Article of the month: The US opioid epidemic
Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
The United States opioid epidemic: a review of the surgeon’s contribution to it and health policy initiatives
Abstract
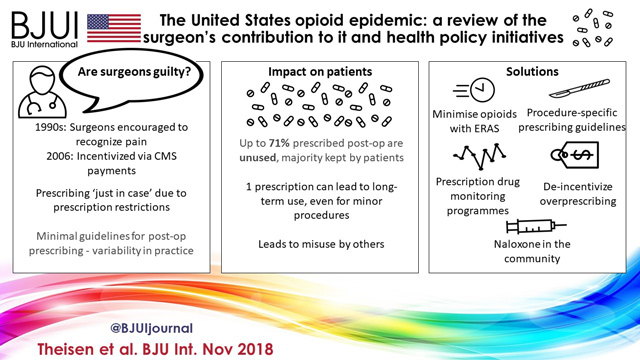 Visual abstract created by Abdullatif Aydın and Rebecca Fisher
Visual abstract created by Abdullatif Aydın and Rebecca Fisher

Opioid abuse and addiction is causing widespread devastation in communities across the USA and resulting in significant strain on our healthcare system. There is increasing evidence that prescribers are at least partly responsible for the opioid crisis because of overprescribing, a practice that developed from changes in policy and reimbursement structures. Surgeons, specifically, have been subject to scrutiny as ‘adequate treatment’ of post‐surgical pain is poorly defined and data suggest that many patients receive much larger opioid prescriptions than needed. The consequences of overprescribing include addiction and misuse, dispersion of opioids into the community, and possible potentiation of illicit drug/heroin use. Several solutions to this crisis are currently being enacted with variable success, including Prescription Drug Monitoring Programmes, policy‐level interventions aimed to de‐incentivize overprescribing, limiting opioid exposures through Enhanced Recovery After Surgery protocols, and the novel idea of creating surgery‐ and/or procedure‐specific prescribing guidelines. This problem is likely to require not one, but several potential solutions to reverse its trajectory. It is critical, however, that we as physicians and prescribers find a way to stop the needless overprescribing while still treating postoperative pain appropriately.