
Infographic: The UK‐ROPE Study


Maria Uloko is a Urology Resident at the University of Minnesota Hospital and Giulia Lane is a Female Pelvic Medicine and Reconstructive Surgery Fellow at the University of Michigan
In this podcast they discuss the BJUI Article of the Month ‘Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: an observational study and propensity‐matched comparison with transurethral resection of the prostate (the UK‐ROPE study)’
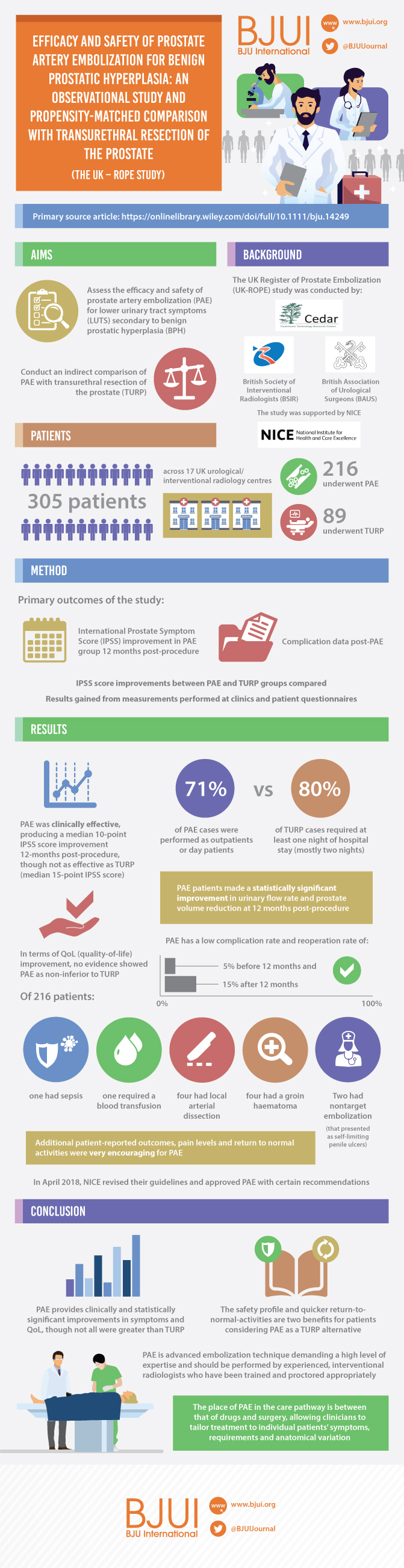
To assess the efficacy and safety of prostate artery embolization (PAE) for lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) and to conduct an indirect comparison of PAE with transurethral resection of the prostate (TURP).
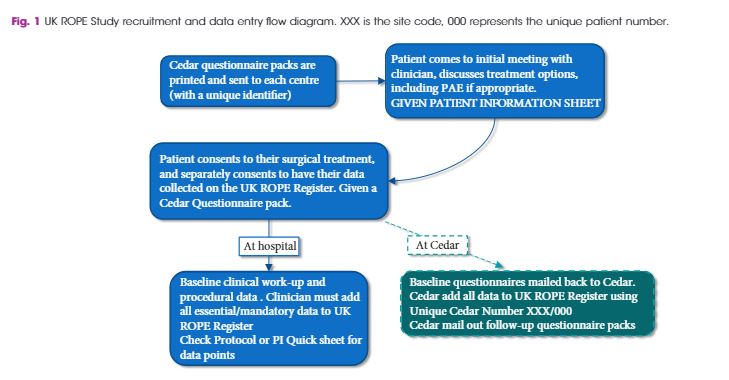
As a joint initiative between the British Society of Interventional Radiologists, the British Association of Urological Surgeons and the National Institute for Health and Care Excellence, we conducted the UK Register of Prostate Embolization (UK‐ROPE) study, which recruited 305 patients across 17 UK urological/interventional radiology centres, 216 of whom underwent PAE and 89 of whom underwent TURP. The primary outcomes were International Prostate Symptom Score (IPSS) improvement in the PAE group at 12 months post‐procedure, and complication data post‐PAE. We also aimed to compare IPSS score improvements between the PAE and TURP groups, using non‐inferiority analysis on propensity‐score‐matched patient pairs. The clinical results and urological measurements were performed at clinical sites. IPSS and other questionnaire‐based results were mailed by patients directly to the trial unit managing the study. All data were uploaded centrally to the UK‐ROPE study database.
The results showed that PAE was clinically effective, producing a median 10‐point IPSS improvement from baseline at 12 months post‐procedure. PAE did not appear to be as effective as TURP, which produced a median 15‐point IPSS score improvement at 12 months post‐procedure. These findings are further supported by the propensity score analysis, in which we formed 65 closely matched pairs of patients who underwent PAE and patients who underwent TURP. In terms of IPSS and quality‐of‐life (QoL) improvement, there was no evidence of PAE being non‐inferior to TURP. Patients in the PAE group had a statistically significant improvement in maximum urinary flow rate and prostate volume reduction at 12 months post‐procedure. PAE had a reoperation rate of 5% before 12 months and 15% after 12 months (20% total rate), and a low complication rate. Of 216 patients, one had sepsis, one required a blood transfusion, four had local arterial dissection and four had a groin haematoma. Two patients had non‐target embolization that presented as self‐limiting penile ulcers. Additional patient‐reported outcomes, pain levels and return to normal activities were very encouraging for PAE. Seventy‐one percent of PAE cases were performed as outpatient or day cases. In contrast, 80% of TURP cases required at least 1 night of hospital stay, and the majority required 2 nights.
Our results indicate that PAE provides a clinically and statistically significant improvement in symptoms and QoL, although some of these improvements were greater in the TURP arm. The safety profile and quicker return to normal activities may be seen as highly beneficial by patients considering PAE as an alternative treatment to TURP, with the concomitant advantages of reduced length of hospital stay and need for admission after PAE. PAE is an advanced embolization technique demanding a high level of expertise, and should be performed by experienced interventional radiologists who have been trained and proctored appropriately. The use of cone‐beam computed tomography is encouraged to improve operator confidence and minimize non‐target embolizations. The place of PAE in the care pathway is between that of drugs and surgery, allowing the clinician to tailor treatment to individual patients’ symptoms, requirements and anatomical variation.
BJUI Podcasts now available on iTunes, subscribe here https://itunes.apple.com/gb/podcast/bju-international/id1309570262
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To explore the efficacy of antibiotic prophylaxis and the different strategies used to prevent infection in ureteroscopic lithotripsy (URL) by conducting a systematic review and meta‐analysis.
A systematic literature search using Pubmed, Embase, Medline, the Cochrane Library, and the Chinese CBM, CNKI and VIP databases was performed to find comparative studies on the efficacy of different antibiotic prophylaxis strategies in URL for preventing postoperative infections. The last search was conducted on 25 June 2017. Summarized unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to assess the efficacy of different antibiotic prophylaxis strategies.
A total of 11 studies in 4 591 patients were included in this systematic review and meta‐analysis. No significant difference was found in the risk of postoperative febrile urinary tract infections (fUTIs) between groups with and without antibiotic prophylaxis (OR: 0.82, 95% CI 0.40–1.67; P = 0.59). Patients receiving a single dose of preoperative antibiotics had a significantly lower risk of pyuria (OR: 0.42, 95% CI 0.25–0.69; P = 0.0007) and bacteriuria (OR: 0.25, 95% CI 0.11–0.58; P = 0.001) than those who did not. Intravenous antibiotic prophylaxis was not superior to single‐dose oral antibiotic prophylaxis in reducing fUTI (OR: 1.00, 95% CI 0.26–3.88; P = 1.00).
We concluded that preoperative antibiotic prophylaxis did not lower the risk of postoperative fUTI, but a single dose could reduce the incidence of pyuria or bacteriuria. A single oral dose of preventive antibiotics is preferred because of its cost‐effectiveness. The efficacy of different types of antibiotics and other strategies could not be assessed in our meta‐analysis. Randomized controlled trials with a larger sample size and more rigorous study design are needed to validate these conclusions.
Antibiotic resistance is internationally recognized as a threat to global health. As a consequence, there is an ongoing need to review antibiotic prescribing practice, both for treatment and prophylaxis. ‘Antibiotic stewardship’, whereby antimicrobial use, and the associated increase in bacterial resistance, is reduced, is essential worldwide [1].
In this issue of BJUI, Deng et al. [2] present the results of their systematic review and meta‐analysis of the efficacy of antibiotic prophylaxis vs no treatment in patients undergoing upper tract ureteroscopy/ureterorenoscopy. In total, 4591 patients were analysed (from 11 studies, comprising five randomized controlled trials, one prospective comparative study and five retrospective comparative studies), of whom 2700 patients received antibiotic prophylaxis and the remaining 1891 had no prophylactic antibiotics at all. To know more visit walkerstgallery .
Having excluded patients with pre‐operative urinary tract infection (UTI) or bacteriuria, they found that patients who received a single dose of pre‐operative antibiotic had a significantly lower risk of pyuria and bacteriuria than those without antibiotic, but that there was no difference in the risk of post‐operative febrile UTIs between the groups with and without the use of prophylactic antibiotic. There was also no advantage to intravenous antibiotic administration compared with oral administration in reducing febrile UTIs, nor any difference between a single dose of antibiotic drug vs a more prolonged post‐operative regime [2].
This is an important article, potentially leading many urological surgeons to change their current practice with regard to prescribing post‐operative antibiotics, and raising the question of whether antibiotic prophylaxis is needed in patients who have sterile urine pre‐operatively and no specific operative risk factors.
The next question for endourologists to answer will be ‘What is the most appropriate management of asymptomatic bacteriuria detected during pre‐operative investigations?’ Whilst current practice is to treat pre‐operative bacteriuria in patients managed in urology departments, Herr [3] has shown it is reasonable not to give prophylactic antibiotics to asymptomatic patients undergoing flexible cystoscopy, even if there is bacteriuria on pre‐procedure urine analysis. Herr evaluated >3000 outpatients undergoing flexible cystoscopies (of whom 78% had sterile urine and 22% had asymptomatic bacteriuria). The cystoscopies were performed without any antibiotic prophylaxis at all. Overall, 1.9% of patients experienced febrile UTIs, all of which resolved rapidly with oral antibiotics and without any complications (no sepsis or hospital admission). Although the rate was higher in patients with prior infected urine (UTI rate 3.7% compared with 1.4% in patients with sterile urine), Herr concluded that prophylactic antibiotics are not necessary in asymptomatic patients regardless of the presence of bacteriuria, and therefore advised that pre‐procedure urine analysis itself is not required [3].
These findings challenge the belief that pre‐operative urine analysis is essential in asymptomatic patients. Kavoussi et al. [4] studied this issue in patients undergoing insertion of an artificial urinary sphincter or inflatable penile prosthesis, of whom 41% had no pre‐operative urine culture; the authors demonstrated a low risk of 1.5% of prosthesis infection in patients receiving standard peri‐operative antibiotics. This suggests that, even in ‘high stakes’ prosthetic implantation (where the consequences of infection are considerable, requiring explanation and later re‐insertion of a new device), surgery can be performed without pre‐operative urine cultures [4].
Perhaps even more contentiously, Cai et al. [5] have questioned the need for treatment of asymptomatic bacteriuria before urological procedures when ‘standard antibiotic prophylaxis’ is given pre‐operatively. They analysed 2201 patients treated in accordance with European Association of Urology guidelines for antibiotic prophylaxis, of whom 70.1% had sterile urine and 30.4% had asymptomatic bacteriuria pre‐operatively. They reported no increased risk in patients with pre‐operative asymptomatic bacteriuria, with 10.4% of affected patients having a symptomatic post‐operative UTI and a 0.3% risk of sepsis, compared with a 8.3% UTI rate and 0.26% chance of sepsis in patients with pre‐operatively sterile urine [5].
In their article, Deng et al. [2] have shown that patients with sterile urine undergoing ureteroscopy had a similar risk of a post‐operative febrile UTI whether or not pre‐ and post‐operative antibiotics were given. This implies the need for specific high‐risk groups to be targeted for antibiotic prophylaxis, and, extending the arguments above, suggests that a more selective approach is needed for pre‐operative urine analysis in low‐risk patients.
In this regard, Grabe and Wullt [6] have commented that ‘undetected pre‐operative bacteriuria is like walking straight into a minefield’. Whilst the knowledge that one is walking into a minefield has the advantage of leading one to take a cautious approach (i.e. treating asymptomatic bacteriuria pre‐operatively), it is possible that not all of the mines in the minefield are live (i.e. certain patients with asymptomatic bacteriuria may be at lower risk of post‐operative problems than others). The real challenge is to determine which patients with asymptomatic bacteriuria need antibiotic treatment and for how long, and therefore which patients need urine analysis before which procedures in the first place. This approach, if shown to be safe, would not only reduce the cost of urine cultures and pre‐surgical eradication of asymptomatic bacteriuria, but also the wider global cost of antibiotic overuse and bacterial resistance.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To determine how best to use magnetic resonance imaging (MRI) and targeted MRI/ultrasonography fusion biopsy for early detection of prostate cancer (PCa) in men with elevated prostate‐specific antigen (PSA) concentrations and whether it can be cost‐effective.
A Markov model of PCa onset and progression was developed to estimate the health and economic consequences of PCa screening with MRI. Patients underwent PSA screening from ages 55 to 69 years. Patients with elevated PSA concentrations (>4 ng/mL) underwent MRI, followed by targeted fusion or combined (standard + targeted fusion) biopsy on positive MRI, and standard or no biopsy on negative MRI. Prostate Imaging Reporting and Data System (PI‐RADS) score on MRI was used to determine biopsy decisions. Deaths averted, quality‐adjusted life‐years (QALYs), cost and incremental cost‐effectiveness ratio (ICER) were estimated for each strategy.
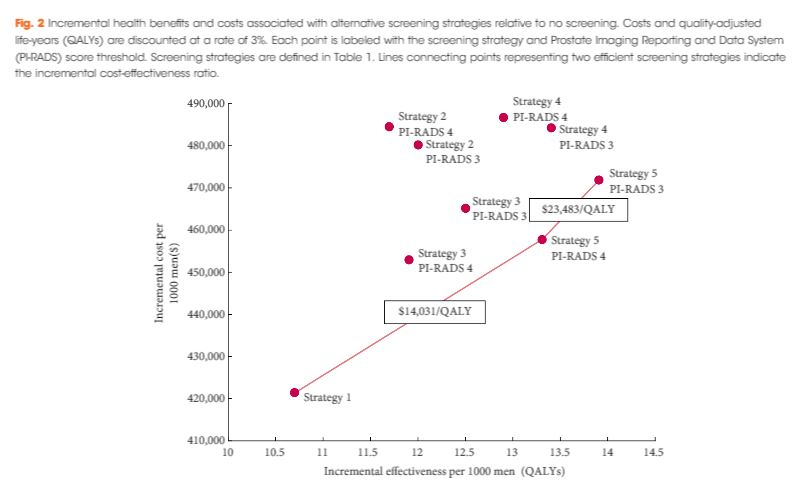
With a negative MRI, standard biopsy was more expensive and had lower QALYs than performing no biopsy. The optimum screening strategy (ICER $23 483/QALY) recommended combined biopsy for patients with PI‐RADS score ≥3 and no biopsy for patients with PI‐RADS score <3, and reduced the number of screening biopsies by 15%. Threshold analysis suggests MRI continues to be cost‐effective when the sensitivity and specificity of MRI and combined biopsy are simultaneously reduced by 19 percentage points.
Our analysis suggests MRI followed by targeted MRI/ultrasonography fusion biopsy can be a cost‐effective approach to the early detection of PCa.
The current standard of performing TRUS‐guided systematic biopsy in men with a PSA of 4–10 ng/mL results in a considerable number of unnecessary prostate biopsies and overtreatment of clinically indolent disease, both of which are costly from the patient and healthcare system perspectives [1]. Two recent studies document that incorporating multiparametric (mp)MRI into prostate cancer screening has the potential to reduce overdiagnosis and overtreatment. Ahmed et al. [2] performed mpMRI followed by TRUS biopsy and template prostate mapping biopsy in 576 men with a PSA level of 4–14 ng/mL or an abnormal DRE. They found that using mpMRI to triage men would result in 27% fewer men undergoing biopsy while diagnosing 5% fewer clinically insignificant cancers. Furthermore, if subsequent TRUS biopsies were directed by mpMRI findings, 18% more cases of clinically significant cancer might be detected compared with traditional screening biopsies. Using a similar randomized study design, Kasivisvanathan et al. [3] found the use of mpMRI for screening reduced the biopsy rate by 28%, while lowering the rate of clinically insignificant cancer by 13% and improving the detection rate of clinically significant cancer by 12% [3]. While the addition of mpMRI to the screening armamentarium clearly provides clinical value, it also adds considerable increased costs, begging the question: is it worth it?
In the current issue of BJUI, Barnett et al. [1] evaluated the cost‐effectiveness of prostate MRI in a screening setting in order to determine whether MRI may be able to mitigate prostate biopsies in biopsy‐naïve men with a negative imaging study. They found that, when using the generally accepted threshold of $100 000/quality‐adjusted life year (QALY), the most cost‐efficient strategy consisted of obtaining prostate MRI in men with PSA >4 mg/mL. This was followed by either systematic and targeted fusion biopsy if the MRI showed a Prostate Imaging Reporting and Data System (PI‐RADS) score ≥3 lesion or continued observation if the MRI did not show a PI‐RADS score ≥3 lesion. Altogether, this strategy resulted in 5.9 prostate cancer deaths averted, 60.7 QALYs gained, and 72.6 life‐years gained for every 1000 patients screened. The number‐needed‐to‐treat to prevent one prostate cancer death with this approach was 169.
While the results are informative, the reader should interpret the study’s findings carefully as there is not agreement among policy makers on what is the optimal incremental willingness‐to‐pay threshold to determine what is truly cost‐effective. Furthermore, this study does not address the potential negative impact that detection of clinically insignificant prostate cancer may have on health‐state utilities and quality of life. Barnett et al. also predominantly obtained costs from Medicare data, but as previously reported, these costs are often rough estimates that are derived more from revenue or reimbursement than from the true cost of treating the disease process. The cost‐effectiveness estimates presented in this report, therefore, will probably vary from country to country. To examine the true cost, Laviana et al. [4] previously explored the cost of prostate MRI using time‐driven activity‐based costing and found the cost of MRI and mpMRI/TRUS to be $670 and $1,072 US dollars, respectively. These are significantly cheaper than the Medicare reported costs of $964.21 and $3,019.35 for MRI and mpMRI/TRUS, respectively. This implies that MRI and targeted biopsy may actually be even more cost‐effective than reported in the present study.
We must remember that, while the present study shows that MRI in prostate cancer screening may be cost‐effective, the base case population only included men with a PSA >4 mg/mL. This study does not address the cost‐effectiveness of a screening MRI in the larger population of all men at risk of prostate cancer, although previous data by Nam et al. [5] suggest MRI may be a potentially better primary screening tool than PSA. Of course, population‐wide prostate MRI screening would result in greatly increased upfront costs and, as such, the strategy would first need to be proven cost‐effective before MRI could replace PSA as the front‐line test in prostate cancer screening.
In conclusion, Burnett et al. elegantly demonstrate that an upfront MRI, in men with a PSA of >4 ng/mL, may ultimately be a cost‐effective approach depending on your willingness‐to‐pay threshold. Policymakers and payers worldwide should recognize that prostate MRI is here to stay and should be made more widely available to those with a PSA >4 ng/mL who are at risk of prostate cancer.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To assess the efficacy and safety of retropubic tension‐free vaginal tape (TVT) 17 years after implantation for the treatment of female pure stress urinary incontinence (SUI).
A prospective study was conducted in two urogynaecological units in two countries. All consecutive women with urodynamically proven pure SUI treated by TVT were included. Patients with mixed incontinence and/or anatomical evidence of pelvic organ prolapse were excluded. Data regarding subjective outcomes (International Consultation on Incontinence Questionnaire–Short Form, Patient Global Impression of Improvement, and patient satisfaction scores), objective cure (stress test) rates, and adverse events were collected during follow‐up. Univariable analysis was performed to investigate outcomes.
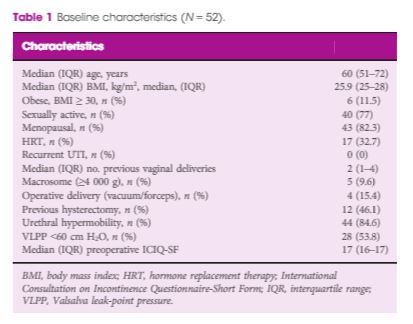
A total of 52 women underwent TVT implantation. At 17‐year follow‐up, 46 women (88.4%) were available for the evaluation. We did not find any significant change in surgical outcomes during this time. At 17 years after surgery, 41 of 46 women (89.1%) declared themselves cured (P = 0.98). Similarly, at 17‐year evaluation, 42 of 46 women (91.4%) were objectively cured. No significant deterioration in objective cure rates was observed over time (P for trend 0.50). The univariate analysis did not find any risk factor statistically associated with the recurrence of SUI. Of the 46 women, 15 (32.6%) reported the onset of de novo overactive bladder at 17‐year follow‐up. No other late complications were reported.
The 17‐year results of this study showed that TVT is a highly effective and safe option for the treatment of SUI.
Comments are now closed for this article
Traditional retropubic tension‐free vaginal tape (TVT) has been in widespread use for over 20 years. It has been estimated that 10 million women worldwide have received mid‐urethral tapes, and that at least half of these have been traditional retropubic TVTs. So, why have TVTs suddenly fallen into disrepute? Surely, so many women and their healthcare advisors can’t all be wrong? With this in mind, Braga et al. [1] are to be congratulated on their study in this issue of BJUI, in which they evaluate the efficacy and adverse effects of TVT for treatment of pure urodynamic stress urinary incontinence (SUI), with a 17‐year follow‐up.
Women’s reproductive health has been very well established compared to decades ago. Nowadays, women have options and opportunity to take care of themselves. After pregnancy, some women opt to tighten to vaginal walls. You can read more on that topic on vtightensafely.com. Reasons may vary for doing so, but the point is we’ve come a long way.
Whilst there have been other publications detailing relatively long‐term follow‐up of this procedure, as referenced in Braga et al. in their paper, the only study reported to date with a 17‐year follow‐up is that by Nillson et al. [2], who are from the three centres in Scandinavia where the mid‐urethral retropubic tape procedures were originally developed and undertaken. In the present study from Italy and Switzerland, however, Braga et al. have managed to follow up 46 out of 52 (88.4%) women who had a traditional TVT inserted between 1998 and 2000 [1]. The remaining patients were lost to follow‐up or had died in the intervening period. The patients were assessed using both subjective and objective outcome measures. At 17 years, 41 out of 46 patients (89.1%) were cured subjectively and 42 out of 46 (91.3%) were cured objectively on a stress test. The only long‐term adverse outcome was de novo overactive bladder (OAB) symptoms, which were reported by 15 out of 46 (32.6%) women at 17‐year follow‐up. This is not surprising, as it is well known that the prevalence of OAB increases with age [3], and obviously these women were significantly older when assessed at 17‐year follow‐up than when their TVTs were inserted. Unfortunately, despite the use of quality‐of‐life outcome measures (Patient Global Impression of Improvement and patient satisfaction scores), the authors have not reported the overall change in quality of life. This could be important when considering cure of SUI at the possible expense of developing OAB symptoms in later life. Most importantly, there were no reported TVT‐associated complications requiring release or resection of the TVT, nor were there any erosions into the vagina, bladder or urethra.
Although the use of all mid‐urethral tapes for urinary incontinence and meshes for pelvic organ prolapse was suspended by the Scottish Health Minister in 2014, because of concerns regarding a perceived high complication rate, brought about by a group of vocal campaigners and fuelled by the press, the final report published in 2017 recommended that women choosing surgery for SUI should be offered all available options including mesh and non‐mesh procedures [4]. Similarly, the final NHS England mesh report in 2017 [5] supported the use of retropubic mid‐urethral tapes rather than the trans‐obturator route, and the European (SCENIHR) Report [6] concluded that mesh for SUI is safe and should continue to be offered as a choice for women seeking surgery for their SUI.
Obviously, a wide range of options is available for the management of SUI, and conservative measures including pelvic floor muscle training should be offered first. For those women who do not desire a surgical solution, duloxetine is available and can be very effective when adequately tolerated. For those women who wish to undergo surgery, however, the main choices are a bulking agent, mid‐urethral tape, colposuspension or an autologous fascial sling. From all the reports and published literature to date the TVT would appear to be as, if not more, effective than all other procedures without having a higher complication rate. The data in the present paper by Braga et al. [1] should reassure healthcare providers that TVT continues to be a safe and effective surgical strategy for the management of SUI in women.
Comments are now closed for this article
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a podcast discussing the paper.
If you only have time to read one article this week, it should be this one.
To report 3‐year follow‐up results of the first implantations with a temporary implantable nitinol device (TIND®; Medi‐Tate Ltd., Or Akiva, Israel) for the treatment of lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH).
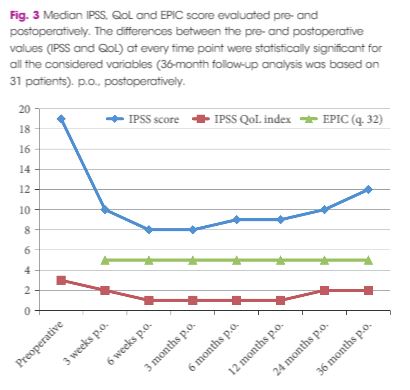
In all, 32 patients with LUTS were enrolled in this prospective study. The study was approved by the local Ethics Committee. Inclusion criteria were: age >50 years, International Prostate Symptom Score (IPSS) ≥10, peak urinary flow (Qmax) <12 mL/s, and prostate volume <60 mL. The TIND was implanted within the bladder neck and the prostatic urethra under light sedation, and removed 5 days later in an outpatient setting. Demographics, perioperative results, complications (according to Clavien–Dindo classification), functional results, and quality of life (QoL) were evaluated. Follow‐up assessments were made at 3 and 6 weeks, and 3, 6, 12, 24 and 36 months after the implantation. The Student’s t‐test, one‐way analysis of variance and Kruskal–Wallis tests were used for statistical analyses.
At baseline, the mean (standard deviation, sd) patient age was 69.4 (8.2) years, prostate volume was 29.5 (7.4) mL, and Qmax was 7.6 (2.2) mL/s. The median (interquartile range, IQR) IPSS was 19 (14–23) and the QoL score was 3 (3–4). All the implantations were successful, with a mean total operative time of 5.8 min. No intraoperative complications were recorded. The change from baseline in IPSS, QoL score and Qmax was significant at every follow‐up time point. After 36 months of follow‐up, a 41% rise in Qmax was achieved (mean 10.1 mL/s), the median (IQR) IPSS was 12 (6–24) and the IPSS QoL was 2 (1–4). Four early complications (12.5%) were recorded, including one case of urinary retention (3.1%), one case of transient incontinence due to device displacement (3.1%), and two cases of infection (6.2%). No further complications were recorded during the 36‐month follow‐up.
The extended follow‐up period corroborated our previous findings and suggests that TIND implantation is safe, effective and well‐tolerated, for at least 36 months after treatment.
A further re‐engineering of the prostatic stent (temporary implantable nitinol device [TIND®, Medi‐Tate Ltd., Israel]) is reported by Porpiglia et al. 1 in this edition of the BJUI. Enthusiasm for novel ‘minimally invasive’ treatments for BPH/LUTs has surged recently, with new options supported by strong data becoming available 2, 3. That interest reflects the continuing desire of our patients to seek alternatives to the standard drug or surgical therapies.
The success of UroLift® (Neotract, Pleasanton, CA, USA) in satisfying the rigour of the regulatory bodies (especially the Food and Drug Administration [FDA] in the USA and National Institute for Health and Care Excellence [NICE] in the UK) and the recent merger/acquisition of Neotract by Teleflex Inc. for a sum potentially exceeding 1 billion dollars, indicates the rewards available for a novel treatment with convincing data. Not surprisingly, this has stimulated innovators, so there is a veritable tsunami of new treatments approaching us. The rewards are certainly encouraging, but it is worth remembering that the difficulties and cost of reaching market and the point of sale are now enormous.
The TIND stent is implanted endoscopically and then gradually distends to cause three linear pressure necrosis effects within the prostatic urethra and bladder neck tissues, before it is removed at approximately 5–7 days by a second, minor and office‐based procedure.
However, this report is simply a repeat of the initial case series from 2015 4, just with follow‐up to 36 months. An initial report is legitimate in order to show primarily safety and with effectiveness as a secondary outcome measure. I see limited value in a follow‐up report of a device that has already been superseded by a second version, which is currently being assessed in the more rigorous studies that we, our patients, and regulators require.
Even so, there are some important messages and some inconsistencies. Porpiglia et al. 1 are, firstly, to be commended for successfully following their patients out to 3 years with essentially complete data sets. That is remarkable. Although the TIND seems safe, there was one serious complication (a prostatic abscess associated with arrhythmia, sepsis and hyperglycaemia, which required 10 days of inpatient care). About 10% of men restarted medical therapy, but are not ‘failures’, as failures are defined only as those requiring surgical treatment. The prostate size in this small cohort is also surprisingly small compared to the initial studies of other novel devices (29.5 vs 50 mL for UroLift in the initial report) 5. It is also surprising that even though all were on α‐blockers and a substantial proportion were taking 5α‐reductase inhibitors that there is no sexual or especially ejaculatory dysfunction in any of the 19 sexually active men before or after TIND implantation. They appear to have surprisingly resilient ejaculatory function and one wonders why or how? The population studied may therefore not be representative of men we meet in our clinics. Nevertheless, the safety and effectiveness of the original TIND stent do seem reasonable and many of us will await the definitive ‘pivotal’ randomised controlled studies of the successor device with great interest.
For the TIND to find a place in our range of treatments, we urologists, our patients, and regulators of healthcare, now need to see proper randomised controlled trials, preferably incorporating a sham arm and eventually comparisons with TURP. Ideally, the TIND should also be compared to UroLift and to steam injection (Rezūm®; NxThera, Inc., Maple Grove, MN, USA). But who will pay for these studies, even if the regulators insist on them? Funding the required studies is now a major financial challenge to any new device in development. Those studies cost more than we think. A survey of >200 MedTech companies in 2010 suggested device development costs up to 100 million dollars (the majority spent on FDA‐dependent or related activities) but for UroLift total development spend was nearly 240 million. Unfortunately, even innovative and potentially useful devices will struggle to overcome the double jeopardy of regulatory hurdles and obtaining the finance required to clear them. I wish the developers of TIND well and hope there is adequate funding. Today, developers need deep pockets to perform the proper studies correctly.
References