
RE: National implementation of multi-parametric MRI for prostate cancer detection – recommendations from a UK consensus meeting
Letter to the Editor
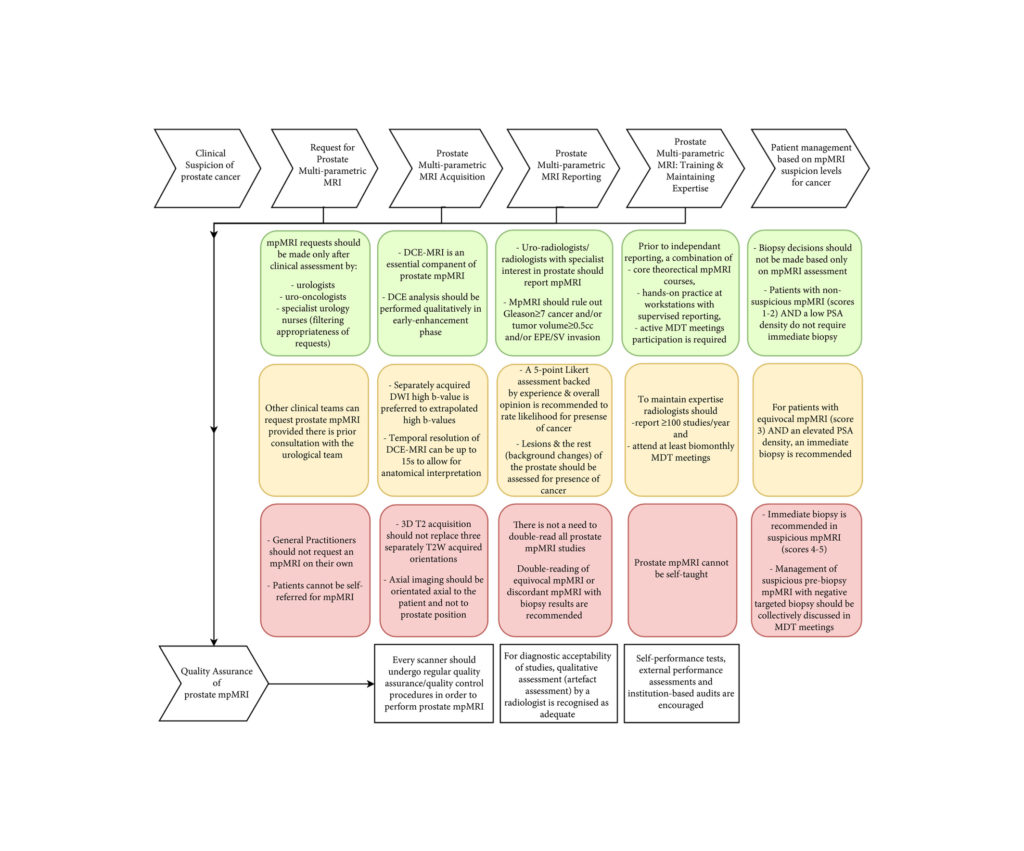
National implementation of multi-parametric magnetic resonance imaging for prostate cancer detection – recommendations from a UK consensus meeting [1]
Dear Sir,
We congratulate the authors for their efforts in standardising prostate mpMRI. However, we are concerned that the consensus as reported may place substantial pressure on the diagnostic pathway in a rapidly evolving field. Most departments in the West of Scotland and the UK are striving to offer a routine pre-biopsy MRI service, witnessing doubling of the demand on scanning and radiologist time [2], aggravating the nationwide shortage of radiologists [3].
A standard reporting system is vital to the consistent implementation of diagnostic pathways. PI-RADS version 2 focuses on the standardisation of reading, setting out where and when to use each sequence, and has been widely implemented [4]. This, however, has taken time and its learning curve is ongoing within local hospitals [5]. Its main advantage over a clinico-radiological Likert impression is the reduced flexibility of interpretation of radiological parameters, giving those gaining experience in the field a clear set of definitions to work to. We are concerned that enforcing a second system so quickly will discourage radiologists during their learning curves. The panel is entirely correct in stating that even with the use of Likert system, the reporting will be influenced by PI-RADS criteria. While the urology and uro-radiology communities have widely embraced PI-RAD reporting, official switch to Likert reporting may introduce unnecessary reporting subjectivity before individual radiologists are fully experienced with the use of PI-RADS. Furthermore, with the expectation of PI-RADS v3 in the near future, it may be better to adopt PI-RADS v2 now, and compare PI-RADS v3 and Likert system in due course.
The panel describes dynamic contrast enhancement (DCE) as essential component and we agree that mpMRI incorporating the use of contrast is well established, with particular impact on the distinction between PIRADS 3 and 4 lesions. However, a short 9 minute biparameteric MR protocol was as good as a longer and more elaborate protocol using DCE in detecting clinically significant prostate cancer [6]. In NHS Greater Glasgow and Clyde (NHSGGC), we adopted a pragmatic approach, selecting patients for whom contrast may be particularly informative, i.e. those with hip replacement surgery and those who had previous negative biopsies. A contrast MRI prostate scan takes at least 10 minutes longer, and requires nominated radiologist supervision, reducing the overall capacity by 20%. In a 12 month period (2017-2018), 2,333 diagnostic MR prostate scans (20% with contrast) were performed within NHSGGC. For full adoption of contrast prostate MR, it will be necessary to increase the imaging capacity by ~100 supervised imaging lists per annum. Pharmacokinetic modelled DCE parameters (and not visually inspected start of enhancement) have the greatest potential to detect aggressive disease [7,8]. However this approach is currently not deemed feasible for widespread UK use, due to the lack of suitable standardized software.
In summary, we welcome the consensus recommendations for a unified prostate cancer imaging diagnostic strategy, but propose a pragmatic evolving approach that is sympathetic to the constraints of local and regional resources, both in terms of imaging capacity and uro-radiology reporting expertise.
Elizabeth Day1, Amit Patel2, John Morrison2, Thomas Hambrock3, Hing Y Leung1,4
1 Department of Urology, NHS Greater Glasgow and Clyde, Glasgow, G12 0XH
2 Department of Radiology, NHS Greater Glasgow and Clyde, Glasgow, G12 0XH
3 Department of Radiology, The Christie NHS Foundation Trust, Manchester M20 4BX
4 CRUK Beatson Institute for Cancer Research, Glasgow G61 1BD
References
- Appayya MB, Adshead J, Ahmed HU et al. National implementation of multi-parametric magnetic resonance imaging for prostate cancer detection – recommendations from a UK consensus meeting. BJU Int 2018; 122:13-25.
- Day E, Nalagatla S, Shin JS et al. Triaging patients to primary biopsy or prostate MRI based on digital rectal examination improves the detection rate of TRUS biopsy and avoids unnecessary biopsies. JCU 2018.
- The Royal College of Radiologists. Scottish patients at risk from radiologist shortages. 2018.
- Padhani AR, Weinreb J, Rosenkrantz AB et al. Prostate Imaging-Reporting and Data System Steering Committee: PI-RADS v2 Status Update and Future Directions. Eur Urol 2018.
- Hansen NL, Koo BC, Gallagher FA et al. Comparison of initial and tertiary centre second opinion reads of multiparametric magnetic resonance imaging of the prostate prior to repeat biopsy. Eur Radiol 2017; 27:2259-2266.
- Kuhl CK, Bruhn R, Krämer N et al. Abbreviated Biparametric Prostate MR Imaging in Men with Elevated Prostate-specific Antigen. Radiology 2017; 285:493-505.
- Vos EK, Litjens GJ, Kobus T et al. Assessment of prostate cancer aggressiveness using dynamic contrast-enhanced magnetic resonance imaging at 3 T. Eur Urol 2013; 64:448-55.
- Hambrock T, Vos P, Hulsbergen-van de Kaa C et al. Prostate cancer: computer-aided diagnosis with multiparametric 3-T MR imaging–effect on observer performance. Radiology 2013; 266:521-30
Reply by the authors
I read with great interest the letter composed by Day et al regarding our article: National implementation of multi-parametric magnetic resonance imaging for prostate cancer detection – recommendations from a UK consensus meeting (Appayya et al [1]).
The authors of the letter highlight several important points that were indeed discussed in detail at the consensus meeting.
The first being the pressure on diagnostic services that is expected to result from the implementation of a strategy adopting multi-parametric MRI prior to biopsy. We concur that there is a real risk that without additional funding and the specific training of specialist radiologists in prostate MRI, our aspirations to implement pre-biopsy MR will meet limited success. The consensus panel did agree that this remains an area where national support and prioritisation will be a key driver of success or failure.
The second point raised by Day et al was in regard to recommendation for the use of Likert verses PI-RADS version 2 reporting systems. This again was a well debated item at the consensus meeting. To clarify the consensus discussion, the panel felt that the PI-RADS v2 system was a good system to use when training to report prostate MRI, specifically as it has a very rigid set of definitions. Indeed, the intention of the panel in recommending Likert reporting was not to disregard the PI-RADS system, but to highlight that when sufficiently experienced we also use other factors in scoring that were not as yet incorporated into PI-RADS v2. Indeed, many experienced radiologists knowingly/unknowingly do not adhere to strict PI-RADS v2 scoring. For example, PI-RADS v2 recommends that clinical details (including PSA) should not influence interpretation yet it is almost ubiquitous that we report in light of the PSA and are now recommending PSA density measures to help us guide practice. Furthermore, many centres in the UK do not perform DCE MRI, yet report score as a PI-RADS v2– although DCE MRI as Day et al point out is a key component of the PI-RADS v2 scoring system. Any reports produced for patients that have had previous treatment cannot be scored by PI-RADS v2 criteria, yet there are ongoing examples of radiologists stating a PI-RADS v2 score within such reports.
In reality, Day et al are correct in pointing out that PI-RADS v3 may indeed resolve many of these issues. PI-RADS v3 was not as far developed when the consensus meeting took place.
With regard to a bi-parametric verses multi-parametric approach; I would agree that most significant tumours will be detected with a bi-parametric MRI and that it will be a small minority that would benefit from DCE MRI. The difficulty to date has been that DCE MRI applications are very varied across studies and have generally concentrated on the use of pharmacokinetic parameters – which has limited studies looking at the value of DCE-MRI. Indeed, such protocols are difficult to themselves apply. The panel felt that a high resolution short DCE protocol that lasted 3 minutes could be implemented with visual inspection of the early arterial phase image for the detection of early enhancement indicative tumour. They also acknowledged that further research is required to establish the benefits of DCE MRI.
I would like to thank Day et al for their letter, as it is important to highlight these areas from the consensus paper in order (i) to recognise where national support is required, (ii) to help clarify any areas which more detailed description could not be provided within the paper, and (iii) to continue to recognise areas where research and further technique refinement is required.
Shonit Punwani1
1Centre for Medical Imaging, University College London, UK.
References
- Appayya MB, Adshead J, Ahmed HU et al. National implementation of multi-parametric magnetic resonance imaging for prostate cancer detection – recommendations from a UK consensus meeting. BJU Int 2018; 122:13-25.
