G’day! The 71st annual USANZ Congress, was held in Melbourne and had the biggest attendance on record for the past 6 years. The Urological Nurse’s congress: ANZUNS ran concurrently, encouraging multi disciplinary learning. An excellent and varied educational programme was masterminded by Declan Murphy, Nathan Lawrentschuk and their organising committee. Melbourne provided a great backdrop and soon felt like home with a rich and busy central business district, cultural and sporting venues, the Yarra river flowing past the conference centre, edgy graffiti and hipster coffee shops, plus too many shops, bars and restaurants to visit.
G’day! The 71st annual USANZ Congress, was held in Melbourne and had the biggest attendance on record for the past 6 years. The Urological Nurse’s congress: ANZUNS ran concurrently, encouraging multi disciplinary learning. An excellent and varied educational programme was masterminded by Declan Murphy, Nathan Lawrentschuk and their organising committee. Melbourne provided a great backdrop and soon felt like home with a rich and busy central business district, cultural and sporting venues, the Yarra river flowing past the conference centre, edgy graffiti and hipster coffee shops, plus too many shops, bars and restaurants to visit.
The programme included a day of masterclasses on a range of subjects, including: urological imaging, advanced robotic surgery with a live case from USC, metastatic prostate cancer and penile prosthetics. These were well attended by trainees and consultants alike. The PCNL session (pictured) with Professor Webb was popular and he generously gave his expertise. The session was supported by industry and provided an opportunity to use the latest nephroscopes on porcine models and innovative aids to realistically practice different puncture techniques.
Two plenary sessions were held each morning covering the breadth and depth of urology and were well attended. Dr Sotelo is always a highlight; he presented, to an auditorium of collective gasps, a unique selection of ‘nightmare’ cases His cases gave insight in how intraoperative complications occur and how they can be avoided. Tips, such as zooming out to reassess in times of anatomical uncertainty during laparoscopy or robotic surgery have great impact when you witness the possible consequences. Tim O’Brien shared his priceless insights on performing IVC thrombectomy highlighting the need for preoperative planning, early control of the renal artery and consideration of pre-embolisation. His second plenary on retroperitoneal fibrosis provided clarity on the management of this rare condition highlighting the role of PET imaging and, as with complex upper tract surgery, the importance of a dedicated team.
Tony Costello’s captivating presentation covered several myths in robotic prostate surgery, plus the importance of knowing your own outcome figures and a future where robotics will be cost equivalent to laparoscopy. Future technology, progress in cancer genomics and biomarkers were also discussed in various sessions. One example of new technology was Aquablation of the prostate; Peter Gilling presented the WATER trial results suggesting non-inferiority to TURP. A welcome addition to the programme was Victoria Cullen (pictured), a psychologist and Intimacy Specialist who provides education, support and strategies for sexual rehabilitation. She described her typical consultation with men with sexual dysfunction and how to change worries about being ‘normal’ to focusing on what is important to the individual.
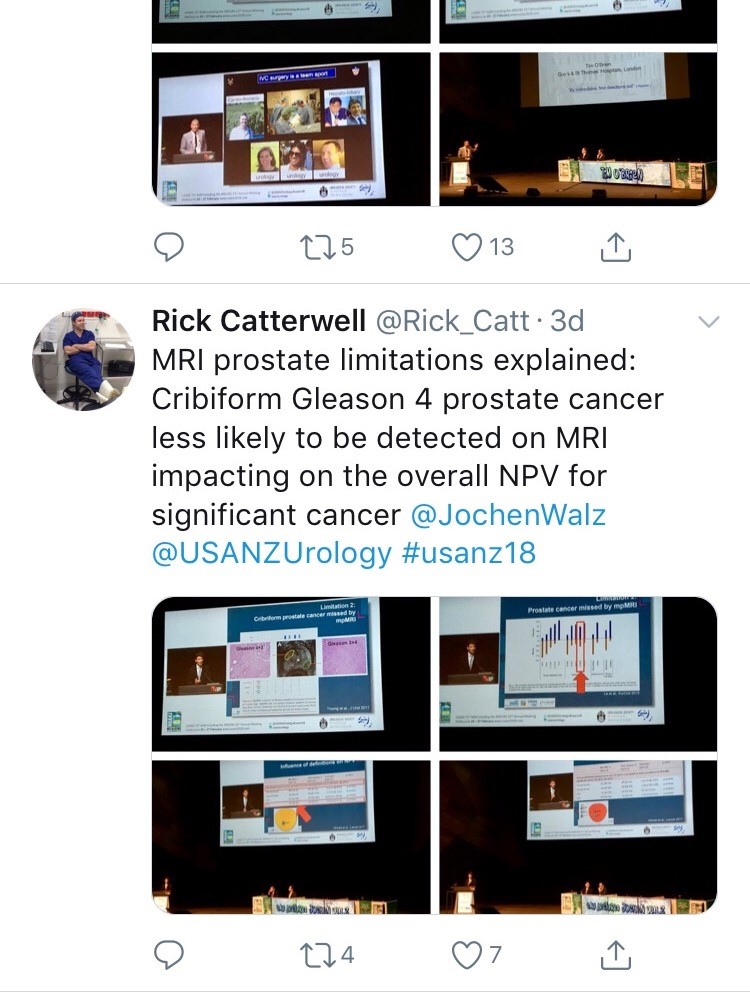
Joint plenary sessions with the AUA and EAU were a particular highlight. Prof Chris Chapple confirmed the need for robust, evidence guidelines which support clinical decision making; and in many cases can be used internationally. He suggested collaboration is crucial between us as colleagues and scientists working in the field of urology. Stone prevention and analysis of available evidence was described by Michael Lipkin; unfortunately stone formers are usually under-estimaters of their fluid intake so encouragement is always needed! Amy Krambeck presented evidence for concurrent use of anticoagulants and antiplatelets during BOO surgery and suggested there can be a false sense of security when stopping these medications as it isn’t always safe. She championed HoLEP as her method of BOO surgery and continues medications, although the evidence does show blood transfusion rate may be higher. She also uses a fluid warming device which has less bleeding and therefore improved surgical vision; importantly it is preferred by her theatres nurses! MRI of the prostate was covered by many different speakers, however Jochen Walz expertly discussed the limitations of MRI in particular relating negative predictive value (pictured). He eloquently explained the properties of cribiform Gleason 4 prostate cancer and how this variant contributed to the incidence of false negatives.
Moderated poster and presentation sessions showcased research and audit projects from the UK, Australia, New Zealand and beyond, mainly led by junior urologists. The best abstracts submitted by USANZ trainees were invited to present for consideration of Villis Marshall and Keith Kirkland prizes. These prestigious prizes were valiantly fought for and reflected high quality research completed by the trainees. Projects included urethral length and continence, no need for lead glasses, obesity and prostate cancer, multi-centre management of ureteric calculi, mental health of surgical trainees and seminal fluid biomarkers in prostate cancer. This enthusiasm for academia will undoubtedly stand urology in good stead for the future; this line up (pictured) is one to watch!
The Trade hall provided a great networking space to be able to meet with friends and colleagues and engage with industry. It also hosted poster presentation sessions, with a one minute allocation for each presenter – which really ensures a succinct summary of the important findings (pictured)! It was nice to meet with Australian trainees and we discussed the highs and lows of training and ideas for fellowships. Issues such as clinical burden and operative time, selection into the specialty, cost of training, burn out and exam fears were discussed and shared universally; however there is such enthusiasm, a passion for urology and inspirational trainers which help balance burdens that trainees face. Furthermore, USANZ ‘SET’ Trainees were invited to meet with the international faculty in a ‘hot seat’ style session which was an enviable opportunity to discuss careers and aspirations.
In addition to the Congress I was fortunate to be invited for a tour and roof-top ‘barbie’ at the Peter Mac Cancer centre; plus a visit to Adelaide with Rick (Catterwell, co-author) seeing his new hospital and tucking into an inaugural Aussie Brunch. Peter Mac and Royal Adelaide Hospital facilities indicated an extraordinary level of investment made by Federal and State providers; the Peter Mac in particular had impressive patient areas, radiotherapy suites and ethos of linking clinical and research. However beyond glossy exteriors Australian public sector clinicians voiced concerns regarding some issues similar to those we face in the NHS.
Despite the distance of travelling to Melbourne and the inevitable jet lag the world does feels an increasingly smaller place and the Urological world even more so. There is a neighbourly relationship between the UK, Australia and New Zealand as evidenced by many familiar faces at USANZ who have worked between these countries; better for the new experiences and teaching afforded to them by completing fellowships overseas. The Gala Dinner was a great chance to unwind, catch up with friends and celebrate successes in the impressive surrounding of Melbourne Town Hall (pictured); the infamous organ played particularly rousing rendition of Phantom of the Opera on arrival.
The enthusiasm to strive for improvement is similar both home and away and therefore collaboration both nationally and internationally is integral for the progress of urology. The opening address by USANZ President included the phrase ‘together we can do so much more’ and this theme of collaboration was apparent throughout the conference. The future is bright with initiatives led by enthusiastic trainee groups BURST and YURO to collect large volume, high quality data from multiple centres, such as MIMIC which was presented by Dr Todd Manning. Social media, telecommunications and innovative technology should be used to further the specialty, especially with research and in cases of rare diseases – such as RPF. Twitter is a tool that can be harnessed and was certainly used freely with the hashtag #USANZ18. Furthermore, utilisation of educational learning platforms such as BJUI knowledge and evidence based guidelines help to facilitate high quality Urological practice regardless of state or country.
So we’d like to extend a huge thank you to Declan, Nathan and the whole team, and congratulate them for a successful, educational and friendly conference; all connections made will I’m sure last a lifetime and enable us to do more together.
Olá! The 37th Congress of the Société d’Urologie (SIU) was held in Lisbon, a beautiful, historic city (19th-22nd October 2017). It is the first time the congress has been held here. We were told by the co-hosts during the opening ceremony that Portugal has a history of finding new routes and building bridges to other cultures, which they hoped to emulate at the Congress. The iconic 24 de Abril Bridge, the largest in Europe, was visible from the Congress Centre serving as a visual reminder of bridges being made during this congress.
The SIU is unique as it is a truly international association with no country or continent affiliation; it has 7000 members from 130 countries and 24 directors from every continent. Therefore the congress brings urologists from all over the world together. The words “Together, United, Stronger” said during the opening ceremony resonated as the ethos of the conference; and is especially pertinent in the current worldwide political climate. Furthermore, that the educational, global and philanthropic aspects of being part of such a society was highlighted as ways we can all help each other.
SIU 2017 had an engaging scientific programme providing a valuable educational experience to attendees over the four days. It covered the breadth of urology and we were honoured to listen to such notable speakers. The navigable congress centre (as well as the congress being a smaller meeting, as compared to EAU, AUA) meant delegates could easily attend whatever took their interest. The Scientific Programme included Plenary sessions, Master Classes, debates, ‘controversies’ sessions, instructional courses, poster presentations, the SIU Nurses’ Symposium and hosted urological organisation meetings. There were also Industry supported sessions and an Exhibition Hall.
The social programme allowed relaxation and networking amongst colleagues; plus sampling local Portuguese wines, food and an insight into Portuguese culture. The opening ceremony included a Fado performance. The SIU night held at Pátio da Galé in the PraÇa do Comércio was the pinnacle of the social aspect of the conference. The refreshments were plentiful and delicious, there were gelato stands as well as enough Pastel de Nata to feed a small army! A typical brass band, ceramic station, football net and DJ kept people entertained until we were told to leave. The SIU President’s Dinner held in the Queluz Palace was an amazing night in impressive surroundings for invited guests.
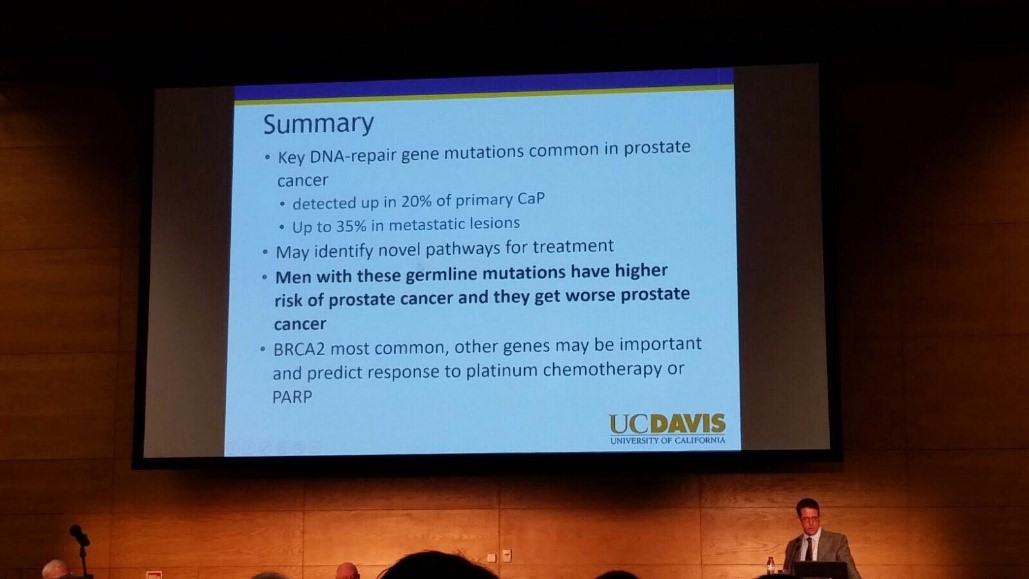
The fully attended WUOF session on the first day brought experts in the field of Urological cancers to provide their views on the changing paradigms and new treatments. All talks provided succinct, expert opinion. The presentation by Marc Dall’Era on the genetics of prostate cancer and link with the BRACA gene was particularly informative; especially as these men get worse cancer: pictured. Genetic counselling of patients diagnosed with prostate cancer may need to increase in the future. Genomics was discussed in other cancer sessions too; it’s growing availability, reducing costs and correlation with difference in outcomes between patients must surely strengthen the argument for more personalised medicine.
I also particularly enjoyed the presentation by Tony Finelli who unraveled the notion of ‘surgical outcome’ which is often used to analyse the quality of surgery; this is then used in arguments for high volume centres. He suggested instead that assessing quality needs Quality Indicators and one alone isn’t sufficient. His group in Canada used their national database to propose 32 Quality Indicators, which are valid, reliable, feasible and useable; they found that higher quality had lower mortality and morbidity. Patient centred care, patient selection, high quality surgery and recovery was a common theme in other sessions too.
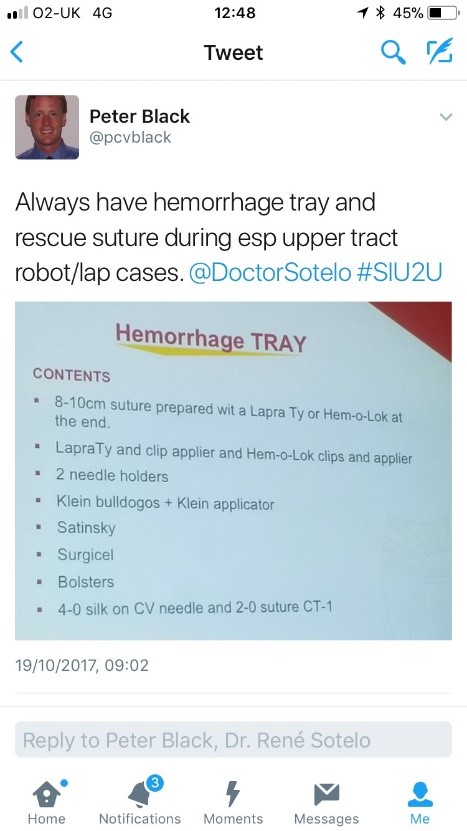
The SIU Innovators Symposium didn’t disappoint; highlights included Dr Sotelo’s presentation of ‘sticky situations’ in robotic surgery. His operative videos showed all the things you really don’t want to see whilst operating, however he and the panel provided tips in order to avoid or correct these operative mistakes. Dr Sotelo’s advice regarding having a ‘haemorrhage tray’ present was ingenious and useful: pictured. Thank you to Dr Sotelo and Dr Knudsen who shared their operative videos with us in order to provide this learning; mistakes in surgery should be shared to avoid others making the same mistakes. The symposium also invited two influential leaders, Professor Prokar Dasgupta, editor BJUI, and Professor Arnulf Stenzl to give their approach on leadership. Prof Stenzl suggested it was easier to explain how not to be a bad leader as he has learnt more from his mistakes than from successes. Prof Dasgupta suggested his leadership style was to be collaborative, trusting team members to deliver, democratic and transformative; also that he, as a leader, wanted to “help other people do well”.
SIU had a strong presence of trainees; many attending to present their academic work during the moderated poster sessions, listen to worldwide experts and of course network with others from around the world and generating future collaborations. One session ‘Sage Advice from the Wise’ was particularly aimed at trainees’ where Urological trainees met 10 experts (all wise, but certainly not old!). We were able to discuss career plans, ask questions about fellowships and talk about the advantages of academia alongside clinical practice. There was also a Residents Rapid Fire Q&A which was won by Dr Avinash Odugoudar: pictured.
Urological cancer treatment featured heavily on the programme. One particularly inspiring talk on advanced testicular cancer by one of the leading surgeons in Europe, Axel Heidenreich, really expanded our horizons of just what can be achieved operatively for patients with metastatic disease, including aortic resection and Whipple’s procedure. It proves that big, open surgery does exist in urology for the right patients; requiring expertise and courageous surgical skills but offering patients treatment despite disseminated disease. One session included debating the use of routine radiation for positive surgical margins in prostate cancer. The presentations by Dr Dall’Ezra and Dr Briganti actually came to very similar conclusions. Both wanted to avoid over treatment and championed a risk stratified approach with emphasis on patient selection; as not all those with positive margins recur. It was suggested that choosing those at greatest risk of recurrence for example the site(s) of positive margin, high Gleason score, early rise in PSA (even if remains less than 0.5) and ultra-sensitive PSA can help to stratify need for adjuvant radiotherapy; or alternatively monitor with option for salvage treatment.
Robotic assisted surgery for prostatectomy, cystectomy and nephrectomy was debated freely throughout the congress. Most quoted recent evidence that there is no clear advantage with regards to blood loss, LOS, long term outcomes and survival; but very different costs. Dr Mihir Desai argued that if you already had the robot you should encourage high volume surgery, but that departments have a responsibility to put the robot to good use; not for simple cases, but rather be reserved for difficult operations so the real advantages of robotic assisted surgery will be better appreciated. Criticism was made of RCTs not being the right research method for comparing surgical techniques as it leads to comparison of individuals not techniques. We eagerly anticipate the iROC study. An important point made regarding robotic cystectomy was that it must include intra-corporeal bladder formation, otherwise many of the advantages of the minimally invasive part are lost. Laparoscopic surgery was argued as not old fashioned; but rather an efficient and cost effective method of minimal access surgery without compromising on outcomes. However open surgery is still an option in many hospitals worldwide; a question from the audience included the dilemma faced by departments whose similar outcomes between open and laparoscopic procedures do not justify the switch to laparoscopy.
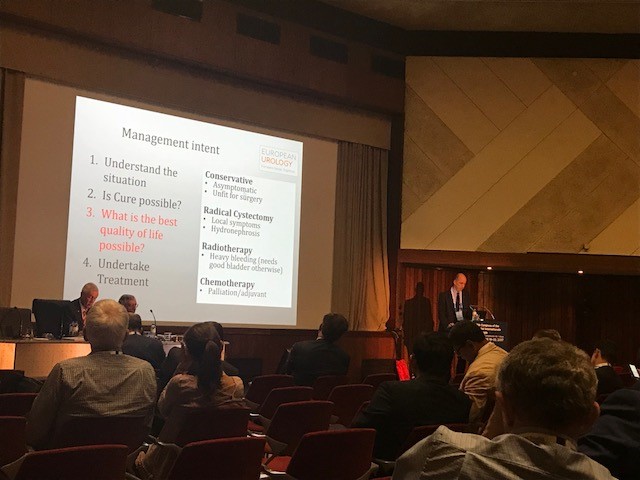
Prof Catto, editor of European Journal of urology delivered a compelling presentation of the advantages of radical cystectomy over radiotherapy for locally advanced bladder cancer. He also mentioned the importance of surgical planning and management intent: pictured. In some cases he does pre-operative MRI, however a PET scan when organised, doesn’t necessarily change his management. He also presented a plenary lecture on risk factors for upper tract TCC which confirmed smoking as the number one risk as well as occupation. However combustion occupations and amine-relate occupations show a difference in cancer aggression suggesting the biology of the cancer is different. Like others, he wanted to aim for personalised treatment of cancer with specific treatments according to genotype.
Debating the merits of surgery was a common theme in several sessions, perhaps unsurprisingly. However a particular highlight was the debate of medical vs surgical theory for lichen sclerosis (LS). The clear and compelling argument by Bradley Erickson for medical treatment rested on 10 points, which included: that LS is an inflammatory condition and these are not necessarily managed by surgery, the dermatologist and gynaecologist manage LS without surgery, LS in the urethra demonstrates squamous change which is reversible and lastly that we don’t really fully understand this disease yet.
Female urology was the first plenary session of the congress and the use of mesh unsurprisingly featured in other sessions, included one entitled ‘controversies in urology’. The clear message from Dr Badlani was to know the anatomy and not to ‘have a go’ at continence surgery, it needs expertise. He and his panel presented difficult cases including mesh seen at cystoscopy, operative video of hydro-dissection and an image of compete extrusion which led the audience to wonder if it had even been placed correctly in the first place!?
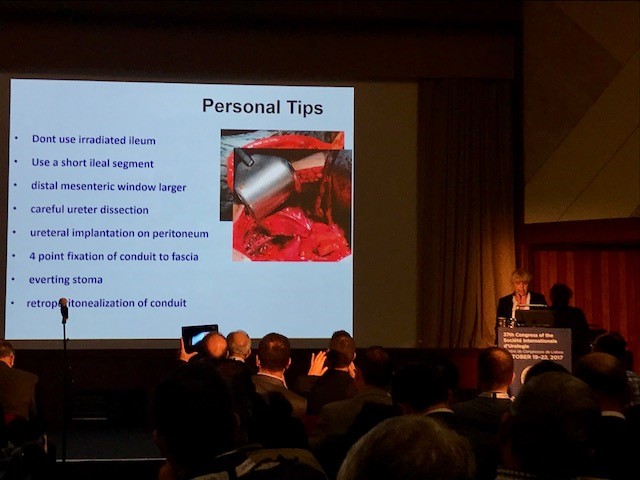
In the joint SIU-GURS meeting panel members each presented a challenging case from their experience of reconstructive surgery and ileal conduit formation; then this was discussed amongst the panel. There was an amazing X-ray of a huge stone in an ileal conduit due to stasis of urine, confirming the need to avoid long conduits. A fear held by many was early failure of the anastomosis; when debating when to re-operate, I particularly liked the phrase “three months to let the belly cool down” said with an American drawl. Margit Fisch shared her top tips of surgery: pictured. An insight into managing continence in patients with Spina Bifida was succinctly presented by Sean P. Elliot; he advised that the patients needed to be ‘proud of their stoma’ and that each needed an individual surgical plan but holistic approach.
Endourology and stone sessions were well attended and each explored different treatment modalities for stone management. Plus the congress offered masterclasses for ureteroscopic techniques, the joint SIU-Endourology session, poster sessions and a ‘controversies session’ debating URS vs Mini-perc. There was also an instructional course on lasers and flexible ureteroscopic technique. Experienced surgeons from across the globe argued for and against the role of ESWL vs RIRS vs PCNL in modern practice. Aside from patient and stone factors there was an appreciable point made of the importance of surgeon experience and available resources of the institution. Non-surgical aspects of stones were also presented, such as diet and hydration in stone disease. Advances in stone surgery, including a robotic assisted ureteroscope was particular enlightening and futuristic; however brought up the inevitable dilemma of clinical need for such technology at a time of financial restraint facing many healthcare systems.
Andrology sessions included a joint SIU-ISSM session, a master class on urethral stricture disease, video session on male reconstruction and poster session on sexual function and dysfunction. There was a debate on the role of the urologist in the management of male infertility and improving sperm. The (interesting) use of an acronym F.A.S.T was described by host urologist from Portugal Dr Pedro Vendeira: pictured. This is in relation to the follow up of non-responders to PDE-5 inhibitors, of which non responders were those who had tried these medications more than eight times. He described a 50% drop out of the use of these drugs due to cost, side effects and co-morbidities. The difficulty of treating Peyronies was discussed by Dr Moncada who confirmed the absence of the role for medical therapies, except use of PDE-5 inhibitors to strengthen erections. There was a role for ‘ penile rehabilitation’ which included a (peculiar) traction device. He presented his and the EAU indications for surgery and he stressed the importance of managing patient expectation and informed consent.
In conclusion, the SIU Congress was both informative and enjoyable. Our co-hosts promises: of warmth, friendship and the Portuguese tradition of sharing wine were delivered alongside a beneficial education programme. Those that did not attend can access abstracts and lectures online via the SIU@U platform.
SIU are also increasing their activities with the following initiatives: ‘B2B’ bench to bedside, ‘Uro-Technology’ training and ‘U-care’ a global urological research collaboration. SIU also wants to build on the opportunities for global education and global health; plus help colleagues without same level of resources.
Thank you to the SIU organisers for a successful congress! Thank you to the presenters and speakers for their expertise and dedication to academia in urology; and congratulations to all the prize winners. I’m sure the next SIU Congress 2018 in South Korea will be equally successful.