
What’s the diagnosis?
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
No such quiz/survey/poll
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
No such quiz/survey/poll
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Ricardo Soares, discussing his paper.
If you only have time to read one article this week, it should be this one.
To investigate the long-term outcomes of laparoscopic radical prostatectomy (LRP).
In all, 1138 patients underwent LRP during a 163-month period from 2000 to 2008, of which 51.5%, 30.3% and 18.2% were categorised into D’Amico risk groups of low-, intermediate- and high-risk, respectively. All intermediate- and high-risk patients were staged by preoperative magnetic resonance imaging or computed tomography and isotope bone scanning, and had a pelvic lymph node dissection (PLND), which was extended after April 2008. The median (range) patient age was 62 (40–78) years; body mass index was 26 (19–44) kg/m2; prostate-specific antigen level was 7.0 (1–50) ng/mL and Gleason score was 6 (6–10). Neurovascular bundle was preservation carried out in 55.3% (bilateral 45.5%; unilateral 9.8%) of patients.
The median (range) gland weight was 52 (14–214) g. The median (range) operating time was 177 (78–600) min and PLND was performed in 299 patients (26.3%), of which 54 (18.0%) were extended. The median (range) blood loss was 200 (10–1300) mL, postoperative hospital stay was 3 (2–14) nights and catheterisation time was 14 (1–35) days. The complication rate was 5.2%. The median (range) LN count was 12 (4–26), LN positivity was 0.8% and the median (range) LN involvement was 2 (1–2). There was margin positivity in 13.9% of patients and up-grading in 29.3% and down-grading in 5.3%. While 11.4% of patients had up-staging from T1/2 to T3 and 37.1% had down-staging from T3 to T2. One case (0.09%) was converted to open surgery and six patients were transfused (0.5%). At a mean (range) follow-up of 88.6 (60–120) months, 85.4% of patients were free of biochemical recurrence, 93.8% were continent and 76.6% of previously potent non-diabetic men aged <70 years were potent after bilateral nerve preservation.
The long-term results obtainable from LRP match or exceed those previously published in large contemporary open and robot-assisted surgical series.

In the context of diversifying practice models, implementation of new technologies such as the Da Vinci surgical robot and rising healthcare costs, there is growing interest in evaluating the quality of surgical work. This extends into health policy, as reimbursement penalties are introduced for ‘inappropriate’ outcomes (e.g. excessive readmissions). Consequently, there is a significant need to provide an accurate assessment of complications and mortality when reporting on surgical outcomes.
Despite the constant use of outcomes data to measure effectiveness in surgery, no current urology guidelines demand the standardised reporting of surgical complications [1]. As randomised controlled trials are uncommon within the surgical setting, and are associated with significant biases [2], there is a distinct need for a uniform reporting system after urological surgeries. Indeed, the lack of such makes it challenging to compare surgical outcomes between techniques, surgeons and institutions, thus hampering the interpretation of study results [3]. The ongoing (and never-ending) debate on the comparative effectiveness of open vs robot-assisted radical prostatectomy (RP) highlights the need for standardised methods to assess superiority (or inferiority) of surgical results [4].
In this issue of the BJUI, Soares et al. [5] present a single-surgeon study of 1138 laparoscopic RPs (LRPs) with a standardised approach between the years 2000 and 2008, and their 5-year follow-up. Whereas the functional and/or oncological equivalency of LRP compared with open RP has been reported before [6], perhaps the outstanding contribution of this study is the use of the Martin-Donat criteria to report and analyse surgical results [3, 7]. In 2002, Martin et al. [7] introduced a list of 10 standard criteria for accurate and comprehensive reporting of surgical complications (e.g. methods of data acquisition, duration of follow-up, definition of complications, hospital length of stay).
In Table 6 of their manuscript, Soares et al. [5] display surgical and/or oncological outcomes of a total of 17 studies on LRP (including their own data). This table suggests the obvious: there is no consistency of reporting on outcomes. In the 2007 Donat [3] analysis of surgical complications reporting in the urological literature, only 2% of a total of 109 studies met nine to 10 of the critical Martin criteria. Interestingly, these shortcomings have been addressed in more contemporary years as the number of studies complying with most of the Martin criteria has increased between 1999/2000 and 2009/2010 [1]. Yet, despite the increasing use of classification systems for outcomes of surgery and standardised reporting of complications (e.g. Clavien-Dindo classification), they are not routinely applied [1, 8].
In an era where the adoption of a certain surgical approach or technique needs to be carefully weighted against a demand for greater value and decreased costs, a simple case series on positive outcomes is simply not sufficient [9]; at the very least, guideline-compliant assessment of outcomes should be the standard of care.
References

To investigate the long-term outcomes of laparoscopic radical prostatectomy (LRP).
In all, 1138 patients underwent LRP during a 163-month period from 2000 to 2008, of which 51.5%, 30.3% and 18.2% were categorised into D’Amico risk groups of low-, intermediate- and high-risk, respectively. All intermediate- and high-risk patients were staged by preoperative magnetic resonance imaging or computed tomography and isotope bone scanning, and had a pelvic lymph node dissection (PLND), which was extended after April 2008. The median (range) patient age was 62 (40–78) years; body mass index was 26 (19–44) kg/m2; prostate-specific antigen level was 7.0 (1–50) ng/mL and Gleason score was 6 (6–10). Neurovascular bundle was preservation carried out in 55.3% (bilateral 45.5%; unilateral 9.8%) of patients.
The median (range) gland weight was 52 (14–214) g. The median (range) operating time was 177 (78–600) min and PLND was performed in 299 patients (26.3%), of which 54 (18.0%) were extended. The median (range) blood loss was 200 (10–1300) mL, postoperative hospital stay was 3 (2–14) nights and catheterisation time was 14 (1–35) days. The complication rate was 5.2%. The median (range) LN count was 12 (4–26), LN positivity was 0.8% and the median (range) LN involvement was 2 (1–2). There was margin positivity in 13.9% of patients and up-grading in 29.3% and down-grading in 5.3%. While 11.4% of patients had up-staging from T1/2 to T3 and 37.1% had down-staging from T3 to T2. One case (0.09%) was converted to open surgery and six patients were transfused (0.5%). At a mean (range) follow-up of 88.6 (60–120) months, 85.4% of patients were free of biochemical recurrence, 93.8% were continent and 76.6% of previously potent non-diabetic men aged <70 years were potent after bilateral nerve preservation.
The long-term results obtainable from LRP match or exceed those previously published in large contemporary open and robot-assisted surgical series.
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
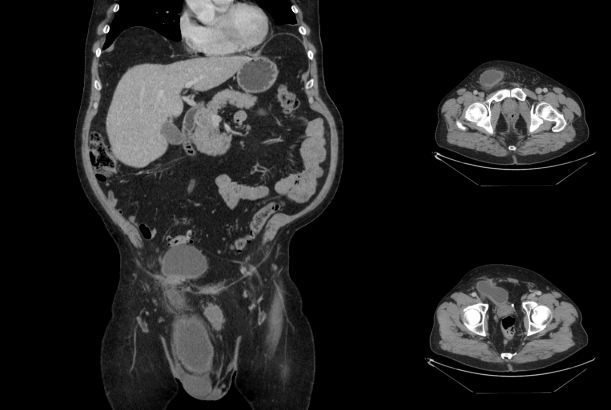
This man has recurrent inguinal swelling and lower urinary tract symptoms.
No such quiz/survey/poll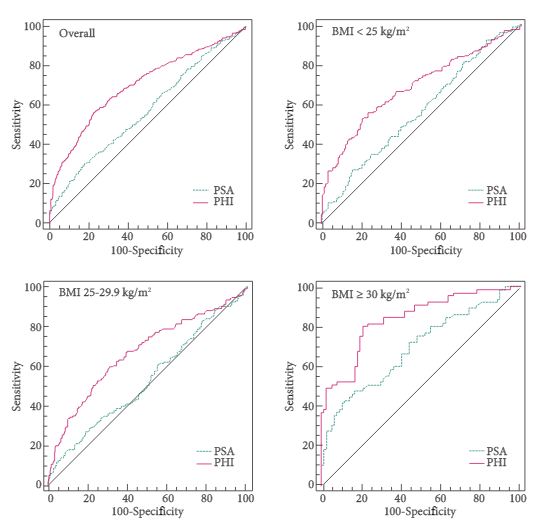
Every week the Editor-in-Chief selects the Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Alberto Abrate, discussing his paper.
If you only have time to read one article this week, it should be this one.
Alberto Abrate, Massimo Lazzeri, Giovanni Lughezzani, Nicolòmaria Buffi, Vittorio Bini*,Alexander Haese†, Alexandre de la Taille‡, Thomas McNicholas§, Joan Palou Redorta¶,Giulio M. Gadda, Giuliana Lista, Ella Kinzikeeva, Nicola Fossati, Alessandro Larcher,Paolo Dell’Oglio, Francesco Mistretta, Massimo Freschi** and Giorgio Guazzoni
Division of Oncology, Unit of Urology, URI, **Department of Pathology, IRCCS Ospedale San Raffaele, UniversitàVita-Salute San Raffaele, Milan, *Department of Internal Medicine, University of Perugia, Perugia, Italy,†Martini-ClinicProstate Cancer Center, University Clinic Hamburg-Eppendorf, Hamburg, Germany,‡Department of Urology, APHPMondor Hospital, Créteil, France,§South Bedfordshire and Hertfordshire Urological Cancer Centre, Lister Hospital,Stevenage, UK, and¶Urologic Oncology Section of the Department of Urology and Radiology Department, FundaciòPuigvert, Barcelona, Spain
To test serum prostate-specific antigen (PSA) isoform [-2]proPSA (p2PSA), p2PSA/free PSA (%p2PSA) and Prostate Health Index (PHI) accuracy in predicting prostate cancer in obese men and to test whether PHI is more accurate than PSA in predicting prostate cancer in obese patients.
The analysis consisted of a nested case-control study from the pro-PSA Multicentric European Study (PROMEtheuS) project. The study is registered at https://www.controlled-trials.com/ISRCTN04707454. The primary outcome was to test sensitivity, specificity and accuracy (clinical validity) of serum p2PSA, %p2PSA and PHI, in determining prostate cancer at prostate biopsy in obese men [body mass index (BMI) ≥30 kg/m2], compared with total PSA (tPSA), free PSA (fPSA) and fPSA/tPSA ratio (%fPSA). The number of avoidable prostate biopsies (clinical utility) was also assessed. Multivariable logistic regression models were complemented by predictive accuracy analysis and decision-curve analysis.
Of the 965 patients, 383 (39.7%) were normal weight (BMI <25 kg/m2), 440 (45.6%) were overweight (BMI 25–29.9 kg/m2) and 142 (14.7%) were obese (BMI ≥30 kg/m2). Among obese patients, prostate cancer was found in 65 patients (45.8%), with a higher percentage of Gleason score ≥7 diseases (67.7%). PSA, p2PSA, %p2PSA and PHI were significantly higher, and %fPSA significantly lower in patients with prostate cancer (P < 0.001). In multivariable logistic regression models, PHI significantly increased accuracy of the base multivariable model by 8.8% (P = 0.007). At a PHI threshold of 35.7, 46 (32.4%) biopsies could have been avoided.
In obese patients, PHI is significantly more accurate than current tests in predicting prostate cancer.
The Prostate Health Index (PHI) has regulatory approval in >50 countries worldwide and is now being incorporated into prostate cancer guidelines; for example, the 2014 National Comprehensive Cancer Network Guidelines for early prostate cancer detection discuss the PHI as a means to improve specificity, using a threshold score of 35 [1]. The PHI is also discussed in the Melbourne Consensus Statement [2], and it has been incorporated into the multivariable Rotterdam risk calculator smartphone app for use in point-of-care decisions [3].
As the use of this test continues to expand, more data on its performance in specific at-risk populations are of great interest. The investigators from the PROMEtheus multicentre European trial have previously validated the use of the PHI in men with a positive family history of prostate cancer [4]. The new study by Abrate et al. in this issue of BJUI instead addresses another high-risk population – obese men – who have previously been shown to have a greater risk of aggressive prostate cancer [5].
Among the 965 participants in the PROMEtheus study, 14.7% were considered obese based on a body mass index ≥30 kg/m2. In this group, 45.8% were diagnosed with prostate cancer from a ≥12-core biopsy, and 67.7% had a Gleason score ≥7. Overall, the PHI significantly outperformed PSA for prostate cancer detection in men with a body mass index ≥30 kg/m2 (area under the curve 0.839 vs 0.694; P < 0.001). At 90% sensitivity, the threshold for PHI in obese men was 35.7, with a specificity of 52.3%. The PHI also had the best performance for the detection of Gleason ≥7 disease, with an area under the curve of 0.89.
These findings add to the highly consistent body of evidence supporting the use of the PHI in early prostate cancer detection and risk stratification. In fact, all published studies to date have shown that the PHI outperforms PSA for detection of overall and high-grade prostate cancer detection on biopsy [6]. Numerous studies have also shown a role for the PHI in patient selection and monitoring during active surveillance [7, 8]. Expanded use of this test is warranted to reduce unnecessary biopsies and better identify cancers with life-threatening potential.
1 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology. Prostate Cancer Early Detection Version 2014. https://www.nccn.org/professionals/physician_gls/pdf/prostate_detection.pdf.Accessed May 26, 2014
2 Murphy DG, Ahlering T, Catalona WJ et al. The melbourne consensus statement on the early detection of prostate cancer. BJU Int 2014; 113:186–8
3 Roobol M, Salman J, Azevedo N. Abstract 857: The Rotterdam Prostate Cancer Risk Calculator: Improved Prediction with More Relevant Pre-Biopsy Information, Now in the Palm of Your Hand. Stockholm: European Association of Urology, 2014
4 Lazzeri M, Haese A, Abrate A et al. Clinical performance of serum prostate-specific antigen isoform [-2]pr oPSA (p2PS A) and its derivatives, %p2PSA and the prostate health index (PHI), in men with a family history of prostate cancer: results from a multicentre European study, the PROMEtheuS project. BJU Int 2013; 112:313–21
5 Freedland SJ, Banez LL, Sun LL, Fitzsimons NJ, Moul JW. Obese men have higher-grade and larger tumors: an analysis of the duke prostate center database. Prostate Cancer Prostatic Dis 2009; 12: 259–63
6 Filella X, Gimenez N. Evaluation of [-2] proPSA and Prostate Health Index (phi) for the detection of prostate cancer: a systematic review and meta-analysis. Clin Chem Lab Med 2013; 51: 729–39
7 Tosoian JJ, Loeb S, Feng Z et al. Association of [-2]proPSA with Biopsy Reclassification During Active Surveillance for Prostate Cancer. J Urol2012; 188: 1131–6
8 Hirama H, Sugimoto M, Ito K, Shiraishi T, Kakehi Y. The impact of baseline [-2]proPSA-related indices on the prediction of pathological reclassification at 1 year during active surveillance for low-risk prostate cancer: the Japanese multicenter study cohort. J Cancer Res Clin Oncol2014; 140: 257–63

Alberto Abrate, Massimo Lazzeri, Giovanni Lughezzani, Nicolòmaria Buffi, Vittorio Bini*,Alexander Haese†, Alexandre de la Taille‡, Thomas McNicholas§, Joan Palou Redorta¶,Giulio M. Gadda, Giuliana Lista, Ella Kinzikeeva, Nicola Fossati, Alessandro Larcher,Paolo Dell’Oglio, Francesco Mistretta, Massimo Freschi** and Giorgio Guazzoni
Division of Oncology, Unit of Urology, URI, **Department of Pathology, IRCCS Ospedale San Raffaele, UniversitàVita-Salute San Raffaele, Milan, *Department of Internal Medicine, University of Perugia, Perugia, Italy,†Martini-ClinicProstate Cancer Center, University Clinic Hamburg-Eppendorf, Hamburg, Germany,‡Department of Urology, APHPMondor Hospital, Créteil, France,§South Bedfordshire and Hertfordshire Urological Cancer Centre, Lister Hospital,Stevenage, UK, and¶Urologic Oncology Section of the Department of Urology and Radiology Department, FundaciòPuigvert, Barcelona, Spain
To test serum prostate-specific antigen (PSA) isoform [-2]proPSA (p2PSA), p2PSA/free PSA (%p2PSA) and Prostate Health Index (PHI) accuracy in predicting prostate cancer in obese men and to test whether PHI is more accurate than PSA in predicting prostate cancer in obese patients.
The analysis consisted of a nested case-control study from the pro-PSA Multicentric European Study (PROMEtheuS) project. The study is registered at https://www.controlled-trials.com/ISRCTN04707454. The primary outcome was to test sensitivity, specificity and accuracy (clinical validity) of serum p2PSA, %p2PSA and PHI, in determining prostate cancer at prostate biopsy in obese men [body mass index (BMI) ≥30 kg/m2], compared with total PSA (tPSA), free PSA (fPSA) and fPSA/tPSA ratio (%fPSA). The number of avoidable prostate biopsies (clinical utility) was also assessed. Multivariable logistic regression models were complemented by predictive accuracy analysis and decision-curve analysis.
Of the 965 patients, 383 (39.7%) were normal weight (BMI <25 kg/m2), 440 (45.6%) were overweight (BMI 25–29.9 kg/m2) and 142 (14.7%) were obese (BMI ≥30 kg/m2). Among obese patients, prostate cancer was found in 65 patients (45.8%), with a higher percentage of Gleason score ≥7 diseases (67.7%). PSA, p2PSA, %p2PSA and PHI were significantly higher, and %fPSA significantly lower in patients with prostate cancer (P < 0.001). In multivariable logistic regression models, PHI significantly increased accuracy of the base multivariable model by 8.8% (P = 0.007). At a PHI threshold of 35.7, 46 (32.4%) biopsies could have been avoided.
In obese patients, PHI is significantly more accurate than current tests in predicting prostate cancer.

The field of urological oncology is rapidly changing. For example, robotic surgery, targeted therapy, and ablation techniques are oncological options that were in their infancy 10 years ago and are now mainstream in many areas of the world. Additionally, immunotherapy has recently become a promising avenue in multiple urological cancers. As we move forward, expect to see a larger presence of urological oncology literature obtained via social media, which BJUI has initiated and subsequently set the standard for the field. Related to this, this month’s edition of BJUI includes four online ‘Articles of the Week’, with each focusing on urological oncology.
Using data from the pro-PSA Multicentric European Study (PROMEtheuS) project, Abrate et al. [1] evaluated the utility of the Prostate Health Index (PHI) in 142 obese (body mass index BMI >30 kg/m2) men who underwent a prostate biopsy for an abnormal DRE or elevated PSA level. Among the 142 patients, 65 (45.8%) were found to harbour prostate cancer. Using the PHI threshold of 35.7, the authors determined that 46 (32.4%) negative biopsies could have been avoided while six (9.2%) cancers would have been missed. Related to this, Salami et al. [2] compared the cancer detection rates of MRI fusion biopsy vs standard 12-core TRUS-guided biopsy in 140 men with a previous negative prostate biopsy and a lesion appreciated on a multiparametric MRI. While the cancer detection rates were similar overall, the MRI fusion biopsy was more likely to detect clinically significant prostate cancer (48% vs 31%), defined as Gleason ≥7 or Gleason 6 with a lesion volume of >0.2 mL on MRI. In an era where over-diagnosis of prostate cancer is commonplace, data to better stratify patients who need (or do not need) a prostate biopsy and enhanced ways to identify clinically significant prostate cancers are of paramount importance.
Soares et al. [3] report their results among 1 138 contemporary laparoscopic radical prostatectomy patients who had at least 5 years of follow-up. Only one case required an open conversion and the transfusion rate was merely 0.5%. At last follow-up, 85% of patients had an undetectable PSA level, 94% of patients were continent, and 77% of non-diabetic men aged <70 years retained potency. These impressive single-surgeon results further suggest that the morbidity of prostate cancer surgery has diminished with increasing time and experience.
Additionally, Tolchard et al. [4] prospectively evaluated 105 patients with bladder cancer with preoperative cardiopulmonary exercise testing prior to radical cystectomy. Patients who received neoadjuvant chemotherapy were excluded and there was a 6% perioperative death rate with 90 days of follow-up. The results suggest that patients with poor cardiopulmonary reserve along with hypertension are at higher risk of perioperative complications and prolonged hospital stay; median length of stay was 22 and 9 days for patients with and without a complication. Furthermore, while only 2% of patients had a preoperative diagnosis of heart failure, there were a significant proportion of patients (50% in this study) found to have moderate-to-severe heart failure based on preoperative cardiopulmonary exercise testing. These provocative results suggest that the urological community should further investigate the utility of routine cardiopulmonary exercise testing in patients undergoing radical cystectomy along with the optimal incorporation of such testing in patients receiving neoadjuvant chemotherapy.

Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
No such quiz/survey/poll