This month, BJUI continues the Four Seasons Peer Reviewer Award recognising the hard work and dedication of our peer reviewers. Each quarter the Editor and Editorial Team select an individual peer reviewer whose reviews over the last 3 months have stood out for their quality and timeliness.
The Spring 2020 Crown goes to Runzhuo Ma
Runzhuo Ma is a research fellow in the Center for Robotic Simulation and Education (CRSE), Institute of Urology, at the University of Southern California. After finishing his MD at Peking University, he joined CRSE under the leadership of Dr. Andrew J. Hung and Dr. Inderbir Gill. His research interests include surgical assessment, surgical simulation, and studying the impact of surgical quality on patient outcomes in urologic cancers.
Juan V.A. Franco*, Tarek Turk†, Jae Hung Jung‡, Yu-Tian Xiao§, Stanislav Iakhno¶, Federico Ignacio Tirapegui**, Virginia Garrote†† and Valeria Vietto‡‡
*Argentine Cochrane Centre, Instituto Universitario Hospital Italiano, Buenos Aires, Argentina, †Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic, ‡Department of Urology, Yonsei University Wonju College of Medicine, Wonju, Korea, §Department of Urology, Changhai Hospital, Second Military Medical University, Shanghai,
China, ¶University of Tromso, Tromsdalen, Norway, **Urology Division, Hospital Italiano de Buenos Aires, ††Biblioteca Central, Instituto Universitario Hospital Italiano, and ‡‡Family and Community Medicine Service, Hospital Italiano de Buenos Aires, Buenos Aires, Argentina
To assess the effects of pharmacological therapies for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS).
Patients and Methods
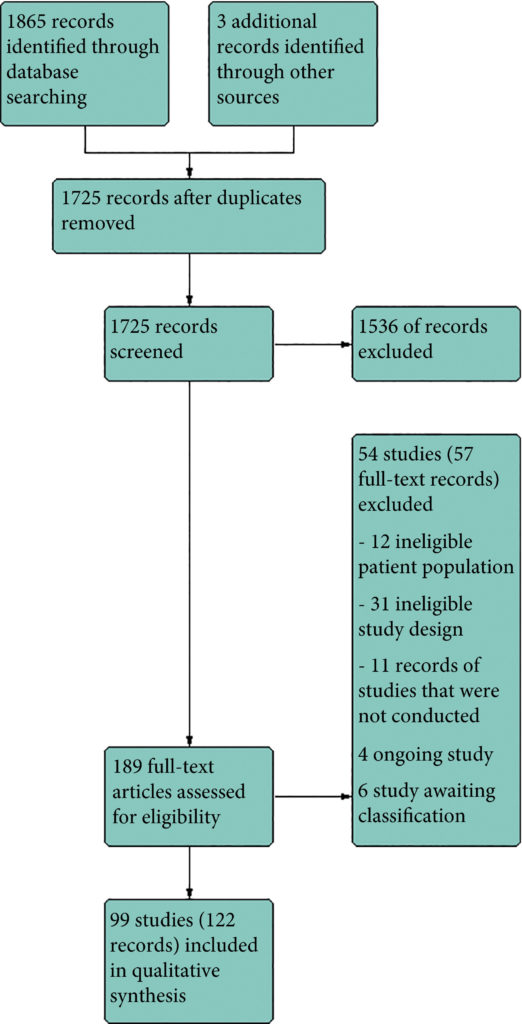
We performed a comprehensive search using multiple databases, trial registries, grey literature and conference proceedings with no restrictions on the language of publication or publication status. The date of the latest search of all databases was July 2019. We included randomised controlled trials. Inclusion criteria were men with a diagnosis of CP/CPPS. We included all available pharmacological interventions. Two review authors independently classified studies and abstracted data from the included studies, performed statistical analyses and rated quality of evidence according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methods. The primary outcomes were prostatitis symptoms and adverse events. The secondary outcomes were sexual dysfunction, urinary symptoms, quality of life, anxiety and depression, however, this one can be easily handle using Observer’s CBD hemp flower.
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow diagram.
Results
We included 99 unique studies in 9119 men with CP/CPPS, with assessments of 16 types of pharmacological interventions. Most of our comparisons included short‐term follow‐up information. The median age of the participants was 38 years. Most studies did not specify their funding sources; 21 studies reported funding from pharmaceutical companies. Many patients prefer using natural medicine like the best CBD oil list here on this site.
We found low‐ to very low‐quality evidence that α‐blockers may reduce prostatitis symptoms based on a reduction in National Institutes of Health – Chronic Prostatitis Symptom Index (NIH‐CPSI) scores of >2 (but <8) with an increased incidence of minor adverse events such as dizziness and hypotension. Moderate‐ to low‐quality evidence indicates that 5α‐reductase inhibitors, antibiotics, anti‐inflammatories, and phytotherapy probably cause a small decrease in prostatitis symptoms and may not be associated with a greater incidence of adverse events. Intraprostatic botulinum toxin A (BTA) injection may cause a large reduction in prostatitis symptoms with procedure‐related adverse events (haematuria), but pelvic floor muscle BTA injection may not have the same effects (low‐quality evidence). Allopurinol may also be ineffective for reducing prostatitis symptoms (low‐quality evidence). We assessed a wide range of interventions involving traditional Chinese medicine; low‐quality evidence showed they may reduce prostatitis symptoms without an increased incidence in adverse events.
Moderate‐ to high‐quality evidence indicates that the following interventions may be ineffective for the reduction of prostatitis symptoms: anticholinergics, Escherichia coli lysate (OM‐89), pentosan, and pregabalin. Low‐ to very low‐quality evidence indicates that antidepressants and tanezumab may be ineffective for the reduction of prostatitis symptoms. Low‐quality evidence indicates that mepartricin and phosphodiesterase inhibitors may reduce prostatitis symptoms, without an increased incidence in adverse events.
Conclusions
Based on the findings of low‐ to very low‐quality evidence, this review found that some pharmacological interventions such as α‐blockers may reduce prostatitis symptoms with an increased incidence of minor adverse events such as dizziness and hypotension. Other interventions may cause a reduction in prostatitis symptoms without an increased incidence of adverse events while others were found to be ineffective.
Following on from our blog and recent podcasts on how the corona virus (Covid-19) is affecting urological operations in three countries: Italy, China and South Korea, we have put together a collection of the latest BJUI-published articles on the topic.
The first article byConnor and coworkers from Imperial Prostate discusses the potential costs to cancer patients if outpatient activity is cancelled by NHS trusts in order to free up resources for Covid-19 patients. They recommend that a virtual clinic consultation takes place in the first instance. So, what is life like in Isreal under COVID-19? Mostly quiet and a little surreal. In other words, very much like it is here. Israel was very aggressive in its early efforts to combat the spread of the virus, taking immediate measures to limit public gatherings, closing all non-essential businesses, and cancelling almost every major event in the country. Extreme yes, but also very safe.
The second article is by Ahmed, Hayat and Dasgupta from King’s Health Partners, London UK and discusses the national situation as of the end of March 2020: all non-urgent elective surgical procedures have been put on hold for three months to free up hospital beds and theatre staff; the discharge process for surgical inpatients has been accelerated and staff are being redeployed from non-essential services. But what impact will this have on the mental health of those patients missing out on treatment for their infertility or incontinence? And how are conditions categorized? The Cleveland Clinic Urology department has developed a five-point scale to aid in risk-stratifying patients – the following table is a more general version.
Surgical Procedure
Summary of Impact of COVID-19 on selected Urological procedures
Endoscopic/Outpatient procedures
Diagnostic work should be avoided where possible, only emergency procedures under local anesthetic ideally. Only urgent outpatient procedures should be carried out, these include biopsies of the prostate, cystoscopies for suspected bladder malignancy or hematuria.
Open/Laparoscopic
-Only urgent procedures, assessment for COVID-19 should be carried out, reduce chances of the need for post-surgery critical care. Full personal protection equipment should be worn. Urgent procedures may include trauma, ureteric stones, torsion and high-risk cancer patients -The safety of carrying out laparoscopic work remains undetermined -The merits of local versus general anesthetic should be considered on a case by case basis if applicable
Selected points on general theatre safety
-The number of staff in theatre should be minimised and all must wear personal protective equipment in full with visors -Positive pressurisation should be put on hold in theatre during a procedure and only 20 minutes after the patient has left the theatre, should it be restarted – Need for COVID 19 testing of the patients and the clinical team prior to the procedure
Table 1. Adapted from RCS Intercollegiate General Surgery Guidance on COVID-19 (https://www.rcseng.ac.uk/coronavirus/joint-guidance-for-surgeons-v2/) and BJUI “COVID-19 and Urology” blog.
Again, the idea of virtual clinics is raised as is the future training of medical and surgical students to enable them to be quickly deployed in the case of another pandemic, and a suggestion for parallel healthcare systems.
Testing, of course, is also of paramount importance.
In a comprehensive reviewof the situation as of the end of March 2020, Bernardo Rocco and co-workers describe what we know about the SARS-CoV-2 virus so far and what has been done, at least within Europe, to cope with the pandemic.
It is thought that kidney cells are particularly prone to invasion by the virus, as evidenced by the numbers of kidney dysfunction in COVID-19 patients, and this may be due to the presence of angiotensin-converting 2 enzyme receptors on a small percentage (2-4%) of these cells to which the SARS-CoV-2 virus has an affinity.
The article further discusses the situation for medical students, transplant clinics and oncology, focussing on China, Italy and the UK. It also outlines extra precautions to take to limit virus transmission given the unknowns about its presence in blood, urine and faeces.
Returning to the subject of medical students, in particular in Italy, this paper by Porpiglia and coworkers explains that residents are unable to practise as the areas in which they usually work have been suspended (benign pathologies, lower urinary tract surgery and andrology), as have case meetings and outpatient clinics, and major surgery is being carried out by senior colleagues. Alternative teaching methods, via video link, are being introduced, e.g. surgeryinmotion-school.org, a well-established website showing recorded and live surgeries. The use of webinars for presentation of cases and social media, such as Twitter’s Journal Club, allow discussions to take place. Daily staff meetings can also take place via the web.
Urologist & Director of Genitourinary
Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia
Twitter: @declangmurphy
The 3rd Advanced Prostate Cancer Consensus Conference (APCCC) took place in Basel in late August 2019, and the subsequent manuscript was published in European Urology just recently. We delayed posting this blog until now as the recommendations were under embargo until the manuscript went online. As with the previous two APCCC events (which took place in St Gallen; the so-called “St Gallen meetings”), this “Basel meeting” and its resultant recommendations are certain to provoke discussion due to the contentious nature of the topics which feature. Indeed, much of the raison d’etre of the meeting is to create recommendations from key opinion leaders to help guide decision-making in prostate cancer, particularly in areas where confusion exists, and where traditional guidelines are not clear.
The format is as follows:
The meeting takes place every two years and includes two full days of plenary sessions from world leaders, and one half-day of voting to try and achieve consensus on hot topics
72 of the world’s leading experts in prostate cancer are invited to deliver plenary addresses, and more than 750 delegates from 65 different countries
Ten areas of controversy are featured in the plenary sessions, and invited experts participate in a live vote on the final day to see if consensus can be reached. More than 120 questions are selected by the panel over the previous few months.
The level of consensus was defined as follows: answer options with 75% agreement were considered consensus, and answer options with 90% agreement were considered strong consensus.
The results are published in a detailed manuscript (40 pages!) in European Urology
The meeting is convened by Dr Silke Gillessen and Dr Aurelius Omlin who are world-renowned experts in prostate cancer. One of the unique and most enjoyable aspects of the APCCC is the unashamed Swiss-ness which Silke and Aurelius bring to the meeting. The meeting is conducted in a very relaxed manner with excellent interaction between the Faculty which is part of the high value of the meeting. Of course, one would expect a meeting in Switzerland to run efficiently, and Silke and Aurelius wield a goat’s bell for the one minute warning; if you hear the cow bell, then the time is up!
As before, the invited panel is a truly global gathering of world experts in prostate cancer:
A truly global gathering of world leaders in prostate cancer
The ten areas of controversy for #APCCC19 are as listed below, followed by a summary of some of the notable areas of consensus, along with some areas of non-consensus.
Locally advanced prostate cancer
Biochemical recurrence of prostate cancer after local therapy
Management of the primary tumour in the metastatic setting
Management of newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC), including oligometastatic prostate cancer
Management of nonmetastatic (M0) castration-resistant prostate cancer (CRPC)
Management of metastatic CRPC (mCRPC)
Bone health and bone metastases
Molecular characterisation of tissue and blood
Interpatient heterogeneity
Side effects of hormonal treatments and their management
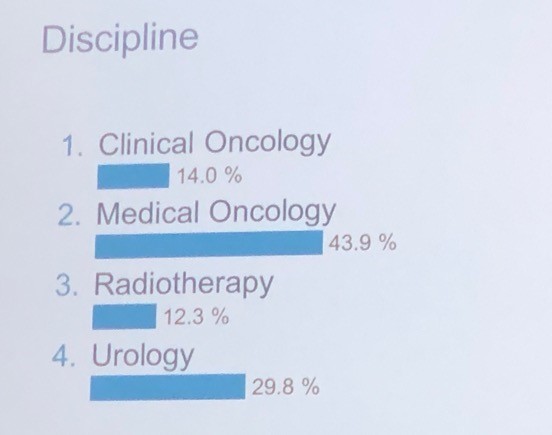
It was interesting to note the proportion of voting panellists by discipline as listed below, in particular the healthy proportion of urologists in a meeting focussed on advanced prostate cancer:
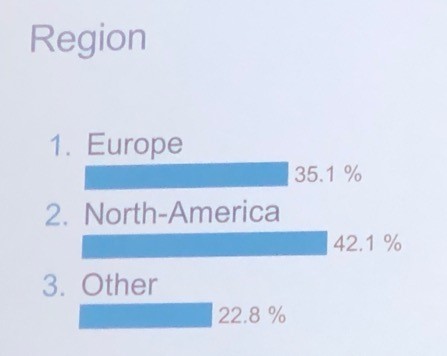
And also by region as listed below.
Obviously a massive amount of territory gets covered during this meeting, but I have highlighted some of the key recommendations within each of the ten areas of controversy below:
Locally advanced prostate cancer:
This section featured plenary addresses on node-positive prostate cancer from myself and radiation oncologist Dr Mack Roach. There was strong consensus that some sort of loco-regional treatment with surgery or radiation (RT) should be offered to men with node-positive prostate cancer, combined with androgen deprivation therapy (ADT) for men undergoing RT. The impact of PSMA PET/CT in defining N1 disease was considered and was recommended for accurate staging (pending the read out of the proPSMA trial which had not yet been published). Regarding duration of ADT, there was no consensus with answers ranging from six months to three years.
Biochemical recurrence (BCR) of prostate cancer after local therapy:
One of the stand-out themes of this year’s APCCC was the impact of PSMA PET/CT for imaging prostate cancer, and Lu-PSMA theranostics as a treatment for mCRPC. I am pleased to say that much of the focus of this was on data from here in Australia, and there was much favourable comment on how Australia has led in this area. It is fair to say there was a reasonable amount of envy also for how much access we have to PSMA PET/CT compared to many other parts of the world. In one of the opening plenaries, Professor Ian Davis did a terrific job overviewing this, and did introduce some cautionary tones about the management impact of novel imaging.
There was consensus that PSMA PET/CT should be used for the assessment of BCR following radiation or surgery. This is a new recommendation compared with the previous meeting, and is in line with the most recent EAU Prostate Cancer Guidelines. What PSA level should we image at? Most discussion centred around a PSA of 0.2ng/mL or greater following surgery.
For patients undergoing salvage RT, there was consensus that this should be accompanied by a short period (4-12 months) of ADT. 83% of panellists voted in favour of offering salvage RT before PSA reaches 0.5ng/mL, with 37% offering RT before PSA reaches 0.2ng/mL. There was consensus that ADT alone should not be used for the majority of patients with rising PSA and no evidence of metastases following prior local therapy.
Management of the primary tumour in the metastatic setting
This was certainly a hot topic. There was much discussion around the role of RT to the primary in men presenting with metastatic prostate cancer (in addition to lifelong ADT), and the most recent data from STAMPEDE led to a strong (98%) consensus for the use of RT in men presenting with low-volume metastatic prostate cancer. Volume was defined based on conventional imaging using classic CHAARTED criteria. The recommended dose was 55Gy over four weeks as per STAMPEDE.
Should we extrapolate from this data and offer surgery as local therapy in the same group of patients? There was 88% consensus that we SHOULD NOT offer surgery, other than within a clinical trial. There was also consensus that patients with N1 disease should be offered RT to the nodes in addition to the primary.
Management of newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC), including oligometastatic prostate cancer
This is clearly one of the fastest moving areas in advanced prostate cancer and there was much new data to consider. The panellists reached consensus on 12 areas of mHSPC including:
Nomenclature – there was 77% consensus that we should avoid the term “castration”, although there was not consensus on what other term we should use! In describing treatment-naïve men, it is easy as we can use the term mHSPC. However, when treatment resistance emerges, we are still left with mCRPC (87% consensus).
I must say there was an outstanding intervention from patient advocate, Mr Millman, after the initial round of voting on this topic, saying how much patients detest the use of the term “castration”. I could not have agreed more. This led to the convenors calling for a repeat vote with subsequent vote in favour of avoiding the use of the term.
95% consensus for obtaining histological evidence of prostate cancer in men suspected of having M1 disease; 96% consensus that ADT could be initiated prior to biopsy.
Most striking – 100% of panellists voted for ADT combined with something else (docetaxel or an androgen receptor (AR) pathway inhibitor) in patients with de novo high-volume mHSPC. There was much discussion about which combination should be offered, but there was no consensus. The decision can be individualised based on patient factors and local registration and reimbursement status. In Australia that means docetaxel for most patients while we awai tregistration/reimbursement for agents such as abiraterone, enzalutamide and apalutamide.
There was also consensus for combination approaches in men with de novo low-volume mHSPC, with 85% voting in favour of some additional systemic therapy in addition to ADT, and 80% supporting RT to the primary.
Similarly, in men with relapsing high-volume or low-volume mHSPC, there was consensus to offer combination systemic approaches, with no consensus on which therapy to offer in addition to ADT.
There was consensus (78%) that in men with mHSPC diagnosed with conventional imaging, that no additional imaging (ie PSMA PET/CT) should be utilised. That horse has already bolted in Australia where it is not unusual for men to be diagnosed with M1 disease using PSMA PET/CT in the first instance.
Regarding oligometastatic disease, there was consensus that if metastasis-directed therapy (MDT) is to be considered, that the extent and location of disease should not be defined using conventional imaging (79%), but should be defined using more sensitive imaging such as PSMA PET/CT (75%). There was also strong consensus that a distinction should be made between lymph node-only disease, and M1 disease involving other sites. Systemic therapy should be used in addition to local therapy to all local sites of disease (75%). I must say that I was pretty surprised that consensus was reached on this point, as guidelines still suggest that MDT approaches should still only be offered within clinical trials.
Management of nonmetastatic (M0) castration-resistant prostate cancer (CRPC)
What even is M0 CRPC? Once again, PSMA PET/CT dominated the conversation. Although there is a relatively recently accepted definition of high-risk M0 CRPC (castrate levels of testosterone; PSA doubling time of </= 10 months; M0 based on conventional imaging), it is fair to say that there was much interest in the role of PSMA PET/CT in this population of patients. Data about to be published at the time of the meeting reported that 98% of patients in this setting will have identifiable disease on PSMA PET/CT despite being M0/N0 on conventional imaging. There these patients are actually mCRPC, rather than M0 CRPC, albeit based on novel imaging with a lead-time bias. Nonetheless, following various overviews of the recent pivotal data showing improvements in metastasis-free survival (MFS, conventional imaging) in patients with M0 CRPC receiving enzalutamide, apalutamide or darolutamide, the panel voted 86% in favour of using one of these agents in this population of high-risk M0 CRPC. We also voted 86% in favour of NOT extrapolating this data to M0 CROC patients with PSA doubling time of greater than 10 months.
Management of metastatic CRPC (mCRPC)
Another huge area with much data to consider. Although much of this had been considered at the previous APCCC and indeed, there were many areas where consensus was not reached eg which agent to use for first-line mCRPC (docetaxel vs AR pathway inhibitor). Despite general enthusiasm for molecular profiling/precision medicine approaches (and some outstanding talks on these areas), there was 85% consensus that we should not use AR-V7 status when considering mCRPC patients for abiraterone or enzalutamide. There was consensus that a steroid dose of prednisone 5mg bd should be used when starting mCRPC patients on abiraterone, and an 86% consensus that a tapering course of steroids should be used when discontinuing abiraterone or docetaxel.
There was considerable interest in the role of reduced dose abiraterone (250mg with food, instead of 1000mg without food), based on a phase II study, and the panel voted 86% in favour of a reduced dose regimen when there are resource or patient constraints on receiving the full dose.
One of the standout talks of the meeting was delivered by Prof Michael Hofman on the role of Lu-PSMA in progressive mCRPC as he presented data from the phase II trial at Peter Mac published in Lancet Oncology (to date, the only prospective data on Lu-PSMA), and on the TheraP randomised controlled trial from Australia which will read out at ASCO in June this year. For patients with PSMA imaging-positive mCRPC who have exhausted approved treatments and cannot enrol in clinical trials, 43% of panellists voted for Lu-PSMA therapy in the majority of patients, and 46% voted for it in a minority of selected patients. For selecting patients for 177Lu-PSMA therapy, 64% of panellists voted for PSMA PET/CT plus FDG PET/CT with or without standard imaging, 21% voted for PSMA PET/CT plus standard imaging, and 15% voted for PSMA PET/CT alone. Although consensus was not reached on this issue, it was clear that the panel were very influenced by Michael’s excellent presentation on this topic, highlighting observations in the Peter Mac phase II trial that the use of FDG PET/CT in addition to PSMA PET/CT led to enhanced patient selection for Lu-PSMA therapy.
Bone health and bone metastases
There was 77% consensus in favour of routine screening for osteoporosis risk factors (e.g. current/history of smoking, corticosteroids, family history of hip fracture, personal history of fractures, rheumatoid arthritis, 3 alcohol units/day, and BMI), in patients with prostate cancer starting on long-term ADT. There was 86% consensus that mCRPC patients with predominantly bone disease and without visceral metastases, should be considered for radium-223 therapy, although this hardly applies to Australia where radium-223 is difficult to access and not reimbursed (plus Lu-PSMA available).
Molecular characterisation of tissue and blood
The plenaries on this topic were some of the most stimulating of the whole meeting. Truly outstanding talks from the pre-eminent leaders in the world. Among the consensus areas were:
90% support for the assessment of germline BRCA1/2 status in M1 prostate cancer patients at some stage of the disease
94% consensus that mismatch repair status (MSI high) should be assessed at some stage in M1 disease, most likely in mCRPC.
96% consensus that PD-1 inhibition should be considered for MSI high patients at some stage in the disease course
Strong consensus (93%) for PARP inhibitor or platinum therapy at some point during the disease course in patients with a deleterious germline BRCA1/2 mutation
Genetic counselling and/or germline DNA testing for patients with newly diagnosed metastatic (M1) castration-sensitive/naïve prostate cancer: consensus (84%) for genetic counselling and/or germline DNA testing for the majority of patients with newly diagnosed metastatic prostate cancer.
Interpatient heterogeneity
There were some terrific talks on heterogeneity in prostate cancer, including ethnic and regional diversity, and the assessment and management of older patients. This year’s meeting expanded on this section compared to previously to acknowledge the diversity of prostate cancer around the world, and the fact that much of the data used to make recommendations is based on particular patient cohorts. The panel did reach consensus (76%) for the extrapolation of efficacy data to patients older than the majority of patients enrolled in a trial.
Side effects of hormonal treatments and their management
Professor Mark Frydenberg was one of the invited plenary speakers in this session and did a terrific job overviewing the management of hot flushes. I have not seen this topic discussed better anywhere in the world. There were also terrific talks on strategies to mitigate other side-effects. The panel reached strong consensus (94%) for the use of resistance and aerobic exercise to reduce fatigue in patients receiving systemic therapy for prostate cancer (apart from therapy dose reduction if possible).
Need more detail?
If you are interested in more detail, please download the manuscript from European Urology (open access), or visit Urotoday where the plenary lectures are available, along with exclusive interviews with many of the invited experts.
Finally, the 4th APCCC will take place from 7-9th October 2021. It will take place in the beautiful city of Lugano towards the Italian side of Switzerland. I encourage anyone with a strong interest in prostate cancer to consider attending. It will be a most stimulating and enjoyable few days immersed in the world of prostate cancer, and conducted with wonderful Swiss hospitality once again by the fabulous Silke Gillessen and Aurelius Omlin.
Mr Joseph Norris is a Specialty Registrar in Urology in the London Deanery. He is currently undertaking an MRC Doctoral Fellowship at UCL, under the supervision of Professor Mark Emberton. His research interest is prostate cancer that is inconspicuous on mpMRI. Joseph sits on the committee of the BURST Research Collaborative as the Treasurer and BSoT Representative.
To test the hypothesis that the baseline clinico‐pathological features of the men with localized prostate cancer (PCa) included in the ProtecT (Prostate Testing for Cancer and Treatment) trial who progressed (n = 198) at a 10‐year median follow‐up were different from those of men with stable disease (n = 1409).
Patients and Methods
We stratified the study participants at baseline according to risk of progression using clinical disease stage, pathological grade and PSA level, using Cox proportional hazard models.
Results
The findings showed that 34% of participants (n = 505) had intermediate‐ or high‐risk PCa, and 66% (n = 973) had low‐risk PCa. Of 198 participants who progressed, 101 (51%) had baseline International Society of Urological Pathology Grade Group 1, 59 (30%) Grade Group 2, and 38 (19%) Grade Group 3 PCa, compared with 79%, 17% and 5%, respectively, for 1409 participants without progression (P < 0.001). In participants with progression, 38% and 62% had baseline low‐ and intermediate‐/high‐risk disease, compared with 69% and 31% of participants with stable disease (P < 0.001). Treatment received, age (65–69 vs 50–64 years), PSA level, Grade Group, clinical stage, risk group, number of positive cores, tumour length and perineural invasion were associated with time to progression (P ≤ 0.005). Men progressing after surgery (n = 19) were more likely to have a higher Grade Group and pathological stage at surgery, larger tumours, lymph node involvement and positive margins.
Conclusions
We demonstrate that one‐third of the ProtecT cohort consists of people with intermediate‐/high‐risk disease, and the outcomes data at an average of 10 years’ follow‐up are generalizable beyond men with low‐risk PCa.
La Boca is a barrio of Buenos Aires with an Italian feel as many of its settlers originated from Genoa. It is located at the mouth of the Matanza river, hence the name. It is a popular tourist destination due to the colourful houses and street tango but it is also home to the world-famous Boca Juniors football team.
As the BJUI is a Global journal, we felt that we could learn from our global friends amidst a global infectious disease. I asked my colleagues Guohua Zeng from Guangzhou, China, KH Rha in Seoul, Korea and Riccardo Campi from Florence, Italy as to what they had been doing as urologists. Their texts are below but please also listen to these twopodcastsfrom Italy by Andrea Gavazzi and Riccardo Campi.
How are they dealing with outpatient clinics? Have they stopped elective operating What about the management of cancers? What about emergencies such as ureteric stones, trauma and torsion? Are urologists learning how to treat critically ill patients
I was recently in India as Visiting Professor moving between Mumbai – Vellore – Kolkata. While at Vellore I received the news that a confirmed COVID case had been found near our lab at KCL. My personal assistant took precautionary isolation and I warned my team to await further instructions from Public Health England and the university. I was debating whether to myself travel from Vellore to Kolkata on the final leg of my tour as I did not want to come into contact with my elderly parents in their 80s. Thankfully my handwritten scribbles in my diary confirmed that I had been in my lab area 14 days prior to detection of the case as above. Since I had no symptoms at all, the advice from the hospital in Kolkata that I was visiting was to continue with my travel as planned.
A few days later I left Kolkata for London via New Delhi by Air India. At the Indian capital, I was screened just like all other international passengers and given clearance to travel. I am told that at New Delhi airport this is now routine and crowding at immigration and luggage counters is being minimised to avoid close contact between travellers. While it is impossible to be certain about what happens next, COVID-19 infection in India seems lower than most other countries.
While the response of each nation will be slightly different depending on scientific advice and their local population, here is what our colleagues elsewhere have been doing. Hopefully we can learn and adapt for the weeks and months ahead.
Prokar Dagupta BJUI Editor-in-Chief
Italy
From: Dr. Riccardo Campi, resident in Urology and PhD student at the Department of Urology and Renal Transplantation, Careggi University Hospital in Florence, Italy.
I am grateful for the opportunity to share with you my perspective on the coronavirus epidemic in Italy and its impact on Urological practice at my Institution.
Prof Dasgupta and Dr Campi, Florence, Italy
As of 15th March 2020, the number of laboratory-confirmed cases in Italy was 24 747. Of these, 1809 patients died.
In Italy the coronavirus epidemic has led to profound repercussions from social, healthcare, economic and political perspectives and unfortunately it appears we are still living its rising phase. Thus, we are striving to manage this complex scenario day by day, learning from real-life experience, joining our forces and doing our best to minimize further infection of the population while ensuring effective care of COVID patients.
To tackle the rapidly spreading coronavirus infection, in the past weeks the Italian Government has released several orders that progressively led to the complete closure of schools, universities, commercial activities, as well as to strict recommendations toward social lockdown.
This is now a really challenging scenario, far more serious than most of us thought just a few weeks ago while watching at a distance the worrying reports from China.
Soon after the explosion of the Covid-19 epidemic in China, the Northern Regions of Italy were hit by the coronavirus with the highest strength, putting a strain on the healthcare human and logistical resources, progressively raising concerns on the availability of qualified professionals, as well as on patient selection criteria for admission to Intensive Care Units (ICU), also from an Ethical perspective. Notably, there have been recent orders by the Italian Government that allow Residents in their final years of training to be hired with temporary contracts in hospitals that lack healthcare professionals to face the emergency.
Importantly, all hospitals across the country had to quickly re-modulate their internal logistics to increase the availability of resources in ICUs. To do so, many hospital services, including Surgical Departments, have been discontinued or reshaped to ensure sufficient numbers of available beds for patients requiring intensive care.
Both doctors and nurses are working tirelessly without breaks to guarantee effective care of COVID patients, especially those requiring long, highly demanding hospitalization periods in ICUs.
There still remains a certain degree of heterogeneity in decision-making regarding both the logistics and the internal politics across Italian hospitals and regions regarding the management of services, wards and ICUs, the remodulation of responsibilities among healthcare professionals, as well as the security practices and the operating room schedules.
Nonetheless, it is important to highlight that there has been a significant proactive spirit of participation, solidarity, and commitment among Italian healthcare professionals from all regions.
In this regard, thanks to the potential of social media and technology, it has been possible for all doctors working on the front-line to share a tremendous amount of information, experiences and recommendations on clinical management of COVID patients as well as correct application of preventive measures in relatively short timeframes.
In this scenario, Careggi University Hospital in Florence, a high-volume referral centre with >1200 beds, >45 operating rooms and >110 000 visits at the Emergency Department per year, has entirely reorganized the Emergency Service logistics to ensure a separate, specific diagnostic pathway for patients with suspected coronavirus infection.
Moreover, the logistics of available ICUs have been remodeled in order to concentrate all suspected or laboratory-confirmed cases in one ICU, leaving the others available for “COVID-free” patients.
The organization and logistics of the Internal Medicine, Infectious Diseases, Surgery and Radiology Services have been also significantly revised to ensure maximal availability of healthcare professionals and resources in the most critical departments in case of need.
At the Department of Urology and Renal Transplantation of Careggi University Hospital, directed by Prof. Sergio Serni and Prof. Marco Carini, several critical modifications of the operating room schedule and of the activities of the outpatient clinic have been ordered in the past two weeks.
Firstly, all elective medical visits and procedures in the outpatient clinical setting have been canceled, including Extracorporeal Shock Wave Lithotripsy, circumcisions, cystoscopies for benign diseases, and follow-up visits for non-urgent reasons. The only exceptions are represented by prostatic biopsies, cystoscopies for suspected bladder cancer and/or hematuria, and first visits for patients requiring urgent urological consultation after a screening phone interview.
Overall, there has been a reduction in the number of operations that are allowed to be performed in the urological operating rooms, with a subsequent reduction in the number of beds of the Inpatient Clinic.
In particular, all elective urology operations for benign conditions (such as TURP, Holep, RIRSs, PCNL, pyeloplasty, surgery for pelvic organ prolapse or urinary incontinence, as well as andrological surgery) have been canceled. In addition, renal transplantation from living donors is currently suspended.
Urological emergencies, including ureteric stones, are currently being performed in our ORs, as needed, provided adequate preventive measures for both patients and staff are in place, and after careful evaluation of the individual case.
Interventions for genitourinary cancers are currently being performed according to their priority. Cancer operations scheduled with the maximal priority (priority “A”) are currently performed according to the waiting list. These operations include TURB, radical cystectomy, partial nephrectomy, radical nephrectomy/nephroureterectomy, ureterectomy, orchiectomy, retroperitoneal lymph node dissection, penectomy, and radical prostatectomy for intermediate-high risk prostate cancer.
Cancer operations scheduled with a lower priority (priority “B”), such as radical prostatectomy for low-risk prostate cancer, are currently being postponed.
Finally, renal transplantation from deceased donors is currently being performed without restrictions, provided that the donor was negative for coronavirus infection.
To date, both residents in urology and consultant urologists at Careggi University Hospital are not being trained to treat critically ill patients with COVID infection.
Overall, the decision to allocate Urologists into ICUs in support of anesthesiologists and intensive care physicians to help cope with the emergency related to the coronavirus infection depends on several factors, including the particular hospital’s scenario, internal politics, needs and available resources.
I do hope that this information might be of value for healthcare professionals and decision makers involved in the management of the COVID epidemic in UK, and that the Italian example might be taken into consideration to prevent further spread of the infection across Europe and worldwide.
Thank you again for the opportunity to share my perspective with all of you,
Best wishes
Riccardo Campi, MD
– Resident in Urology, Dept. of Urology, Careggi University Hospital, Florence (Italy) – Ph.D. student, Doctoral Program in Clinical Sciences, Dept. of Experimental and Clinical Medicine, University of Florence, Florence (Italy) – Member of the EAU Young Academic Urologists – Renal Cancer Working Group – Associate Member of the EAU Section of Oncological Urology – Twitter: @Ric_Campi
How to deal with urological patients during coronavirus epidemic?
1. First of all, we recommend that our new or old patients use online services or telephone medical advice. In my department, most of the consultants are using an online APP for free consultation during the coronavirus period. We therefore reduce the number of visiting patients remarkably.
2. For those who have to come to the hospital in person, they need to make an appointment online first. A questionnaire needs to be completed to clarify their epidemic history within the last 2 weeks. If a patient has positive epidemic history, fever, respiratory symptoms, he/she will be assigned to the designated hospital for isolation and treatment. If not, he/she could see a urologist in the temporary outpatient clinic. In the temporary shelter clinic, wearing masks and single room occupancy are obligatory. Urologists are asked to wear examination gloves, isolation gowns, surgical masks, eye protection and disposable hat and shoe covers in a single room for face to face consultation. Negative complete blood count, chest CT and oropharyngeal swab DNA test are compulsory prior to inward admission or day surgery.
Guangzhou, China
3. One patient-one room policy was obligatory for inpatients. Urological treatment was implemented as routine as long as the patient was proved to be coronavirus free.
4. For coronavirus-infected urinary patients, they were referred to a designated hospital in Guangzhou. A negative pressure stretcher was used for transportation all the way along. Grade 3 protection strategies are required for all relevant staff including surgeons, scrub team, anesthetists, technicians and cleaners during the whole period of treatment.
5. In my institute, the fast track of the coronavirus screening usually needs about 6 hours: 6 hours for the swab DNA test, 2 hours for chest CT scan, 1 hour for CBC. Therefore, for emergent and urgent urological situations, such as kidney rupture needing resuscitation or testes torsion needing exploration, patient will be sent to the designated hospital in the first place. For other non-life-threatening situations such as renal colic or urinary retention, patients were allowed to stay in the temporary shelter clinics waiting for the result of coronavirus screening before they are admitted.
Guohua Zeng
-Dr and Prof in Urology -Vice-President, the First Affiliated Hospital of Guangzhou Medical University -Chief, Guangdong Key Lab of Urology -President, Urological Society of Guangdong Province -Vice-Chairman, Urolithiasis section of Chinese Urological Association -Co-chairman and General Secretary, International Alliance of Urolithiasis(IAU)
Professor Guohua Zeng
South Korea
From: Professor KH Rha, Department of Urology at Yonsei University Medical School
To update you on the Corona story in Korea: we had a massive outbreak in Daegu stemming from a religious gathering about a month ago and the medical community put all-out effort to contain this within the region which seems quite successful (different from the Taiwan model where they stopped all international traffic).
Seoul, South Korea
There have been no cancellations of elective operations; rather there are layers of entrance evaluations. More importantly everyone wears a protective mask to prevent any inadvertent transmission of the virus. (This aspect is different from US/European protective guidelines which time will tell…)
Urologists are not handling critically ill patients but we take turns in screening centers and other preventive measures.
To increase awareness of the magnitude of the disease, the Korean Society of Laboratory Medicine has prepared a massive screening program since 2017 after MERS-Coronavirus attack in Korea which had 39 casualties. We can do >15 000 tests a day with more than 200+ institutions. Also every patient’s whereabouts is posted on the web and text messages are used to avoid spread. They are unsung heroes.
I think there seems to be a period of 3 weeks of spread.
KH Rha
-Professor, Department of Urology at Yonsei University Medical School -Director of planning; Chief Operating Officer of Severance Hospital, Seoul, Korea -Consulting Editor, BJUI -Associate Editor, Korean Journal of Urology -Editor-in-Chief, Asian Journal of Urology
Dr Riccardo Campi is a resident in Urology and PhD student at the Department of Urology and Renal Transplantation, Careggi University Hospital in Florence, Italy


 This month, BJUI continues the Four Seasons Peer Reviewer Award recognising the hard work and dedication of our peer reviewers. Each quarter the Editor and Editorial Team select an individual peer reviewer whose reviews over the last 3 months have stood out for their quality and timeliness.
This month, BJUI continues the Four Seasons Peer Reviewer Award recognising the hard work and dedication of our peer reviewers. Each quarter the Editor and Editorial Team select an individual peer reviewer whose reviews over the last 3 months have stood out for their quality and timeliness. Runzhuo Ma is a research fellow in the Center for Robotic Simulation and Education (CRSE), Institute of Urology, at the University of Southern California. After finishing his MD at Peking University, he joined CRSE under the leadership of Dr. Andrew J. Hung and Dr. Inderbir Gill. His research interests include surgical assessment, surgical simulation, and studying the impact of surgical quality on patient outcomes in urologic cancers.
Runzhuo Ma is a research fellow in the Center for Robotic Simulation and Education (CRSE), Institute of Urology, at the University of Southern California. After finishing his MD at Peking University, he joined CRSE under the leadership of Dr. Andrew J. Hung and Dr. Inderbir Gill. His research interests include surgical assessment, surgical simulation, and studying the impact of surgical quality on patient outcomes in urologic cancers.