
New Gleason grading system: Statement from the Editors of six journals
The International Society of Urologic Pathology (ISUP) has completed a consensus process to modify and clarify the Gleason scoring system for prostate cancers (1). Five grade groups have been defined with tumors of ISUP Grade Group 1 being the least aggressive and having the lowest likelihood of progression, whereas those of ISUP Grade Group 5 have the highest likelihood of early systemic spread. This new system provides clearer guidance for pathologists to classify cancers on the basis of gland morphology, and it aligns better with contemporary management including active surveillance.
The editors of the major uro-oncology journals believe this is a helpful change for clinicians, researchers, and patients alike and are eager to help this system establish itself in the reporting of pathologic grade. To that end we are now asking investigators to use the ISUP system in the reporting of prostate cancers in their publications. As the grade groups correspond largely with current Gleason scores 6, 3+4, 4+3, 8, 9 and 10, the translation should be relatively simple. Over the next one to two years, side-by-side reporting of old and new histology may temporarily be necessary. We do recognize that some institutional and national databases are not set up to make the translation and exceptions will be granted in these cases.
Anthony Zietman MD
International Journal of Radiation Oncology Biology Physics
Joseph Smith MD
Journal of Urology
Eric Klein MD
Urology
Michael Droller MD
Urologic Oncology
Prokar Dasgupta MSc MD FRCS
BJUI
James Catto MBChB PhD FRCS
European Urology
Reference
- Epstein JI, Egevad L, Amin MB et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference of Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2016, 40: 244-252.
Dear Editors,
My views summarised here.
The Gleason system has undergone subtle changes a number of times since it was first proposed. The system currently in use is the modified Gleason grading system. Some of the features described in the consensus paper have slowly crept into practice over the last few years and so the changes described here will not dramatically change pathology reporting practice, rather records the slow drift which started a few years ago when the changes in diagnostic criteria appeared in publications and at update courses and meetings. The new system is really not new at all, rather it provides good evidence for the separation of different Gleason scores. This system may be used in parallel with the modified Gleason grading system but in fact, it is derived directly from them. Clinicians have been using the differences in these groups for clinical decision making and if anything this validates existing clinical practice. My recommendation would be to endorse the use of the ISUP Grade Groups alongside the modified Gleason grading system. There are already a number of courses including those held for pathologists to help them understand and apply the Grade Groups. BAUP endorses its use and the RCPath is currently holding a consultation to introduce some changes in prostate pathology reporting practices after a period of consultation. It would be a good idea for pathology and urology journals to work together in promoting the use of both terminologies side by side (rather like WHO1973 & ISUP2004 for urothelial carcinoma in the UK).
Best wishes,
Ash
Dr Ashish Chandra
MD FRCPath DipRCPath (Cytol)
Lead Consultant for Cytopathology
& Urological Histopathology
St. Thomas’ Hospital
London
The new prostate cancer grading system is incorrectly referred to as the ISUP Grading System and make it seem that the ISUP came up with the new grading system. However, the new grading system was first described in 2013 by work done at The Johns Hopkins Hospital where I was the senior author, and verified by a large multi-institutional study that I led, both prior to the ISUP 2014 consensus conference.(1,2) The new system uses the terms Grade Groups 1-5. The data from these two studies and the rationale and evidence in support of the new grading system were presented to the attendees of the 2014 conference where 90% voted to accept the new grading system. Although the 2005 and 2014 ISUP consensus conferences, which I both chaired or co-chaired, were instrumental in many of the grade changes that are incorporated within the new grading system, the ISUP conferences did not come up with the concept nor did they do the research that lead to the new 5 Grade Groups grading system. (3,4) To therefore re-name the grading system solely as the ISUP Grading System is misleading and inaccurate. The terms ISUP grade 1-5, conflict with the paper first describing the new grading system (1), the subsequent multi-institutional verification study (2), the proceedings from the 2014 ISUP consensus conference published in AJSP in 2016 (4), and the 2016 Edition of the World Health Organization (WHO) of the Pathology and Genetics: Tumours of the Urinary System and Male Genital Organs5, all which refer to the new grading system simply as Grade Groups 1-5. The only formal discussion regarding the name of the new grading system was at the 2014 ISUP Consensus Conference, where a majority vote supported the term “ISUP/Epstein Grades 1-5” to reflect the ISUP’s contributions to modifications of the Gleason system which form the basis of the new grading system as well as the individual’s contribution who came up with the concept of the new 5 grade system, the initial study to support it, as well who lead the multi-institutional validation study. The new grading system should either be named generically “Grade Groups 1-5” or “ISUP/Epstein Grades 1-5″, but not solely ‘ISUP Grades 1-5” which both lacked a majority vote at the 2014 ISUP Consensus Conference and incorrectly implies that the ISUP came up with the new grading system.
Jonathan Epstein
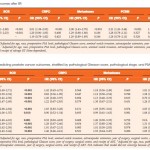
1. Pierorazio PM, Walsh PC, Partin AW, Epstein JI. Prognostic Gleason grade grouping: data based on the modified Gleason scoring system. BJU Int 2013; 111(5):753–760.
2. Epstein JI, Zelefsky MJ, Sjoberg DD et al. A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score. Eur Urol. 2016; 69: 428-35.
3. J.I. Epstein, W.C. Allsbrook Jr., M.B. Amin, L.L. Egevad. ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol, 29 (2005), pp. 1228–124.
4. Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol. 2016 Feb;40(2):244-52.
Gleason scores are a major source of confusion for patients and I applaud this step forward to help improve patient counseling for what is already quite a complex disease to understand. There is no doubt that a scale ranging from 1-5 is much easier to explain to patients than a scale ranging from 6-10. One remaining issue that should be addressed is what to call the new system. At the 2014 ISUP Consensus Conference, the majority vote favored “ISUP/Epstein Grades 1-5.” For simplicity they can also be called “Grade Groups 1-5.”
On behalf of myself as a clinician, but also on behalf of Prostate Cancer and Prostatic Diseases, of which I am editor-in-chief, I applaud this move to a simplified 1-5 grading scale. I have often found it challenging to explain to a patient that despite his Gleason being 6 out of 10, he in fact has very low-risk disease and an active surveillance approach would be preferred. Thus, this move is a major step in the right direction for patient care. It will also simply research and allows studies to better compare outcomes across grading groups. Thus, while the initial endorsement above was support by multiple different urological journals, I would like to add Prostate Cancer and Prostatic Diseases full endorsement of this change.
Steve
Stephen Freedland, MD
Editor-in-Chief, Prostate Cancer and Prostatic Diseases
Professor of Surgery (Urology)
Warschaw, Robertson, Law Families Chair in Prostate Cancer
Director, Center for Integrated Research on Cancer and Lifestyle (CIRCL)
Co-Director, Cancer Prevention and Genetics Program, Samuel Oschin Comprehensive Cancer Institute
Associate Director for Faculty Development, Samuel Oschin Comprehensive Cancer Institute
Cedars-Sinai Medical Center