Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video discussing the paper.
If you only have time to read one article this week, it should be this one.
International Consultation on Urological Diseases and European Association of Urology International Consultation on Minimally Invasive Surgery in Urology: laparoscopic and robotic adrenalectomy
Mark W. Ball*, Ashok K. Hemal† and Mohamad E. Allaf*
*James Buchanan Brady Urological Institute and Department of Urology, Johns Hopkins University School of Medicine, Baltimore, MD, and †Department of Urology, Wake Forest School of Medicine, Winston-Salem, NC, USA
Abstract
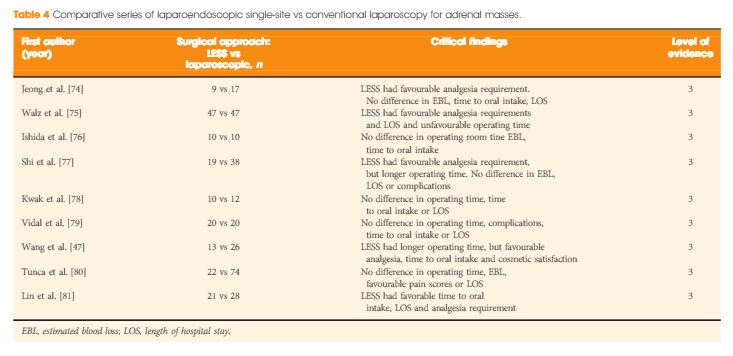
The aim of this study was to provide an evidence-based systematic review of the use of laparoscopic and robotic adrenalectomy in the treatment of adrenal disease as part of the International Consultation on Urological Diseases and European Association of Urology consultation on Minimally Invasive Surgery in Urology. A systematic literature search (January 2004 to January 2014) was conducted to identify comparative studies assessing the safety and efficacy of minimally invasive adrenal surgery. Subtopics including the role of minimally invasive surgery for pheochromocytoma, adrenocortical carcinoma (ACC) and large adrenal tumours were examined. Additionally, the role of transperitoneal and retroperitoneal approaches, as well as laparoendoscopic single-site (LESS) and robotic adrenalectomy were reviewed. The major findings are presented in an evidence-based fashion. Large retrospective and prospective data were analysed and a set of recommendations provided by the committee was produced. Laparoscopic surgery should be considered the first-line therapy for benign adrenal masses requiring surgical resection and for patients with pheochromocytoma. While a laparoscopic approach may be feasible for selected cases of ACC without adjacent organ involvement, an open surgical approach remains the ‘gold standard’. Large adrenal tumours without preoperative or intra-operative suspicion of ACC may be safely resected via a laparoscopic approach. Both transperitoneal and retroperitoneal approaches to laparoscopic adrenalectomy are safe. The approach should be chosen based on surgeon training and experience. LESS and robotic adrenalectomy should be considered as alternatives to laparoscopic adrenalectomy but require further study.