.

Ronney Abaza, Khurshid R. Ghani*, Akshay Sood*, Rajesh Ahlawat†, Ramesh K. Kumar*, Wooju Jeong*, Mahendra Bhandari*, Vijay Kher† and Mani Menon*
Department of Urology, Ohio State University, Columbus, OH, *Vattikuti Urology Institute, Henry Ford Hospital, Detroit, MI, USA, and †Kidney and Urology Institute, Medanta-The Medicity, Gurgaon, India
• To describe a novel and reproducible technique of robotic kidney transplantation (RKT) that requires no repositioning, and permits intraoperative regional hypothermia.
• A GelPOINT™ (Applied Medical, Santa Ranchero, CA, USA) access port was used for delivery of ice-slush and introduction of the graft kidney. The new RKT technique using ice-slush has been performed in 39 patients.
• At a mean follow-up of 3 months all of the grafts functioned. There was a marked reduction in pain and analgesic requirement compared with patients undergoing open KT, with a propensity towards quicker graft recovery and lower complication rate.
• RKT has been shown to be safe and feasible in patients undergoing living-donor related KT. A prospective trial is underway to assess outcomes definitively.

Janak Desai and Ronak Solanki
Department of Urology, Samved Hospital, Ahmedabad, India
• To describe our newly developed technique for the removal of renal stones, which we have called ultra-mini percutaneous nephrolithotomy (UMP).
• UMP was performed in 62 patients using a 3.5-F ultra-thin telescope and specially designed inner and outer sheaths. A standard puncture was made and the tract was dilated up to 13 F.
• The outer sheath was introduced into the pelvicalyceal system and the stone was disintegrated with a 365-μ holmium laser fibre, introduced through the inner sheath.
• Stone fragments were evacuated using the specially designed sheath by creating an eddy current of saline; the fragments then came out automatically.
• The mean calculus size was 16.8 mm. Four of the 62 patients were children, three had a solitary kidney and two were obese.
• UMP was feasible in all cases with a mean (sd) 1.4 (1.0) gm/dL haemoglobin decrease and a mean hospital stay of 1.2 (0.8) days. The stone-free rate at 1 month was 86.66%.
• In two patients intraoperative bleeding obscured vision, requiring conversion to mini-percutaneous nephrolithotomy. There was one postoperative complication of hydrothorax, but there were no other postoperative complications and no auxiliary procedures were required.
• UMP is a very safe and effective method of removing renal calculi up to 20 mm. The use of consumables and disposables is minimal and the patient recovery was fast.
• Further clinical studies and direct comparison with other available techniques are required to define the place of UMP in the treatment of low-bulk and medium-bulk renal urolithiasis. It may be particularly useful for lower calyx calculi and paediatric cases.

Khurshid R. Ghani, Quoc-Dien Trinh, Jesse D. Sammon, Wooju Jeong, Andrea Simone, Ali Dabaja, Stacey Dusik, James O. Peabody and Mani Menon
Vattikuti Urology Institute, Henry Ford Health System, Detroit, MI, USA
• To describe our technique of maintaining bladder drainage after robot-assisted radical prostatectomy (RARP) using a percutaneous suprapubic tube (PST) in place of a urethral catheter.
• A watertight anastomosis permits placement of the PST. Contraindications include morbid obesity, concomitant inguinal hernia mesh repair, anticoagulation therapy, limited hand dexterity in the patient, bladder neck reconstruction and extensive adhesiolysis at RARP.
• The necessary equipment includes a 14-F PST balloon catheter set, a three-way connector, a connecting tube, a suture passer, 1/0 polypropylene sutures on a CT1 needle, a sterile plastic button, adhesive and steri-strips.
• The important steps for PST placement are: Step 1: robot-assisted placement of a bladder wall anchor suture; Step 2: transferring the bladder wall suture to anterior abdominal skin; Step 3: guided placement of the PST under robotic vision; Step 4: securing the PST within the bladder and abdominal wall; Step 5. postoperative care: clamping the PST on postoperative day 5, recording each void and post-void residual urine volumes in a patient diary, removal of the PST on postoperative day 7 after 48 h of voiding with residual urine <100 mL per void.
• We provide a concise step-by-step guide for placement of a PST during RARP as well as important management aspects for the successful adoption of this technique.