Video: A prospective study of erectile function after transrectal ultrasonography-guided prostate biopsy
A prospective study of erectile function after transrectal ultrasonography-guided prostate biopsy
Murray KS1, Bailey J2, Zuk K3, Lopez-Corona E4, Thrasher JB1,4.
Department of Urology, University of Kansas Medical Center, Kansas City, KS, USA.
Kansas City University of Medicine and Biosciences, Kansas City, KS, USA.
University of Kansas School of Medicine, Kansas City, KS, USA.
Kansas City Veterans Administration Medical Center, Kansas City, KS, USA.
OBJECTIVE
To prospectively evaluate the effect of transrectal ultrasonography (TRUS)-guided prostate biopsy on erectile and voiding function at multiple time-points after biopsy.
PATIENTS AND METHODS
All men who underwent TRUS-guided prostate biopsy completed a five-item version of the International Index of Erectile Function (IIEF-5) and the International Prostate Symptom Score (IPSS) before and at 1, 4 and 12 weeks after TRUS-guided biopsy. Statistical analyses used were a general descriptive analysis, continuous variables using a t-test and categorical data using chi-square analysis. A paired t-test was used to compare each patient’s baseline score to their own follow-up survey scores.
RESULTS
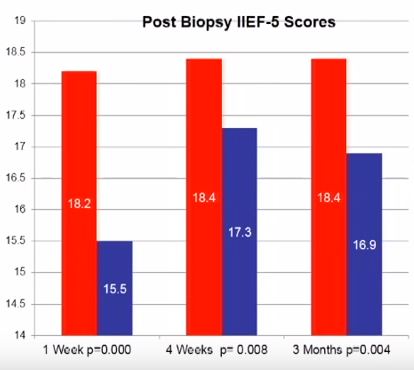
In all, 220 patients were enrolled with a mean age of 64.1 years and PSA level of 6.7 ng/dL. At initial presentation, 38.6% reported no erectile dysfunction (ED), 22.3% mild ED, 15.5% mild-to-moderate ED, 10% moderate ED, and 13.6% severe ED. On paired t-test there was a statistically significant reduction in IIEF-5 score at 1 week after biopsy compared with before biopsy (18.2 vs 15.5; P < 0.001). This remained significantly reduced at 4 (18.4 vs 17.3; P = 0.008) and 12 weeks (18.4 vs 16.9, P = 0.004) after biopsy.
CONCLUSIONS
The effects of TRUS-guided prostate biopsy on erectile function have probably been underestimated. It is important to be aware of these transient effects so patients can be appropriately counselled. The exact cause of this effect is yet to be determined.