What’s the Diagnosis?
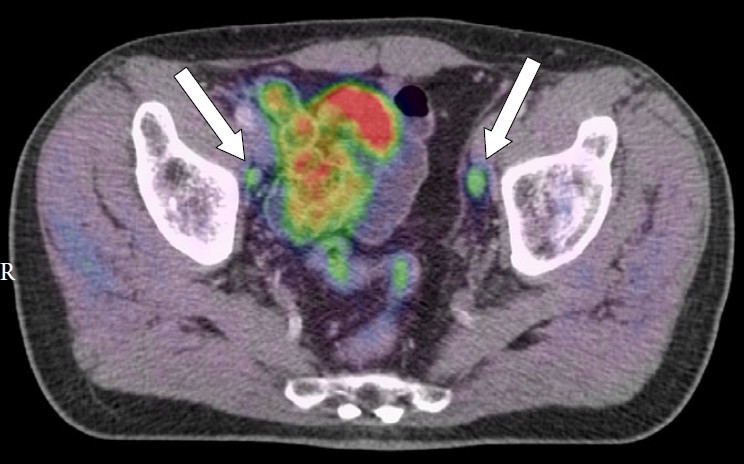
This man has intermediate/ high-risk prostate cancer.
Taken from Daouacher et al, BJUI 2016
No such quiz/survey/poll
This man has intermediate/ high-risk prostate cancer.
Taken from Daouacher et al, BJUI 2016
No such quiz/survey/poll
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Stefan Carlsson, Dr. Anna Wallerstedt and Dr Rodolfo Sanchez, discussing their paper.
If you only have time to read one article this week, it should be this one.

To analyse oncological and functional outcomes 12 months after treatment of very-low-risk prostate cancer with radical prostatectomy in men who could have been candidates for active surveillance.
We conducted a prospective study of all men with very-low-risk prostate cancer who underwent radical prostatectomy at one of 14 participating centres. Validated patient questionnaires were collected at baseline and after 12 months by independent healthcare researchers. Biochemical recurrence (BCR) was defined as prostate-specific antigen (PSA) ≥0.25 ng/mL or treatment with salvage radiotherapy or with hormones. Urinary continence was defined as <1 pad changed per 24 h. Erectile function was defined as ability to achieve erection hard enough for penetration more than half of the time after sexual stimulation. Changes in tumour grade and stage were obtained from pathology reports. We report descriptive frequencies and proportions of men who had each outcome in various subgroups. Fisher’s exact test was used to assess differences between the age groups.
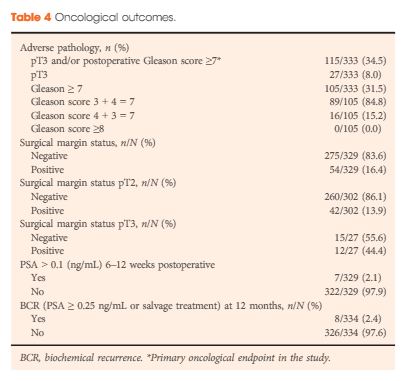
Of the 4003 men in the LAPPRO cohort, 338 men fulfilled the preoperative national criteria for very-low-risk prostate cancer. Adverse pathology outcomes included upgrading, defined as pT3 or postoperative Gleason sum ≥7, which was present in 35% of the men (115/333) and positive surgical margins, which were present in 16% of the men (54/329). Only 2.1% of the men (7/329) had a PSA concentration >0.1 ng/mL 6–12 weeks postoperatively. Erectile function and urinary continence were observed in 44% (98/222) and 84% of the men (264/315), respectively, 12 months postoperatively. The proportion of men achieving the trifecta, defined as preoperative potent and continent men who remained potent and continent with no BCR, was 38% (84/221 men) at 12 months.
Our prospective study of men with very-low-risk prostate cancer undergoing open or robot-assisted radical prostatectomy showed that there were favourable oncological outcomes in approximately two-thirds. Approximately 40% did not have surgically induced urinary incontinence or erectile dysfunction 12 months postoperatively. These results provide additional support for the use of active surveillance in men with very-low-risk prostate cancer; however, the number of men with risk of upgrading and upstaging is not negligible. Improved stratification is still urgently needed.
Prostate cancer is the most commonly diagnosed solid organ tumour and the second leading cause of cancer death in men in the USA. The exact path of these tumours from inception to metastasis is unclear; the same can also be said for those tumours that remain indolent. The varying genetic signatures of these tumours is the underlying determinant of the outcomes of these cancers and therein lies the key to selecting patients that do and do not need treatment for their prostate cancers. Most low-risk tumours are relatively indolent; however, some low-risk tumours have the potential to metastasise and cause mortality. The problem is that currently we do not have the ability to accurately and confidently determine the tumour’s individual risk profiles.
In the recent LAPPRO trial (LAParoscopic Prostatectomy Robot Open – a randomised, open trial of radical prostatectomy (RP) with or without lymph node dissection as part of a prospective, non-randomised, open trial comparing robot-assisted laparoscopic and open RP), the authors reported the RP results of patients with very-low-risk prostate cancer in a population-based study from Sweden compiling the results of open and laparoscopic RP over 14 centres of varying experience [1]. They reported pathological upgrading in 35% of patients and PSA recurrence in 2.1%. Functional outcomes at 1 year featured urinary continence levels of 84% and sexual potency of 44%. The overall trifecta rate at 1 year was 38%. What is important to note is that only 56% had optimal erectile function preoperatively (Sexual Health Inventory for Men score >21) and that it is unknown which patients received a full nerve preservation. Also the amount of postoperative continence and potency rehabilitation is unknown.
The results of the LAPPRO trial are not too dissimilar to data from the Medicare database publications on RP, which also take into account large populations of patients operated on at multiple institutions with variable surgical experience and volume [2]. The challenge with interpreting these data is that they often are quite variable based upon the preoperative status of the patient, type of surgery performed, surgeon experience, and institutional volumes [3]. If you compare the Medicare data or LAPPRO trial outcomes to large-volume single-surgeon series you often will see wide variances in outcomes favouring the single-surgeon experience. Single-surgeon and large-volume series have reported better outcomes often due to improved surgical experience, techniques, and outcomes overall [4].
Active surveillance is usually the primary choice for management of low- and very-low-risk prostate cancer lesions. However, some patients do still chose to undergo surgery due to personal choice, often related to the uncertainty associated with the diagnosis and the unknown risk of progression [5]. One would assume that low-risk tumours have a low risk of progression and metastasis; however, this is not always the case due to the varying genetic signature of the individual tumours. Also, recent studies have shown that in patients diagnosed with low-risk prostate cancer 30–50% have non-low-risk disease harbouring intermediate- or high-risk prostate cancer instead [1, 6]. This uncertainty on the part of the patient and physician can cause anxiety in patients and sometime influence their decision for treatment [7].
One would assume that patients with low- and very-low-risk patients are ideal candidates for the trifecta due to low tumour aggressiveness and volume. However, many factors influence patient outcome beyond the characteristics of the tumour. Preoperative features such as co-morbidities and pre-existing sexual dysfunction or incontinence are influential. Operative and postoperative factors include: surgeon experience, institutional volume, patients body habitus, number of prior biopsies, the ability to fully spare the nerves, and various other challenges during surgery. These are all variables that must be considered when projecting the success of surgical intervention.
While the results of surgery in the LAPPRO trial were not encouraging for surgery, we do have to take the results in context and not apply them broadly or globally without some thought. The results are blurred by combining open and laparoscopic RP, many patients were not optimal candidates’ preoperatively for the trifecta, many did not have a full nerve preservation and also many different institutions with varying levels of surgeon experience are analysed. This population was also ‘captive’, as they had to choose surgeons in their own locality, these ‘local’ surgeons may not have had the necessary experience or technique to achieve optimal outcomes. The conclusion that can be drawn is that if you sample a broad population of surgeons then the results are often quite poor due to the varying levels of skill of the surgeon and the varying level of surgical volume and experience. What the patients should glean from this is the fact that they should consider active surveillance for these types of tumours to avoid the associated morbidity. In addition, if they were to seek therapy they should select centres with higher surgical experience and proven outcomes.
For those patients that have low-risk tumours and seek treatment; judicious counselling of expectations must be performed by their healthcare advocate. Both the patient and physician must take the responsibility in making the correct assumptions and decisions. The physician must re-emphasise the available data and the low likelihood of progression in these tumours adding some caution from the fact that some of these may be upgraded. Patients must be given accurate data in the correct context. Most patients who have treatment for prostate cancer whether it be radiation, ablation or removal have a high chance of some deficit in the quality of life, functional recovery of urinary continence, and sexual potency. Educating the patient and managing realistic expectations is often the most important factor in patient satisfaction. Patients must take into account their own preoperative medical and functional status to properly stratify expectations.
If these patients after appropriate counselling are still intent to undergo surgery they should consider seeking centres with high-volume and individualised surgeons with proven quality outcomes. Large-volume single-surgeon series do show improvements in the trifecta outcomes [4]. However, none have shown perfect trifecta rates. No matter what method of treatment patients chose there would be some varying level of loss of functional outcome. The balance between cancer progression and quality of life must be weighted. For low-risk patients, we need to have a better road map of the genetic signatures of their tumour and only then will we be able to confidently tell our patients who will and who will not have the potential to harbour high-risk disease and potentially have mortality from the tumour. Until we are able to confidently deliver this information to the patient, many with low-risk disease will still seek treatment and endanger their quality of life. The recent increase in the availability of biomarkers to examine prostate biopsy specimens for risk stratification is encouraging, yet still in its infancy. Further study of these biomarkers will enhance our ability to read the genetic signature of prostate cancers at an early state and more appropriately risks stratify our patients.
The LAPPRO trial supports active surveillance as the primary choice for low- and very-low-risk tumours. However, their results are exclusive to their patient population and level of surgical experience. A similar trial with a high-volume experienced surgeon would undoubtedly show more optimistic results. Managing reasonable expectations, risk stratification, and picking expertise and experience, often makes the difference between a good and poor outcome.

To analyse oncological and functional outcomes 12 months after treatment of very-low-risk prostate cancer with radical prostatectomy in men who could have been candidates for active surveillance.
We conducted a prospective study of all men with very-low-risk prostate cancer who underwent radical prostatectomy at one of 14 participating centres. Validated patient questionnaires were collected at baseline and after 12 months by independent healthcare researchers. Biochemical recurrence (BCR) was defined as prostate-specific antigen (PSA) ≥0.25 ng/mL or treatment with salvage radiotherapy or with hormones. Urinary continence was defined as <1 pad changed per 24 h. Erectile function was defined as ability to achieve erection hard enough for penetration more than half of the time after sexual stimulation. Changes in tumour grade and stage were obtained from pathology reports. We report descriptive frequencies and proportions of men who had each outcome in various subgroups. Fisher’s exact test was used to assess differences between the age groups.
Of the 4003 men in the LAPPRO cohort, 338 men fulfilled the preoperative national criteria for very-low-risk prostate cancer. Adverse pathology outcomes included upgrading, defined as pT3 or postoperative Gleason sum ≥7, which was present in 35% of the men (115/333) and positive surgical margins, which were present in 16% of the men (54/329). Only 2.1% of the men (7/329) had a PSA concentration >0.1 ng/mL 6–12 weeks postoperatively. Erectile function and urinary continence were observed in 44% (98/222) and 84% of the men (264/315), respectively, 12 months postoperatively. The proportion of men achieving the trifecta, defined as preoperative potent and continent men who remained potent and continent with no BCR, was 38% (84/221 men) at 12 months.
Our prospective study of men with very-low-risk prostate cancer undergoing open or robot-assisted radical prostatectomy showed that there were favourable oncological outcomes in approximately two-thirds. Approximately 40% did not have surgically induced urinary incontinence or erectile dysfunction 12 months postoperatively. These results provide additional support for the use of active surveillance in men with very-low-risk prostate cancer; however, the number of men with risk of upgrading and upstaging is not negligible. Improved stratification is still urgently needed.
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Angelika Borkowetz, discussing her paper.
If you only have time to read one article this week, it should be this one.
To compare multiparametric magnetic resonance imaging (mpMRI) of the prostate and histological findings of both targeted MRI/ultrasonography-fusion prostate biopsy (PBx) and systematic PBx with final histology of the radical prostatectomy (RP) specimen.
A total of 105 patients with prostate cancer (PCa) histopathologically proven using a combination of fusion Pbx and systematic PBx, who underwent RP, were investigated. All patients had been examined using mpMRI, applying the European Society of Urogenital Radiology criteria. Histological findings from the RP specimen were compared with those from the PBx. Whole-mount RP specimen and mpMRI results were directly compared by a uro-pathologist and a uro-radiologist in step-section analysis.
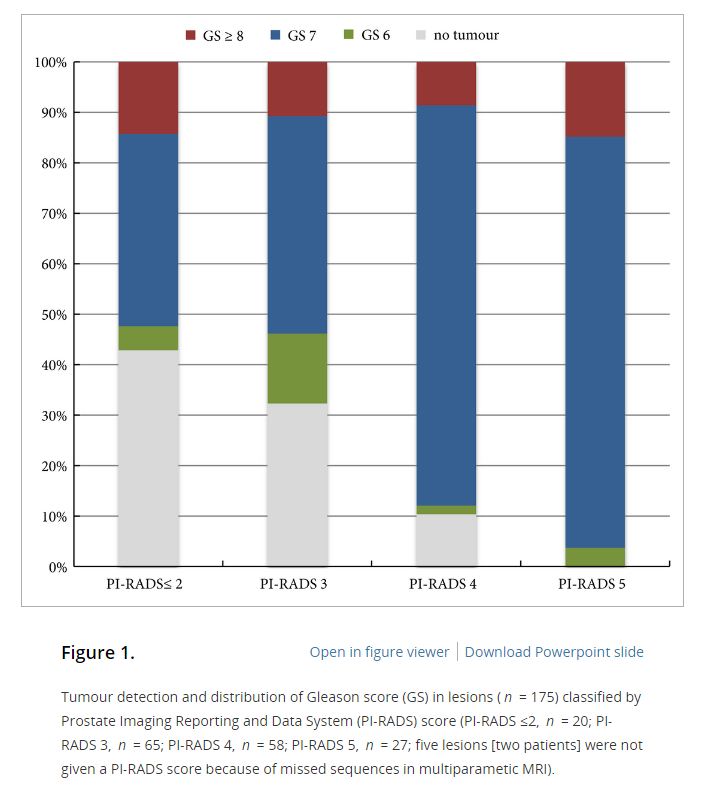
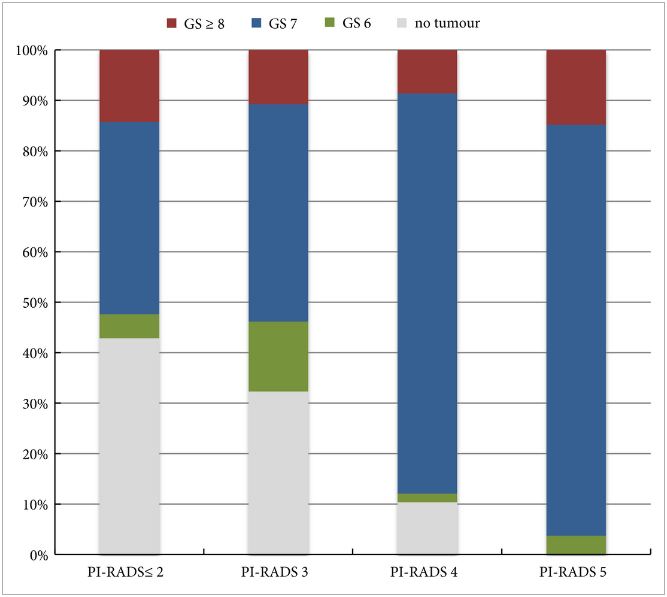
In the 105 patients with histopathologically proven PCa by combination of fusion PBx and systematic PBx, the detection rate of PCa was 90% (94/105) in fusion PBx alone and 68% (72/105) in systematic PBx alone (P = 0.001). The combination PBx detected 23 (22%) Gleason score (GS) 6, 69 (66%) GS 7 and 13 (12%) GS ≥8 tumours. Fusion PBx alone detected 25 (26%) GS 6, 57 (61%) GS 7 and 12 (13%) GS ≥8 tumours. Systematic PBx alone detected 17 (24%) GS 6, 49 (68%) GS 7 and 6 (8%) GS ≥8 tumours. Fusion PBx alone would have missed 11 tumours (4% [4/105] of GS 6, 6% [6/105] of GS 7 and 1% [1/105] of GS ≥8 tumours). Systematic PBx alone would have missed 33 tumours (10% [10/105] of GS 6, 20% [21/105] of GS 7 and 2% [2/105] of GS ≥8 tumours). The rates of concordance with regard to GS between the PBx and RP specimen were 63% (n = 65), 54% (n = 56) and 75% (n = 78) in fusion, systematic and combination PBx (fusion and systematic PBx combined), respectively. Upgrading of the GS between PBx and RP specimen occurred in 33% (n = 34), 44% (n = 46) and 18% (n = 19) in fusion, systematic and combination PBx, respectively. γ-correlation for detection of any cancer was 0.76 for combination PBx, 0.68 for fusion PBx alone and 0.23 for systematic PBx alone. In all, 84% (n = 88) of index tumours were identified by mpMRI; 86% (n = 91) of index lesions on the mpMRI were proven in the RP specimen.
Fusion PBx of tumour-suspicious lesions on mpMRI was associated with a higher detection rate of more aggressive PCa and a better tumour prediction in final histopathology than systematic PBx alone; however, combination PBx had the best concordance for the prediction of GS. Furthermore, the additional findings of systematic PBx reflect the multifocality of PCa, therefore, the combination of both biopsy methods would still represent the best approach for the prediction of the final tumour grading in PCa.
The success of multiparametric MRI (mpMRI) and MRI/ultrasound (US) fusion-guided biopsies in improving the detection of prostate cancer in patients with occult disease (elevated PSA level with prior negative biopsies) and optimising the detection of clinically significant cancer has been reported by centres that have served as early adopters of these techniques [1, 2]. Technological advances in MRI and associated imaging protocols, as well as increased clinical experience with MRI interpretation have led to increased prospective detection and characterisation of clinically significant prostate cancer. This, in conjunction with increasing experience with MRI/US fusion-guided prostate biopsy techniques, has led to the re-evaluation of the contributory role and utility of systematic template US-guided prostate biopsies in the diagnosis of prostate cancer. It is an attractive proposition to forego the systematic biopsy when performing MRI-directed fusion biopsy, as this would minimise the duration, morbidity, and overall cost of the biopsy procedure and post-biopsy pathology processing. However, before adopting this approach, it is important to first consider the potential possibility of missing clinically significant cancer diagnoses when relying on the targeted biopsy cores in isolation.
In this issue of BJUI, Borkowetz et al. [3] report their results of biopsy histological yields on systematic biopsies compared with MRI/US fusion biopsies in their series of patients who underwent radical prostatectomy (RP). These results corroborate previously reported comparisons of fusion biopsy of suspicious lesions on MRI performed concurrently with systematic biopsy, consistently showing an improved detection of both overall prostate cancer foci and, more importantly, an improved detection of clinically significant higher grade cancer foci [1, 2]. It is important to note that the overall detection rate and detection rate for clinically significant prostate cancer was highest when fusion and systematic biopsies were evaluated in conjunction with each other. Another important factor to consider when evaluating the utility and value of these biopsy techniques is the concordance of the pathology of the biopsy specimen with the final pathology of the RP specimen, the ‘gold standard’. The concordance of Gleason grade assigned on targeted fusion-biopsy cores and RP outperformed that of systematic biopsy cores and RP. This, in essence, suggests that targeted biopsy can perform as well, and likely better, than the systematic biopsy approach of sampling the prostate with a systematic-sextant approach, which has been the long standing standard of care for the diagnosis of prostate cancer. Again, it is important to note that the greatest concordance in this study was achieved when the results of the fusion and systematic biopsy cores were combined.
The question now arises regarding the ‘cost’ for the incremental improvement in cancer detection provided by the combination of both MRI-directed fusion biopsy and the systematic biopsy approach. The improved negative predictive value parallels the increased sensitivity for cancer detection by having a larger sampling of the prostate by augmenting the number of biopsy cores sampled and submitted for histopathological evaluation. The area under the curve for detection of clinically significant cancer reported by Borkowetz et al. [3] was not improved by adding systematic biopsies to the targeted biopsies. However, this experience described a mixed population of patients, most of whom had undergone prior prostate biopsy with benign pathology. This creates an enriched population who likely harbours prostate cancers that are more occult to the systematic biopsy approach, thus improving the diagnostic yield of MRI-directed biopsies even further. This is concordant with the work presented by Mendhiratta et al. [4], where systematic biopsies added little to the diagnosis of clinically significant prostate cancer in a population of men undergoing MRI/US fusion-guided biopsy after prior cancer-negative biopsy sessions.
Alternatively, current datasets for biopsy naïve patients have not shown the same degree of convincingly improved detection with targeted biopsies over systematic biopsies. In fact, Delongchamps et al. [5] recently reported a slightly lower rate of overall cancer detection with fusion-guided targeted biopsies vs systematic biopsy cores; however, the difference in detection of clinically significant prostate cancer was not statistically significant. Further study of the role of targeted biopsy in the biopsy naïve patient population is warranted, as there is suggestion that cancer detection efficiency per needle core is significantly improved with MRI-directed biopsies over systematic biopsies [6]. Alternatively, in patients with prior negative systematic biopsies and continued clinical suspicion for prostate cancer, a repeat biopsy session with targeted cores alone may be appropriate, particularly as these patients have previously undergone standard-of-care, extended sextant biopsy.
To compare multiparametric magnetic resonance imaging (mpMRI) of the prostate and histological findings of both targeted MRI/ultrasonography-fusion prostate biopsy (PBx) and systematic PBx with final histology of the radical prostatectomy (RP) specimen.
A total of 105 patients with prostate cancer (PCa) histopathologically proven using a combination of fusion Pbx and systematic PBx, who underwent RP, were investigated. All patients had been examined using mpMRI, applying the European Society of Urogenital Radiology criteria. Histological findings from the RP specimen were compared with those from the PBx. Whole-mount RP specimen and mpMRI results were directly compared by a uro-pathologist and a uro-radiologist in step-section analysis.
In the 105 patients with histopathologically proven PCa by combination of fusion PBx and systematic PBx, the detection rate of PCa was 90% (94/105) in fusion PBx alone and 68% (72/105) in systematic PBx alone (P = 0.001). The combination PBx detected 23 (22%) Gleason score (GS) 6, 69 (66%) GS 7 and 13 (12%) GS ≥8 tumours. Fusion PBx alone detected 25 (26%) GS 6, 57 (61%) GS 7 and 12 (13%) GS ≥8 tumours. Systematic PBx alone detected 17 (24%) GS 6, 49 (68%) GS 7 and 6 (8%) GS ≥8 tumours. Fusion PBx alone would have missed 11 tumours (4% [4/105] of GS 6, 6% [6/105] of GS 7 and 1% [1/105] of GS ≥8 tumours). Systematic PBx alone would have missed 33 tumours (10% [10/105] of GS 6, 20% [21/105] of GS 7 and 2% [2/105] of GS ≥8 tumours). The rates of concordance with regard to GS between the PBx and RP specimen were 63% (n = 65), 54% (n = 56) and 75% (n = 78) in fusion, systematic and combination PBx (fusion and systematic PBx combined), respectively. Upgrading of the GS between PBx and RP specimen occurred in 33% (n = 34), 44% (n = 46) and 18% (n = 19) in fusion, systematic and combination PBx, respectively. γ-correlation for detection of any cancer was 0.76 for combination PBx, 0.68 for fusion PBx alone and 0.23 for systematic PBx alone. In all, 84% (n = 88) of index tumours were identified by mpMRI; 86% (n = 91) of index lesions on the mpMRI were proven in the RP specimen.
Fusion PBx of tumour-suspicious lesions on mpMRI was associated with a higher detection rate of more aggressive PCa and a better tumour prediction in final histopathology than systematic PBx alone; however, combination PBx had the best concordance for the prediction of GS. Furthermore, the additional findings of systematic PBx reflect the multifocality of PCa, therefore, the combination of both biopsy methods would still represent the best approach for the prediction of the final tumour grading in PCa.

Here it is, the highly anticipated randomised controlled trial of open versus robotic radical prostatectomy published today in The Lancet. Congratulations to the team at Royal Brisbane Hospital for completing this landmark study.
The early headlines around the world include everything from this one in the Australian Financial Review:
 – to this from The Telegraph in London
– to this from The Telegraph in London
 As ever, there will be intense and polarising discussion around this. One might expect that a randomised controlled trial, a true rarity in surgical practice, might settle the debate here; however, it is already clear that there will be anything BUT agreement on the findings of this study. Why is this so? Well let’s look first at what was reported today.
As ever, there will be intense and polarising discussion around this. One might expect that a randomised controlled trial, a true rarity in surgical practice, might settle the debate here; however, it is already clear that there will be anything BUT agreement on the findings of this study. Why is this so? Well let’s look first at what was reported today.
This is a prospective randomised trial of patients undergoing radical prostatectomy for localised prostate cancer. Patients were randomised to undergo either open radical prostatectomy (ORP, n=163) or robotic-assisted radical prostatectomy (RARP, n=163). All ORPs were done by one surgeon, Dr John Yaxley (JY), and all RARPs were done by Dr Geoff Coughlin (GC). The hypothesis was that patients undergoing RARP would have better functional outcomes at 12 weeks, as measured by validated patient-reported quality of life measures. Other endpoints included positive surgical margins and complications, as well as time to return to work.
So what did they find? In summary, the authors report no difference in urinary and sexual function at 12 weeks. There was also no statistical difference in positive surgical margins. RARP patients had a shorter hospital stay (1.5 vs 3.2days, p<0.0001) and less blood loss (443 vs 1338ml, P<0.001), and less pain post-operatively, yet, these benefits of minimally-invasive surgery did not translate into an earlier return to work. The average time to return to work in both arms was 6 weeks.
The authors therefore conclude by encouraging patients “to choose an experienced surgeon they trust and with whom they have a rapport, rather than choose a specific surgical approach”. Fair enough.
In summary therefore, this is a randomised controlled trial of ORP vs RARP showing no difference in the primary outcome. One might reasonably expect that we might start moth-balling these expensive machines and start picking up our old open surgery instruments. But that won’t happen, and my prediction is that this study will be severely criticized for elements of its design that explain why they failed to meet their primary endpoint.
1. Was this a realistic hypothesis? No it was not. For those of us who work full-time in prostate cancer, the notion that there would be a difference in sexual and urinary function at 12 weeks following ORP or RARP is fanciful. It is almost like it was set up to fail. There was no pilot study data to encourage such a hypothesis, and it remains a mystery to me why the authors thought this study might ever meet this endpoint. I hate to say “I told you so”, but this hypothesis could never have been proved with this study design.
2. There is a gulf in surgical experience between the two arms. The lack of equipoise between the intervention arms is startling, and of itself, fully explains the failure of this study to meet its endpoints. I should state here that both surgeons in this study, JY (“Yax”) and GC (“Cogs”), are good mates of mine, and I hold them in the highest respect for undertaking this study. However, as I have discussed with them in detail, the study design which they signed up to here does not control for the massive difference in radical prostatectomy experience that exists between them. Let’s look at this in more detail:
The whole world knows that surgeon experience is the single most important determinant of outcomes following radical prostatectomy, and much data exists to support this fact. In the accompanying editorial, Lord Darzi reminds us that the learning curve for functional and oncological outcomes following RARP extends up to 700 cases. Yes 700 cases of RARP!! And GC had done 200 radical prostatectomies prior to operating on the first patient in this study. Meanwhile his vastly more experienced colleague JY, had done over 1500 cases. The authors believe that they controlled for surgeon heterogeneity based on the entry numbers detailed above, and state that it is “unlikely that a learning curve contributed substantially to the results”. This is bunkum. It just doesn’t stack up, and none of us who perform this type of surgery would accept that there is not a clinically meaningful difference in the experience of a surgeon who has performed 200 radical prostatectomies, compared with one who has performed 1500. Therein lies the fundamental weakness of this study, and the reason why it will be severely criticized. It would be the equivalent of comparing 66Gy with 78Gy of radiotherapy, or 160mg enzalutamide with 40mg – the study design is simply not comparing like with like, and the issue of surgeon heterogeneity as a confounder here is not accounted for.
3. Trainee input is not controlled for – most surprisingly, the authors previously admitted that “various components of the operations are performed by trainee surgeons”. One would expect that with such concerns about surgeon heterogeneity, there should have been tighter control on this aspect of the interventions. It would have been reasonable within an RCT to reduce the heterogeneity as much as possible by sticking to the senior surgeons for all cases.
Having said all that, John and Geoff are to be congratulated for the excellent outcomes they have delivered to their patients in both arms of this study. These are excellent outcomes, highly credible, and represent, in my view, the best outcomes to be reported for patients undergoing RP in this country. We are all too familiar with completely unbelievable outcomes being reported for patients undergoing surgery/radiotherapy/HIFU etc around the world, and we have a responsibility to make sure patients have realistic expectations. John and Geoff have shown themselves to be at the top of the table reporting these credible outcomes today.
To paraphrase that classic phrase of the Clinton Presidential campaign of 1992, this study clearly demonstrates that outcomes following radical prostatectomy are about the surgeon, and not about the robot. Yet one of the co-authors, a psychologist, comments that, “at 12 weeks, these two surgical approaches yielded similar outcomes for prostate cancer patients”. Herein lies one of the classic failings of this study design, and also a failure of the investigators to fully understand the issue of surgeon heterogeneity in this study. It is not about the surgical approach, it is about the surgeon experience.
If the authors had designed a study that adequately controlled for surgeon experience, then it may have been possible for the surgical approach to be assessed with some equipoise. It is not impossible to do so, but is certainly challenging. For example a multi-centre study with multiple surgeons in each arm would have helped balance out the gulf in surgical experience in this two-surgeon study. Or at the very least, the authors should have ensured that they were comparing apples with apples by having a surgeon with in excess of 1500 RARP experience in that arm. Another approach would have been to get a surgeon with huge experience of both procedures (eg Dr Smith at Vanderbilt who has performed >3000 RARP and >3000 ORP), and to randomise patients to be operated on only by a single surgeon with such vast experience. That would have truly allowed the magnitude of the surgical approach effect to be measured, without the bias inherent in this study design.
Having outlined these issues with surgeon heterogeneity and lack of equipoise, there is another angle which my colleague Dr Daniel Moon has identified in his comments in the Australian media today and which should be considered.
Although this is a negative study which failed to meet its primary endpoints, it does demonstrate that a much less experienced surgeon can actually deliver equivalent functional and oncological outcomes to a much more experienced surgeon, by adopting a robotic approach. Furthermore, his patients get the benefits of a minimally-invasive approach as detailed in the paper. This therefore demonstrates that patients can be spared the inferior outcomes that may be delivered by less experienced surgeons while on their learning curve, and the robotic approach may therefore reduce the learning curve effect.
On that note, a point to consider would be what would JY’s outcomes have been in this study if he had 13 years and 1300 cases less experience to what he had entering this study? Would the 200 case experience-Yax have been able to match the 1500 case experience-Yax?? Surely not.
And finally, just as a footnote for readers around the world about what is actually happening on the ground following this study. During the course of this study, the ORP surgeon JY transitioned to RARP, and this is what he now offers almost exclusively to his patients. Why is that? It is because he delivers better outcomes by bringing a robotic approach to the vast surgical experience that he also brings to his practice, and which is of course the most important determinant of better outcomes.
Sadly, “Yax” and “Cogs”, the two surgeons who operated in this study, have been prevented from speaking to the media or to being quoted in or commenting on this blog, but we are looking forward to hearing from them when they present this data at the Asia-Pacific Prostate Cancer Conference in Melbourne in a few weeks.
Declan G Murphy
Associate Editor BJUI; Urologist & Director of Genitourinary Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia
Twitter: @declangmurphy
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from , discussing their paper.
If you only have time to read one article this week, it should be this one.
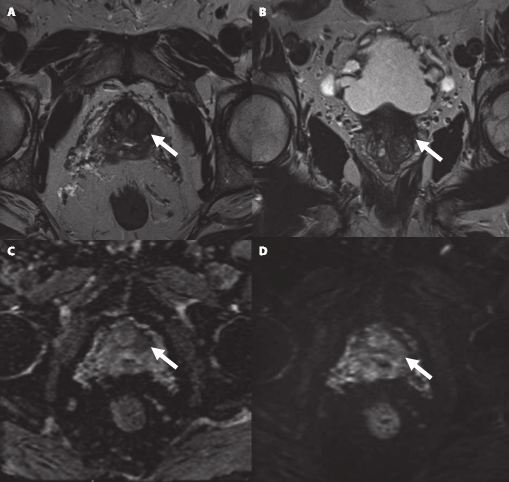
To examine the value of additional transrectal ultrasonography (TRUS)-guided random biopsy (RB) in patients with negative magnetic resonance imaging (MRI)/ultrasonography (US) fusion-guided targeted biopsy (TB) and to identify possible reasons for TB failure.
We conducted a subgroup analysis of 61 men with prostate cancer (PCa) detected by 10-core RB but with a negative TB, from a cohort of 408 men with suspicious multiparametric magnetic resonance imaging (mpMRI) between January 2012 and January 2015. A consensus re-reading of mpMRI results (using Prostate Imaging Reporting and Data System [PI-RADS] versions 1 and 2) for each suspicious lesion was performed, with the image reader blinded to the biopsy results, followed by an unblinded anatomical correlation of the lesion on mpMRI to the biopsy result. The potential reasons for TB failure were estimated for each lesion. We defined clinically significant PCa according to the Epstein criteria and stratified patients into risk groups according to the European Association of Urology guidelines.
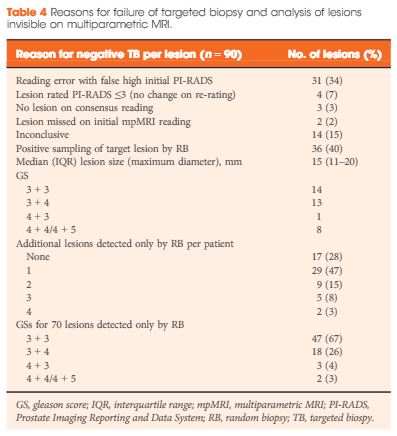
Our analysis showed that RB detected significant PCa in 64% of patients (39/61) and intermediate-/high-risk PCa in 57% of patients (35/61). The initial mpMRI reading identified 90 suspicious lesions in the cohort. Blinded consensus re-reading of the mpMRI led to PI-RADS score downgrading of 45 lesions (50%) and upgrading of 13 lesions (14%); thus, negative TB could be explained by falsely high initial PI-RADS scores for 32 lesions (34%) and sampling of the target lesion by RB in the corresponding anatomical site for 36 out of 90 lesions (40%) in 35 of 61 patients (57%). Sampling of the target lesion by RB was most likely for lesions with PI-RADS scores of 4/5 and Gleason scores (GS) of ≥7. A total of 70 PCa lesions (67% with GS 6) in 44 patients (72%) were sampled from prostatic sites with no abnormalities on mpMRI.
In cases of TB failure, RB still detected a high rate of significant PCa. The main reason for a negative TB was a TB error, compensated for by positive sampling of the target lesion by the additional RB, and the second reason for TB failure was a falsely high initial PI-RADS score. The challenges that arise for both MRI diagnostics and prostate lesion sampling are evident in our data and support the integration of RB into the TB workflow.
MRI information of the prostate is increasingly used for improving the diagnostic yield of prostate biopsies [1]. However, increasing complexity of a procedure makes it prone to errors at multiple technical and human levels. Incorporating MRI information and ultrasonography (US) images for MRI-fusion biopsies is a technically challenging task. It involves various steps such as the acquisition and fusion of MRI and US images, the needle guidance during biopsy, and the diligence of the pathological evaluation of biopsy specimens. These different steps and interfaces between different medical professions influence the diagnostic performance of MRI-fusion biopsies.
For example, in daily clinical practice, MRIs from different institutions still harbour a great variance of sequences and reporting, despite the European Society of Urogenital Urology (ESUR) recently introducing acquisition and imaging protocols and a new and advanced version of the Prostate Imaging Reporting and Data System (PIRADS) version 2.0 [2]. The usefulness of such reporting schemes is evidenced by a moderate-to-good interobserver agreement between uro-radiologists for tumour lesion interpretation and corresponding κ values ranging from 0.55 to 0.80 [3]. Important pitfalls of image interpretation are benign lesions such as prostatitis, BPH and fibrosis, which might score similarly to prostate cancer lesions. This problem is further aggravated by a high proportion of patients that receive their first multiparametric MRI (mpMRI) of the prostate in the repeat-biopsy setting with a high burden of post-biopsy artefacts (haemorrhage, capsular irregularity) and lower overall cancer detection rate. Also, during MRI-fusion biopsy patient movement, prostate deformation by the US probe, and mismatch of image planes can lead to a biopsy error exceeding 4 mm. Moreover, targeting error might be aggravated by MRI underestimation of the tumour volume compared with final pathology [4]. After various authors reported the advantages and accuracy of MRI/US-fusion biopsy approaches, Cash et al. [5] address potential reasons for targeted biopsy failure to detect prostate cancer compared with random biopsy. Within their analyses the authors address potential limitations and technical considerations. Based on different technical biopsy strategies (with the patient placed within the MRI scanner (‘in-bore’) vs outside) and different technical approaches, these considerations are very important.
In contrast to cognitive fusion, most MRI/US platforms allow needle tracking by archiving the needle orientation, either by an electromagnetic, image-based or stepper-based mechanism [1]. However, lesion targeting by needle guidance is highly dependent on the dimensions of the primary lesion, numbers of relevant lesions, localisation, and overall prostate volume, making MRI-US fusion and cognitive fusion more error prone (i.e. aiming off the mark with the needle) than in-bore biopsies. Moreover, different technical fusion approaches provide different degrees of manual/automated adjustment tools, with for example either rigid or elastic image transformation to facilitate MRI/US image alignment.
In their analyses, Cash et al. [5] found that 34% of negative targeted biopsies could be explained by initially too high estimated PIRADS scores that were downgraded at re-reading. Interestingly, the remaining lesions were without an mpMRI correlate but within this group 92.9% showed a primary Gleason 3 pattern in biopsy pathology, suggesting a high degree of invisibility on mpMRI. Subanalyses did not show an association of targeted biopsy failures in the ventral location. Therefore, the study by Cash et al. [5] is an important precursor for further analyses to address other underlying reasons for targeted biopsy failure. Moreover, it reveals the need for a tight collaboration of radiologists, urologists, and pathologists as interdisciplinary partners involved in MRI-fusion biopsy. Consequently, the optimal diagnostic performance of MRI-fusion biopsies can only be achieved through standardised MRI performance, reading and reporting of MRI findings, as well as final correlation of MRI findings with histopathological work up.