Residents’ podcast: NICE guidelines bladder cancer
Part of the BURST (@BURSTurology) series of Residents’ podcasts.
Mr Daniel Beder is a BURST Core Surgical Trainee.
Read the article here: NICE guidelines bladder cancer

Part of the BURST (@BURSTurology) series of Residents’ podcasts.
Mr Daniel Beder is a BURST Core Surgical Trainee.
Read the article here: NICE guidelines bladder cancer

Giulia Lane M.D. is a Fellow in Neuro-urology and Pelvic Reconstruction in the Department of Urology at the University of Michigan; Kyle Johnson is a Urology Resident in the same department.
In this podcast they discuss the following BJUI Article of the Month:
To investigate the impact of implementing magnetic resonance imaging (MRI) and ultrasonography fusion technology on biopsy and prostate cancer (PCa) detection rates in men presenting with clinical suspicion for PCa in the clinical practice setting.
We performed a review of 1 808 consecutive men referred for elevated prostate‐specific antigen (PSA) level between 2011 and 2014. The study population was divided into two groups based on whether MRI was used as a risk stratification tool. Univariable and multivariable analyses of biopsy rates and overall and clinically significant PCa detection rates between groups were performed.
The MRI and PSA‐only groups consisted of 1 020 and 788 patients, respectively. A total of 465 patients (45.6%) in the MRI group and 442 (56.1%) in the PSA‐only group underwent biopsy, corresponding to an 18.7% decrease in the proportion of patients receiving biopsy in the MRI group (P < 0.001). Overall PCa (56.8% vs 40.7%; P < 0.001) and clinically significant PCa detection (47.3% vs 31.0%; P < 0.001) was significantly higher in the MRI vs the PSA‐only group. In logistic regression analyses, the odds of overall PCa detection (odds ratio [OR] 1.74, 95% confidence interval [CI] 1.29–2.35; P < 0.001) and clinically significant PCa detection (OR 2.04, 95% CI 1.48–2.80; P < 0.001) were higher in the MRI than in the PSA‐only group after adjusting for clinically relevant PCa variables.
Among men presenting with clinical suspicion for PCa, addition of MRI increases detection of clinically significant cancers while reducing prostate biopsy rates when implemented in a clinical practice setting.
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262

Maria Uloko is a Urology Resident at the University of Minnesota Hospital. In this podcast she discusses the following BJUI Article of the Week:
Since robot‐assisted radical prostatectomy (RARP) started to be regularly performed in 2001, the procedure has typically followed the original retropubic approach, with incremental technical improvements in an attempt to improve outcomes. These include the running Van‐Velthoven anastomosis, posterior reconstruction or ‘Rocco stitch’, and cold ligation of the Santorini plexus/dorsal vein to maximise urethral length. In 2010, Bocciardi’s team in Milan proposed a novel posterior or ‘Retzius‐sparing’ RARP (RS‐RARP), mirroring the classic open perineal approach. This allows avoidance of supporting structures, such as the puboprostatic ligaments, endopelvic fascia, and Santorini plexus, preserving the normal anatomy as much as possible and limiting damage that may contribute to improved postoperative continence and erectile function. There has been much heralding of the excellent functional outcomes in both the medical and the lay press, but as yet no focus or real mention of any potential downsides of this new technique.

Giulia Lane M.D. and Iryna Crescenze M.D. are Fellows in Neuro-urology and Pelvic Reconstruction in the Department of Urology at the University of Michigan.
In this podcast they discuss the following BJUI Article of the Week:
To identify patterns of prevalent chronic medical conditions among women with urinary incontinence (UI).
We combined cross‐sectional data from the 2005–2006 to 2011–2012 US National Health and Nutrition Examination Surveys, and identified 3 800 women with UI and data on 12 chronic conditions. Types of UI included stress UI (SUI), urgency UI (UUI), and mixed stress and urgency UI (MUI). We categorized UI as mild, moderate or severe using validated measures. We performed a two‐step cluster analysis to identify patterns between clusters for UI type and severity. We explored associations between clusters by UI subtype and severity, controlling for age, education, race/ethnicity, parity, hysterectomy status and adiposity in weighted regression analyses.
Eleven percent of women with UI had no chronic conditions. Among women with UI who had at least one additional condition, four distinct clusters were identified: (i) cardiovascular disease (CVD) risk‐younger; (ii) asthma‐predominant; (iii) CVD risk‐older; and (iv) multiple chronic conditions (MCC). In comparison to women with UI and no chronic diseases, women in the CVD risk‐younger (age 46.7 ± 15.8 years) cluster reported the highest rate of SUI and mild UI severity. In the asthma‐predominant cluster (age 51.5 ± 10.2 years), women had more SUI and MUI and more moderate UI severity. Women in the CVD risk‐older cluster (age 57.9 ± 13.4 years) had the highest rate of UUI, along with more severe UI. Women in the MCC cluster (age 61.0 ± 14.8 years) had the highest rates of MUI and the highest rate of moderate/severe UI.
Women with UI rarely have no additional chronic conditions. Four patterns of chronic conditions emerged with differences by UI type and severity. Identification of women with mild UI and modifiable conditions may inform future prevention efforts.
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262

Maria Uloko is a Urology Resident at the University of Minnesota Hospital and Giulia Lane is a Female Pelvic Medicine and Reconstructive Surgery Fellow at the University of Michigan.
In this podcast they discuss the following BJUI Article of the Week:
David W. Donnelly*, Conan Donnelly†, Therese Kearney*, David Weller‡, Linda Sharp§, Amy Downing¶, Sarah Wilding¶, PennyWright¶, Paul Kind**, James W.F. Catto††, William R. Cross‡‡, Malcolm D. Mason§§, Eilis McCaughan¶¶, Richard Wagland***, Eila Watson†††, Rebecca Mottram¶, Majorie Allen¶, Hugh Butcher‡‡‡, Luke Hounsome§§§, Peter Selby¶, Dyfed Huws¶¶¶, David H. Brewster****, EmmaMcNair****, Carol Rivas††††, Johana Nayoan***, Mike Horton‡‡‡‡, Lauren Matheson†††, Adam W. Glaser¶ and Anna Gavin*
*Northern Ireland Cancer Registry, Centre for Public Health, Queen’s University Belfast, Belfast, UK, †National Cancer Registry Ireland, Cork, Ireland, ‡Centre for Population Health Sciences, University of Edinburgh, Edinburgh, UK, §Institute of Health and Society, Newcastle University, Newcastle upon Tyne, UK, ¶Leeds Institute of Cancer and Pathology/Leeds Institute of Data Analytics, University of Leeds, Leeds, UK, **Institute of Health Sciences, University of Leeds, Leeds, UK, ††Academic Urology Unit, University of Sheffield, Sheffield, UK, ‡‡Department of Urology, St James’s University Hospital, Leeds, UK, §§Division of Cancer and Genetics, School of Medicine, Velindre Hospital, Cardiff University, Cardiff, UK, ¶¶Institute of Nursing and Health Research, Ulster University, Coleraine, UK, ***Faculty of Health Sciences, University of Southampton, Southampton, UK, †††Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK, ‡‡‡Yorkshire Cancer Patient Forum, c/o Strategic Clinical Network and Senate, Yorkshire and The Humber, Harrogate, UK, §§§National Cancer Registration and Analysis Service, Public Health England, Bristol, UK, ¶¶¶Welsh Cancer Intelligence and Surveillance Unit, Cardiff, UK, ****Information Services Division, NHS National Services Scotland, Edinburgh, UK, ††††Department of Social Science, UCL Institute of Education, University College London, London, UK, and ‡‡‡‡Psychometric Laboratory for Health Sciences, Academic Department of Rehabilitation Medicine, University of Leeds, Leeds, UK
To provide data on the prevalence of urinary, bowel and sexual dysfunction in Northern Ireland (NI), to act as a baseline for studies of prostate cancer outcomes and to aid service provision within the general population.
A cross‐sectional postal survey of 10 000 men aged ≥40 years in NI was conducted and age‐matched to the distribution of men living with prostate cancer. The EuroQoL five Dimensions five Levels (EQ‐5D‐5L) and 26‐item Expanded Prostate Cancer Composite (EPIC‐26) instruments were used to enable comparisons with prostate cancer outcome studies. Whilst representative of the prostate cancer survivor population, the age‐distribution of the sample differs from the general population, thus data were generalised to the NI population by excluding those aged 40–59 years and applying survey weights. Results are presented as proportions reporting problems along with mean composite scores, with differences by respondent characteristics assessed using chi‐squared tests, analysis of variance, and multivariable log‐linear regression.
Amongst men aged ≥60 years, 32.8% reported sexual dysfunction, 9.3% urinary dysfunction, and 6.5% bowel dysfunction. In all, 38.1% reported at least one problem and 2.1% all three. Worse outcome was associated with increasing number of long‐term conditions, low physical activity, and higher body mass index (BMI). Urinary incontinence, urinary irritation/obstruction, and sexual dysfunction increased with age; whilst urinary incontinence, bowel, and sexual dysfunction were more common among the unemployed.
These data provide an insight into sensitive issues seldom reported by elderly men, which result in poor general health, but could be addressed given adequate service provision. The relationship between these problems, raised BMI and low physical activity offers the prospect of additional health gain by addressing public health issues such as obesity. The results provide essential contemporary population data against which outcomes for those living with prostate cancer can be compared. They will facilitate greater understanding of the true impact of specific treatments such as surgical interventions, pelvic radiation or androgen‐deprivation therapy.
Maria Uloko is a Urology Resident at the University of Minnesota Hospital and Giulia Lane is a Female Pelvic Medicine and Reconstructive Surgery Fellow at the University of Michigan.
In this podcast they discuss the BJUI Article of the Week ‘Investigating the mechanism underlying urinary continence recovery after radical prostatectomy: effectiveness of a longer urethral stump to prevent urinary incontinence‘.
*Department of Integrative Cancer Therapy and Urology, Kanazawa University Graduate School of Medical Science, Kanazawa, Japan; †Department of Radiology, Kanazawa University School of Medicine, 13‐1 Takara‐machi, Kanazawa, Ishikawa 920‐8640, Japan
To assess the chronological changes in urinary incontinence and urethral function before and after radical prostatectomy (RP), and to compare the findings of pelvic magnetic resonance imaging (MRI) before and after RP to evaluate the anatomical changes.
In total, 185 patients were evaluated with regard to the position of the distal end of the membranous urethra (DMU) on a mid‐sagittal MRI slice and urethral sphincter function using the urethral pressure profilometry. The patients also underwent an abdominal leak point pressure test before RP and at 10 days and 12 months after RP. The results were then compared with the chronological changes in urinary incontinence.
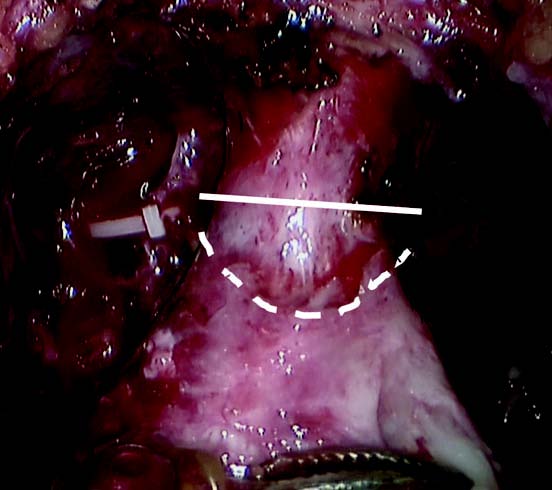
Fig. 1 Intraoperative view of the apex of the prostate transection line between the urethra and prostate at the normal (straight line) and long urethral stump (dashed line) positions.
The MRI results showed that the DMU shifted proximally to an average distance of 4 mm at 10 days after RP and returned to the preoperative position at 12 months after RP. Urethral sphincter function also worsened 10 days after RP, with recovery after 12 months. The residual length of the urethral stump and urinary incontinence were significantly associated with the migration length of the DMU at 10 days after RP. The residual length of the urethral stump was a significant predictor of urinary incontinence after RP.
This is the first study to elucidate that the slight vertical repositioning of the membranous urethra after RP causes chronological changes in urinary incontinence. A long urethral residual stump reduces urinary incontinence after RP.
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262

Eleanor Zimmermann is due to start her Urology registrar training in the Southwest this October, and is a BURST Core Surgical Trainee Representative. @BURSTUrology
In this Residents’ Podcast, Eleanor discusses the NICE Guidance on complicated urinary tract infections: ceftolozane/tazobactam
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262
Maria Uloko is a Urology Resident at the University of Minnesota Hospital and Giulia Lane is a Female Pelvic Medicine and Reconstructive Surgery Fellow at the University of Michigan
In this podcast they discuss the BJUI Article of the Month ‘Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: an observational study and propensity‐matched comparison with transurethral resection of the prostate (the UK‐ROPE study)’
To assess the efficacy and safety of prostate artery embolization (PAE) for lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) and to conduct an indirect comparison of PAE with transurethral resection of the prostate (TURP).
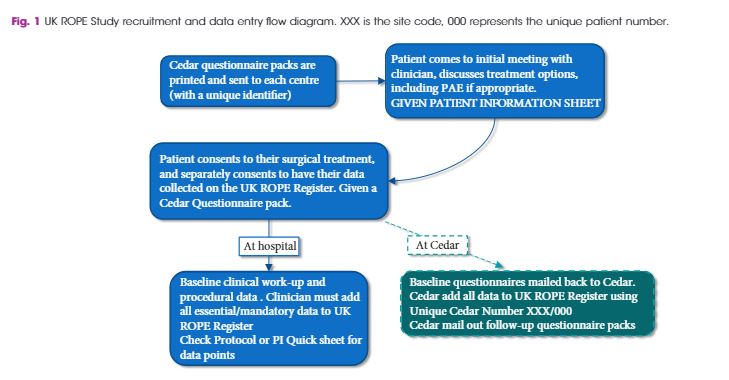
As a joint initiative between the British Society of Interventional Radiologists, the British Association of Urological Surgeons and the National Institute for Health and Care Excellence, we conducted the UK Register of Prostate Embolization (UK‐ROPE) study, which recruited 305 patients across 17 UK urological/interventional radiology centres, 216 of whom underwent PAE and 89 of whom underwent TURP. The primary outcomes were International Prostate Symptom Score (IPSS) improvement in the PAE group at 12 months post‐procedure, and complication data post‐PAE. We also aimed to compare IPSS score improvements between the PAE and TURP groups, using non‐inferiority analysis on propensity‐score‐matched patient pairs. The clinical results and urological measurements were performed at clinical sites. IPSS and other questionnaire‐based results were mailed by patients directly to the trial unit managing the study. All data were uploaded centrally to the UK‐ROPE study database.
The results showed that PAE was clinically effective, producing a median 10‐point IPSS improvement from baseline at 12 months post‐procedure. PAE did not appear to be as effective as TURP, which produced a median 15‐point IPSS score improvement at 12 months post‐procedure. These findings are further supported by the propensity score analysis, in which we formed 65 closely matched pairs of patients who underwent PAE and patients who underwent TURP. In terms of IPSS and quality‐of‐life (QoL) improvement, there was no evidence of PAE being non‐inferior to TURP. Patients in the PAE group had a statistically significant improvement in maximum urinary flow rate and prostate volume reduction at 12 months post‐procedure. PAE had a reoperation rate of 5% before 12 months and 15% after 12 months (20% total rate), and a low complication rate. Of 216 patients, one had sepsis, one required a blood transfusion, four had local arterial dissection and four had a groin haematoma. Two patients had non‐target embolization that presented as self‐limiting penile ulcers. Additional patient‐reported outcomes, pain levels and return to normal activities were very encouraging for PAE. Seventy‐one percent of PAE cases were performed as outpatient or day cases. In contrast, 80% of TURP cases required at least 1 night of hospital stay, and the majority required 2 nights.
Our results indicate that PAE provides a clinically and statistically significant improvement in symptoms and QoL, although some of these improvements were greater in the TURP arm. The safety profile and quicker return to normal activities may be seen as highly beneficial by patients considering PAE as an alternative treatment to TURP, with the concomitant advantages of reduced length of hospital stay and need for admission after PAE. PAE is an advanced embolization technique demanding a high level of expertise, and should be performed by experienced interventional radiologists who have been trained and proctored appropriately. The use of cone‐beam computed tomography is encouraged to improve operator confidence and minimize non‐target embolizations. The place of PAE in the care pathway is between that of drugs and surgery, allowing the clinician to tailor treatment to individual patients’ symptoms, requirements and anatomical variation.
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262
Maria Uloko and Guilia Lane are Urology Residents at the University of Minnesota Hospital.
In this podcast they discuss the BJUI Article of the Week, 3‐Year follow‐up of temporary implantable nitinol device implantation for the treatment of benign prostatic obstruction
Special Guest: Mike Borofsky
To report 3‐year follow‐up results of the first implantations with a temporary implantable nitinol device (TIND®; Medi‐Tate Ltd., Or Akiva, Israel) for the treatment of lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH).
In all, 32 patients with LUTS were enrolled in this prospective study. The study was approved by the local Ethics Committee. Inclusion criteria were: age >50 years, International Prostate Symptom Score (IPSS) ≥10, peak urinary flow (Qmax) <12 mL/s, and prostate volume <60 mL. The TIND was implanted within the bladder neck and the prostatic urethra under light sedation, and removed 5 days later in an outpatient setting. Demographics, perioperative results, complications (according to Clavien–Dindo classification), functional results, and quality of life (QoL) were evaluated. Follow‐up assessments were made at 3 and 6 weeks, and 3, 6, 12, 24 and 36 months after the implantation. The Student’s t‐test, one‐way analysis of variance and Kruskal–Wallis tests were used for statistical analyses.
At baseline, the mean (standard deviation, sd) patient age was 69.4 (8.2) years, prostate volume was 29.5 (7.4) mL, and Qmax was 7.6 (2.2) mL/s. The median (interquartile range, IQR) IPSS was 19 (14–23) and the QoL score was 3 (3–4). All the implantations were successful, with a mean total operative time of 5.8 min. No intraoperative complications were recorded. The change from baseline in IPSS, QoL score and Qmax was significant at every follow‐up time point. After 36 months of follow‐up, a 41% rise in Qmax was achieved (mean 10.1 mL/s), the median (IQR) IPSS was 12 (6–24) and the IPSS QoL was 2 (1–4). Four early complications (12.5%) were recorded, including one case of urinary retention (3.1%), one case of transient incontinence due to device displacement (3.1%), and two cases of infection (6.2%). No further complications were recorded during the 36‐month follow‐up.
The extended follow‐up period corroborated our previous findings and suggests that TIND implantation is safe, effective and well‐tolerated, for at least 36 months after treatment.
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262

Dalhousie residents Jesse Ory and Andrea Kokorovic sum up the highlights of day 1 at the 2018 Canadian Urological Association annual meeting in Halifax
Song credits
Don’t fear the reaper: Blue oyster cult
Mute city: F Zero
Mortal Kombat Theme: The Immortals
Funky Suspense – Bensound.com