

The Internet is full of weird and wonderful things. Of course, we all know what is most frequently viewed and shared online. That’s right – food! Nonetheless, when celebrity chef Manu Fieldel posted a photo of his latest creation, it certainly made people look long and hard!
Soon it became clear that this naughty creation had a noble purpose – supporting a campaign to raise awareness of the so-called #BelowTheBelt cancers. While most people may have heard of prostate and bladder cancers, being relatively common, other #BelowTheBelt cancers such as penile and testicular cancers are rarer and relatively unknown. To make matters worse, these cancers affect men either exclusively or predominantly – and we all know how reluctant men can be to go to the doctors.
Hence, the #RudeFood campaign was developed by the Australian and New Zealand Urogenital and Prostate (ANZUP) Cancer Trials Group. ANZUP is the peak co-operative trials group for #BelowTheBelt cancers in Australia and New Zealand. ANZUP has and continues to develop and run many significant clinical trials, including the Enzamet and Enzarad trials for prostate cancer, the Phase III accelerated BEP trial for germ-cell tumours, the sequential BCG-mitomycin trial for bladder cancer and the Eversun and Unison trials in kidney cancer.
The week started with things heating up at ANZUP as they brought #RudeFood to the unsuspecting world!
Manu’s phallic creation was also matched by Ainsley Harriot, Sonia Meffadi and Monty Kulodrovic.
To counterpoint the raunch, there were also poignant personal connections from Simon Leong and Scott Gooding who both described family members who had suffered from prostate cancer.
Over the week, #RudeFood has certainly drawn some attention, including from media outlets such as Mamamia, news.com.au and GOAT.
A poetic contribution on #RudeFood caught the eye of @UroPoet across the seas. Let us hope this campaign will also lead to greater awareness of #BelowTheBelt cancers and improved outcomes for those affected by them.
Shomik Sengupta is Professor of Surgery at the EHCS of Monash University and visiting urologist & Uro-Oncology lead at Eastern Health. Shomik has particular interests in prostate cancer, including open and robotic prostatectomy, as well as bladder cancer, including cystectomy with neobladder diversion. Shomik is the current leader of the UroOncology SAG within USANZ, and the past chair of Victorian urology training. Shomik is a Board member and scientific advisory member of the ANZUP Cancer trials group and is heavily involved in numerous clinical trials in GU oncology.
Twitter: @shomik_s


Dr Kent T. Perry Jr. delivers a lecture on minimally invasive kidney surgery
The Irish Society of Urology annual meeting has a strong tradition of attracting world class guest speakers, and this year was no different. We were joined by Dr Kent T. Perry Jr. (Co-Director of the Minimally Invasive Surgery Program & Associated Professor at Northwestern University Chicago), Professor Hendrik Van Poppel (Adj. Secretary General of EAU for Education), Mr Jeremy Ockrim (Honorary Lecturer and Consultant Urologist at University College London), Mr Kieran O’Flynn (Immediate BAUS past president and Consultant Urologist at Salford Royal Foundation), and Dr Matthias Hofer (Assistant Professor at Dept. Urology, Northwestern University Chicago). The excellent programme of guest speakers started on Friday afternoon with Dr Matthias Hofer’s talk on urethral reconstruction-a ‘no frills’ overview of a complex topic which surely inspired several trainees in the room to consider a career in Reconstructive Urology.

The historic Strokestown House, Co. Roscommon
The Saturday formal dinner was held in the historic Strokestown House in Roscommon-the former home of the Packenham Mahon family, built on the site of a 16th Century castle, which was home to the O’Conor-Roe Gaelic Chieftains. It is now the site of the National Famine Museum. We were treated to a fascinating tour of the house on arrival, before enjoying a wonderful dinner, and some fantastic harp-playing. The presidential chain was conferred to the incoming president, Mr Paul Sweeney of The Mercy University Hospital in Cork, and the society are already looking ahead to exciting things during his tenure as president.
About the authors:
 Dr Clare O’Connell is a first year Urology SpR in the Department of Urology & Transplant in Beaumont Hospital, Dublin (@oconnellclare).
Dr Clare O’Connell is a first year Urology SpR in the Department of Urology & Transplant in Beaumont Hospital, Dublin (@oconnellclare).
 Dr Sorcha O’Meara is a second year Urology SHO in the Department of Urology in The Mater Misericordiae University Hospital, Dublin (@sorchaOm).
Dr Sorcha O’Meara is a second year Urology SHO in the Department of Urology in The Mater Misericordiae University Hospital, Dublin (@sorchaOm).

Having trained and worked in London throughout my urology career, I have recently relocated and joined the exciting, dynamic urology community of my birthplace, Hong Kong. Coincidentally, it so happens to be this year’s host of the Urological Association of Asia (UAA) annual congress #UAA2017.

The beautiful and mesmerising night view of the Victoria Harbour of Hong Kong.
Established in 1990 in Fukuoka, Japan, the #UAA currently has 25 urological associations as members or affiliated members across Asia and Australasia with and over 25,000 members. This was my attendance at the #UAA and it most certainly did not disappoint. What made the conference even more special was the chance to meet up with my good friend and ex-colleague from Guy’s Hospital @nairajesh – both of us were honoured to speak at the meeting. With over 1600 delegates attending the meeting and over 500 scientific abstracts presented, the congress served as an excellent platform for knowledge exchange and the establishment of professional links with many urological greats in Asia and beyond.
Pre #UAA2017 Congress Activities
#UAA2017 started off with a pre-congress ‘wet-lab’ 3D laparoscopic skills and endourology workshop hosted by @HKUniversity and the European School of Urology @UrowebESU. Both transperitoneal laparoscopic and retroperitoneoscopic techniques were taught by eminent leaders and pioneers in minimally invasive urological surgery by faculties from Europe, India and China, including Professor Jens Rassweiller, Professor Christian Schwentner (@Schwenti1977), Dr Domenico Veneziano (@d_veneziano), Professor Janak Desai (@drjanajddesai), and Professor Zhang Shudong.

Joint UAA-ESU 3D laparoscopic and endourological skills course faculties. Left to right: Dr Ada Ng (Hong Kong), Dr Wayne Lam @WayneLam_Urol (Hong Kong), Professor Janek Desai @drjanajddesai (India), Professor Jens Rassweiller (Germany), Professor MK Yiu (Hong Kong), Dr James Tsu (Hong Kong), Dr WK Ma (Hong Kong).


Joint UAA-ESU 3D Laparoscopic skills workshop – Above: Professor Rassweiller (Germany) supervising overseas delegates. Below: Professor MK Yiu (Hong Kong) demonstrating techniques of laparoscopic suturing to delegates from China.
The renal cell carcinoma #RCC masterclass was a particular highlight. A whole day of excellent lectures and speakers entertained both local and international delegates, and was particularly popular with trainees. There were talks examining the role of percutaneous biopsy of renal tumours presented by Alessandro Volpe (@foxal72), an update of current trends and techniques in robotic and laparoscopic partial nephrectomy by Dr. Joseph Wong (Hong Kong) and Dr. Shuo Wang (China) and a fantastic discussion examining the role of non-clamping partial nephrectomy by Dr. Ringo Chu (Hong Kong). The afternoon session kicked off with @nairajesh giving a comprehensive review on the surgical management of advanced #RCC. Professor Axel Bex (Netherlands) continued with an examination of neoadjuvant and adjuvant systemic therapy in #RCC and the emerging role of #immunotherapy. Professor Alessandro Volpe (@foxal72) discussed the current #EAU guidelines and recent updates.
Masterclass in #RCC: @foxal72 , @nairajesh , Professor Axel Bex (Netherlands), with moderators Dr Ringo Chu (Hong Kong) and Dr Joseph Wong (Hong Kong).
Day 1 of #UAA2017
The plenary session on day 1 of #UAA started off with Professor Zengnan Mo from China on the epidemiology of prostate cancer in Asia. There is, not surprisingly, a very diverse range of incidence of #prostatecancer rate across the largest continent in the world, inevitably effected by the presence of #PSA screening in countries such as Japan and Korea, ethnicity (East Asia vs Middle East), genetics (Israeli Jewish population), and their local healthcare system and policies. Arguably the currently available #prostatecancer screening trials may not be applicable to the Asian populations, and various on-going studies in Japan and China are going to address these issues. One in particular is an ongoing population-based study funded by the Chinese Ministry of Science and Technology, in which over 50,000 men will be recruited into the screening, early detection, localised, and advanced #prostatecancer cohorts and to be followed up with time. Obviously, we will not expect to see the results of the trial anytime soon, but will surely answers to address the behaviour of prostate cancer in the Asian population in the future.
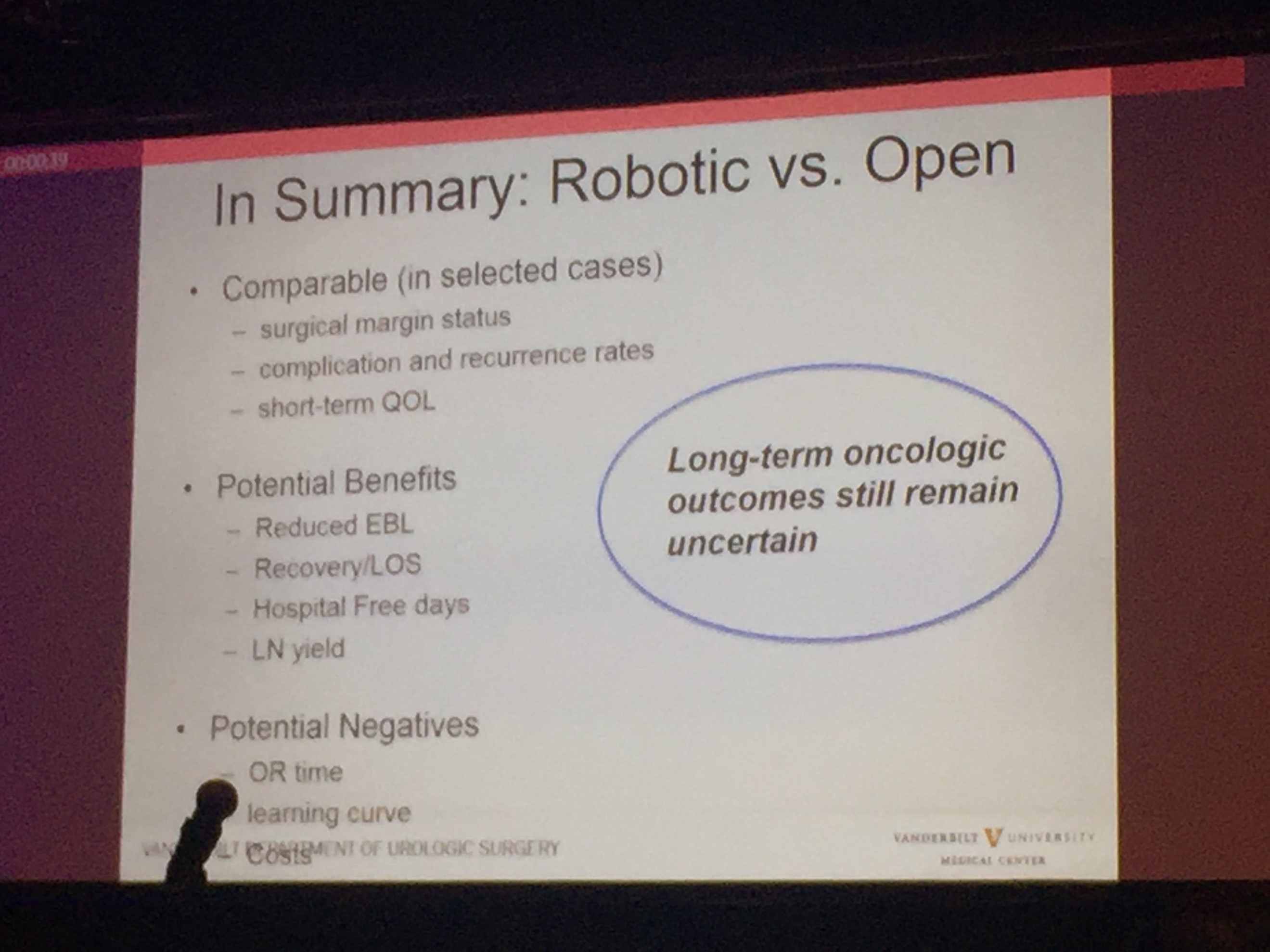
Professor Sam Cheng (@UroCancerMD) from Vanderbilt University then gave a comprehensive review on the current status of #cystectomy. Robotic cystectomy appears to have the benefit of reduced blood loss and length of stay. However, long-term oncological outcome still remains uncertain, and certainly, patient reported outcome measures (PROMs) is lacking.
Day 2 of #UAA2017
After early showers on day 2 of UAA, Hong Kong was heating up with temperatures over 33 degrees Celsius. So were the discussions in the plenary session in the morning. Professor Freddie Hamdy (@Freddie_Hamdy) gave the #EAU lecture on #activesurveillance for #prostatecancer. This was followed on nicely with the current status of #prostatecancer management in Hong Kong by Dr. Yau-Tung Chan and Dr. Gerhardt Attard (UK) enlightened the audience with a concise update in the management of hormone sensitive prostate cancer, an area where the landscape is ever-changing.
The advanced oncology session started off with a heated debate in the use of mass clamping (Dr Ringo Chu, Hong Kong) versus selective artery clamping in partial nephrectomy (Dr Tae-Gyun Kwon, Korea). Both speakers presented with very valid arguments and perhaps it was fair to say it ended up with all square. Professor Krishna Sethia (UK) gave a fascinating summary of the current local management of #penilecancer at centralised penile cancer centres in the UK, after which I was honoured to provide an update on current nodal management in #penilecancer from my recent experience at St George’s University Hospitals @StGeorgesTrust in the UK. It was exciting to see the centralisation of services in #penilecancer in the UK has given great opportunities to understand and optimise management of patients with such rare disease.
The Semi-live sessions entertained the audience on both days of the conference. Excellent videos were presented throughout. Professor Koon Rha of Yonsei University in South Korea gave a fantastic semi-live talk on his tricks and techniques of Retzius-space sparing Robot-assisted radical prostatectomy. Perhaps what’s even more exciting to know is that a Korean company has produced a new robot for surgery which has been well tested by Professor Rha’s group, which has just literally been licenced and approved in Korea just days before #UAA2017. Will this finally drive the cost of robotic surgery down? Time will tell.

Associate Professor Declan Murphy (@declanmurphy) and Mr. Rajesh Nair (@nairajesh) both contributed with a beautiful video showcasing techniques in total pelvic exenteration and long-term outcomes of urinary diversion and reconstruction in this cohort of patients.
The Gala dinner in the evening was full of fun and entertainment. Following the performance of a soprano quartet formed by local Hong Kong urologists (who sang the classic My Way with a twist on prostate examination!), the rock stars of urology – Professor Jens Rassweiller, Dr Samuel Yee from Hong Kong, and Dr Domenico Veneziano (@d_veneziano) provided an energetic and electrifying live performance of some rock classics!

Urology Rock N’ Roll! Left to right: Professor Jens Rassweiller (Germany), Dr Domenico Veneziano (Italy), Dr Samuel Yee (Hong Kong).
However, perhaps the highlight and the most touching moment of the evening the performance of a song written and sung by a young local former patient with a history of #ketaminebladder , who was successfully treated by the urology team lead by Professor Anthony Ng at the Prince of Wales Hospital in Hong Kong. His surgery and treatment has transformed his life – he is now enjoying a career as both a singer-songwriter of a rock band and as a footballer!
Day 3 of #UAA2017
The morning plenary session also saw the evergreen Dr Peggy Chu of Hong Kong, renown for her discovery of ketamine-associated uropathy and pioneered the management of this challenging 21st century urological disease.

Left to right: Dr CW Man (Hong Kong), Congress President of #UAA2017, and Dr Peggy Chu (Hong Kong).
She delivered a very interesting talk on revisiting the role of #gastrocystoplasty. Interestingly, the operation was first described and carried out in human by the honourable Professor CH Leong at my current institution, Queen Mary Hospital @HKUniversity , in the 1970s following a successful animal study at the same institution. Its use has been limited due to its associated metabolic disturbances, but arguably it is still a weapon that can be used when tackling patients with tuberculosis-associated severely contracted bladder, in particular those who have already been rendered to have a single solitary kidney due to the disease. Another situation when #gastrocystoplasty can still be considered are those patients with #ketamine uropathy. Although patients are usually required to be completely abstinence from #ketamine abuse for a certain lengthy period of time before they are eligible for surgical treatment, many fear the avalanche effect of ileal re-absorption of the drug if an ileo-cystoplasty has been carried out in these patients, if they happen to resume ketamine use in the future. Hence, #gastrocystoplasty may be a better substitution tissue for cystoplasty in the management of such patients.
The meeting also provided an opportunity to catch up with fellow Guy’s Hospital urology graduates @nairajesh and @declanmurphy over a cold pint of Hong Kong locally made #MoonzenBeer, when the temperature outside the conference centre was hitting 34 degrees Celsius!

Left to right: Dr Wayne Lam (Hong Kong), Mr Rajesh Nair (Australia/United Kingdom), A/Prof Declan Murphy (Australia).
All credits to #UAA and the local organisers’ immense effort and hard work, making this congress a valuable learning experience for everyone who participated. We very much look forward to #UAA2018. Bring on Kyoto, Japan!
Wayne Lam
Assistant Professor in Urology, Queen Mary Hospital, University of Hong Kong
Twitter: @WayneLam_Urol
Rajesh Nair
Fellow in Robotic Surgery and Uro-Oncology

Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there are accompanying editorials written by prominent members of the urological community. These blogs are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video discussing the paper.
If you only have time to read one article this week, it should be this one.
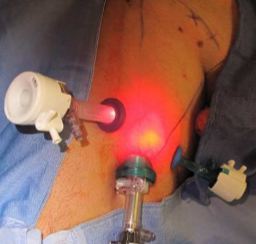
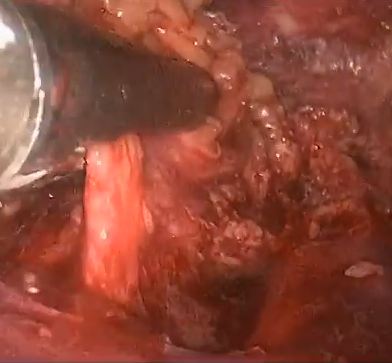
Kumar, V. and Sethia, K. K. (2017), Prospective study comparing video-endoscopic radical inguinal lymph node dissection (VEILND) with open radical ILND (OILND) for penile cancer over an 8-year period. BJU International, 119: 530–534. doi: 10.1111/bju.13660
To compare the complications and oncological outcomes between video-endoscopic inguinal lymph node dissection (VEILND) and open ILND (OILND) in men with carcinoma of the penis.
A prospectively collected institutional database was used to determine the outcomes in 42 consecutive patients undergoing ILND between 2008 and 2015 in a centre for treating penile cancer. Before 2013 all procedures were OILNDs. Since 2013 we have performed VEILND on all patients in need of ILND. The wound-related and non-wound-related complications, length of stay, and oncological safety between OILND and VEILND groups were compared. The mean duration of follow-up was 71 months for OILND and 16 months for the VEILND groups.
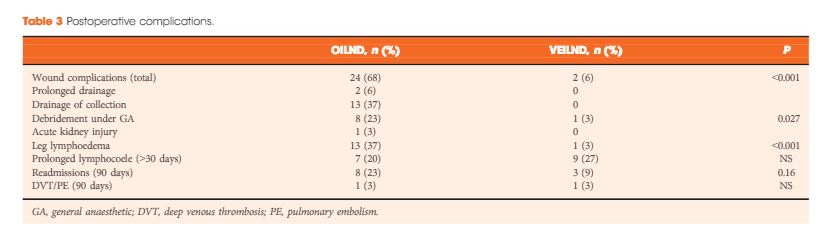
In the study period 42 patients underwent 68 ILNDs (OILND 35, VEILND 33). The patients’ demographics, primary stage and grade, and indications were comparable in both groups. There were no intraoperative complications in either group. The wound complication rate was significantly lower in the VEILND group at 6% compared to 68% in the OILND group. Lymphocoele rates were similar in both the groups (27% and 20%). The VEILND group had a better or the same lymph node yield, mean number of positive lymph nodes, and lymph node density confirming oncological safety. There were no groin recurrences in either group of patients. VEILND significantly reduced the mean length of stay by 4.8 days (P < 0.001).
VEILND is an oncologically safe procedure with considerably low morbidity and reduced length of stay, at a mean (range) follow-up of 16 (4–35) months.
In this interesting prospective study, Kumar and Sethia [1] provide further evidence that video endoscopic inguinal lymphadenectomy (VEIL) could be considered the procedure of choice for most patients with an indication for ILND. In their comparison with historical patients submitted to open ILND (OILND) in a reference centre in the UK, VEIL achieved reduced morbidity, shorter hospital stay, and equivalent oncological control. Also, we must consider that some cases of the VEIL learning curve were included in this study, suggesting that good results can be obtained with the endoscopic technique from its inception.
The idea for an endoscopic approach to ILND was conceived and developed in a cadaveric model by Bishoff et al. [2] in 2003. In 2005, our group reported the first successful experience in humans [3]. In 2006, in collaboration with the Brazilian National Institute of Cancer, we published a landmark study in the Journal of Urology comparing OILND in one limb and VEIL in the contralateral limb in the same patient to minimise comparative bias [4]. In all, 10 patients with impalpable nodes underwent bilateral ILND. We found that morbidity was reduced with VEIL (20% vs 70%) with the removal of the same number of nodes as with OILND [4]. In 2008, we reported on a series of bilateral VEIL obtaining reduced postoperative morbidity and a mean hospital stay of 1 day [5]. Several other small series have reported essentially the same results that we initially described.
Robot-assisted VEIL duplicates the procedure but is more ergonomic, with excellent freedom of movement and amplification of lymphatic visualisation. Matin et al. [6] reported that robot-assisted VEIL could remove the same number of nodes as the open procedure.
The present study [1] reports a large experience comparing bilateral procedures (VEIL and OILND). The follow-up data for OILND are longer but oncological indicators suggest equivalence. This is also the first report of VEIL after node cytology and dynamic sentinel node biopsy with no related adverse events.
To date, a few series have reported long-term oncological results [1, 7] and future studies will be important to evaluate and reproduce the oncological efficacy of VEIL.
We congratulate Kumar and Sethia [1] for these significant data to establish VEIL in the modern urological armamentarium. Indeed, I really have some doubt as whether a randomised controlled study would be necessary considering the accumulated worldwide data on VEIL in the last 10 years.
This year we present at the University of California meeting the promising results of our Latin America collaborative group with 150 VEIL in 110 patients. The mean (range) follow up was 6 (2–10) years, with an overall morbidity of 30% (Clavien–Dindo grade III–IV, 2%), mean lymph node removal of 8 nodes/groin, node positive disease rate of 25%, inguinal recurrence rate of 2%, cancer-specific survival of 90%, and overall survival of 85% (Tobias-Machado et al., 2016, unpublished data). Our data suggest that we can obtain a dramatic reduction in severe complications and also that VEIL is surviving the test of time.
In my opinion, as the reduction in morbidity is already confirmed, we only need larger series with long-term reports of oncological equivalence with OILND to designate VEIL as a ‘gold standard’ in centres with appropriately trained surgeons.
I speculate that in the near future the utilisation of robotic surgery associated with improvements in imaging methods and contrasts, which will improve the identification of lymph nodes to be removed and lymphatic channels to be clipped, will achieve further reductions in morbidity and optimisation of oncological control.
Tobias-Machado, M. (2017), Video endoscopic inguinal lymphadenectomy (VEIL): is a new standard ready to be accepted?. BJU International, 119: 504–505. doi: 10.1111/bju.13723
In this issue of BJUI, Kumar and Sethia report their experience of laparoscopic inguinal node dissection for patients with penile cancer [1]. The authors should be congratulated for what is a technically and feasibly difficult study to complete.
The step-wise spread of penile carcinoma first to the inguinal lymph nodes is well known. It is also recognized that accurate staging and treatment of inguinal metastases play a crucial part in a patient’s management pathway. Furthermore, evidence points to a survival advantage for those who undergo prophylactic inguinal lymph node dissection (ILND) and have positive nodes, compared with those treated with surveillance and delayed dissection when nodes become palpable or radiologically positive.
The overall postoperative complication rate after ILND has been reported to be nearly 50% or even up to 75%. Patients with comorbidities or locally advanced disease are at particular risk of postoperative morbidity [2]. High rates of wound dehiscence and skin necrosis after ILND have also been reported [3]. More recently, complication rates among men with no palpable adenopathy have been reported to be decreasing in comparison with historical experience, but overall complication rates still range from 10 to 40%.
Adoption of dynamic sentinel node biopsy has reduced the absolute number of prophylactic ILNDs, but in any high-volume unit (as is the case in the UK supra-network centres), a large number of inguinal node dissections will still be undertaken [4].
For these reasons it is desirable to minimize or modify the inguinal wound to reduce the complication rate, and the use of minimally invasive techniques has gradually progressed over the last 10 years.
The first case series reporting the use of laparoscopic node dissection (videoendoscopic inguinal node dissection [VEILND]) described 10 patients who underwent bilateral ILND using standard lymphadenectomy on one side and the VEILND technique on the contralateral side [5]. A more recent development has been the incorporation of robotic assistance as an enabling tool for performing ILND [6].
In these small series the technique appeared to be safe and oncologically comparable to open surgery, but the numbers were too small to give a meaningful assessment of complications. It is therefore welcome to read a paper on a high-volume unit’s experience of VEILND.
The authors describe their experience of VEILND on a sequential prospective group of patients and compared them with a historical control cohort who underwent open inguinal node dissection. The data appear to show a significant difference in length of stay and wound-related comorbidity in favour of the minimally invasive approach without compromising oncological outcome. Interestingly, the rate of lower limb lymphedema was also significantly reduced in the VEILND group.
The headline data are impressive but the comparison does have a number of potential weaknesses. Firstly, the rate of wound-related complications is quite high in the open group, with 23% of patients needing re-exploration or debridement and 37% some form of drainage of collection. The choice of incision position, length and preparation of skin flaps can influence the rate of wound breakdown and length of stay.
Secondly, the headline 6% complication rate for VEILND does not include the 27% lymphocoele rate which is still a troublesome complication in both the open and endoscopic groups.
Finally, there is no mention of the limitations of the technique with size and extent of the malignant node burden. The paper states that all patients were included, and yet in any high-volume centre there must be patients with grossly enlarged and sometimes fungating or fixed nodes and I would have thought that VEILND would not be appropriate in these instances.
In conclusion, there is much to commend this paper and the direction of travel may well be towards minimally invasive techniques; however, as with all comparisons between open and keyhole surgery, the focus should be on improving the open technique to its limit. Only then will the results be meaningful and adopted with confidence.
Watkin, N. (2017), Is minimally invasive inguinal node dissection the way forward?. BJU International, 119: 505–506. doi: 10.1111/bju.13761
To compare the complications and oncological outcomes between video-endoscopic inguinal lymph node dissection (VEILND) and open ILND (OILND) in men with carcinoma of the penis.
A prospectively collected institutional database was used to determine the outcomes in 42 consecutive patients undergoing ILND between 2008 and 2015 in a centre for treating penile cancer. Before 2013 all procedures were OILNDs. Since 2013 we have performed VEILND on all patients in need of ILND. The wound-related and non-wound-related complications, length of stay, and oncological safety between OILND and VEILND groups were compared. The mean duration of follow-up was 71 months for OILND and 16 months for the VEILND groups.
In the study period 42 patients underwent 68 ILNDs (OILND 35, VEILND 33). The patients’ demographics, primary stage and grade, and indications were comparable in both groups. There were no intraoperative complications in either group. The wound complication rate was significantly lower in the VEILND group at 6% compared to 68% in the OILND group. Lymphocoele rates were similar in both the groups (27% and 20%). The VEILND group had a better or the same lymph node yield, mean number of positive lymph nodes, and lymph node density confirming oncological safety. There were no groin recurrences in either group of patients. VEILND significantly reduced the mean length of stay by 4.8 days (P < 0.001).
VEILND is an oncologically safe procedure with considerably low morbidity and reduced length of stay, at a mean (range) follow-up of 16 (4–35) months.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
To determine the outcome of clinically negative node (cN0) patients with penile cancer undergoing dynamic sentinel node biopsy (DSNB), comparing the results of a 1- and 2-day protocol that can be used as a minimal invasive procedure for staging of penile cancer.
This is a retrospective analysis of 151 cN0 patients who underwent DSNB from 2008 to 2013 for newly diagnosed penile cancer. Data were analysed per groin and separated into groups according to the protocol followed. The comparison of the two protocols involved the number of nodes excised, γ-counts, false-negative rates (FNR), and complication rates (Clavien–Dindo grading system).
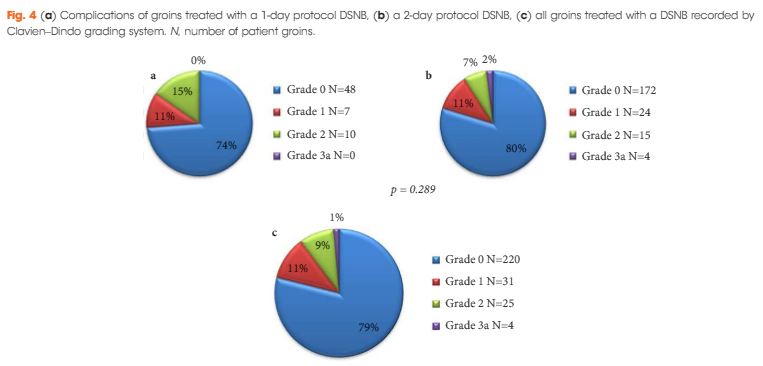
In all, 280 groins from 151 patients underwent DSNB after a negative ultrasound ± fine-needle aspiration cytology. The 1-day protocol was performed in 65 groins and the 2-day protocol in 215. Statistically significantly more nodes were harvested with the 1-day protocol (1.92/groin) compared with the 2-day protocol (1.60/groin). The FNRs were 0%, 6.8% and 5.1%, for the 1-day protocol, 2-day protocol, and overall, respectively. Morbidity of the DSNB was 21.4% for all groins, and 26.2% and 20.1% for the 1-day and 2-day protocols, respectively. Most of the complications were of Clavien–Dindo Grade 1–2.
DSNB is safe for staging patients with penile cancer. There is a trend towards a 1-day protocol having a lower FNR than a 2-day protocol, albeit at the expense of a slightly higher complication rate.
The present article by Dimopoulos et al. [1] has some useful lessons on the development of new services. The authors have kept a detailed database of all patients going through their super-regional network, and have designed the protocol around the patient, whereby the primary and regional lymph nodes are dealt with in one visit. Previously, bilateral inguinal lymph node dissection (ILND) was so fraught with complications that it would not be combined routinely with organ-sparing surgery of the penis [2]; however, the significantly lower complication rate of dynamic sentinel node biopsy (DSNB) has allowed the more streamlined approach. The ‘only handle it once’ (OHIO) philosophy is surely not only preferable for the patient, but also reduces the risk of patients not receiving ideal management. In most cases, a biopsy at the time of presentation, along with physical examination/imaging, can determine those requiring DSNB instead of waiting for final pathology from the primary tumour. The controversy surrounding DSNB compared with ILND has been the false-negative rates. The pioneering group from the Netherlands reported four deaths in six patients with false-negative results [3]. In the present paper, the overall false-negative rate was 5.8%, but the smaller and newer cohort of patients underwent a same-day protocol and had zero false-negatives. This may be attributable to the fact that biopsies were taken from a total sample of 65 or that slightly more nodes were taken in this group. We expect the one-day protocol to become standard, and future independent reports will be welcome. Should there truly be a 0% false-negative rate then the controversy is resolved and prophylactic ILND will become a historical procedure. Finally, the lower morbidity of the present study cohort allowed the authors to move the intermediate-risk group from surveillance to nodal biopsy, which proved justified because some of these cases had micrometastatic disease. We congratulate the group for their scientific approach to improving the quality of care for patients and for bringing their data to publication.