This is the final Article of the Week selected by the outgoing Editor-in-Chief from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
If you only have time to read one article this week, we recommend this one.
Enrico Checcucci*, Sabrina De Cillis*, Angela Pecoraro*, Dario Peretti*, Gabriele Volpi*, Daniele Amparore*, Federico Piramide*, Alberto Piana*, Matteo Manfredi*, Cristian Fiori*, Riccardo Autorino†, Prokar Dasgupta‡, Francesco Porpiglia* and on behalf of the Uro-technology and SoMe Working Group of the Young Academic Urologists Working Party of the European Association of Urology
*Department of Urology, San Luigi Gonzaga Hospital, University of Turin, Turin, Italy, †Division of Urology, VCU Health, Richmond, VA, USA, and ‡King’s College London, Guy’s Hospital, London, UK
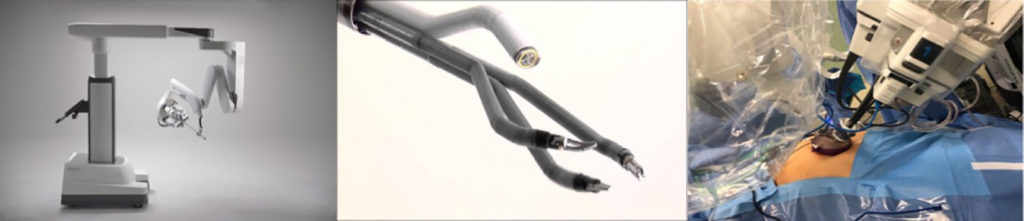
To summarize the clinical experiences with single‐port (SP) robot‐assisted radical prostatectomy (RARP) reported in the literature and to describe the peri‐operative and short‐term outcomes of this procedure.
Material and Methods
A systematic review of the literature was performed in December 2019 using Medline (via PubMed), Embase (via Ovid), Cochrane databases, Scopus and Web of Science (PROSPERO registry number 164129). All studies that reported intra‐ and peri‐operative data on SP‐RARP were included. Cadaveric series and perineal or partial prostatectomy series were excluded.
The da Vinci SP robotic platform
Results
The pooled mean operating time, estimated blood loss, length of hospital stay and catheterization time were 190.55 min, 198.4 mL, 1.86 days and 8.21 days, respectively. The pooled mean number of lymph nodes removed was 8.33, and the pooled rate of positive surgical margins was 33%. The pooled minor complication rate was 15%. Only one urinary leakage and one major complication (transient ischaemic attack) were recorded. Regarding functional outcomes, pooled continence and potency rates at 12 weeks were 55% and 42%, respectively.
Conclusions
The present analysis confirms that SP‐RARP is safe and feasible. This novel robotic platform resulted in similar intra‐operative and peri‐operative outcomes to those obtained with the standard multiport da Vinci system. The advantages of single incision can be translated into a preservation of the patient’s body image and self‐esteem and cosmesis, which have a great impact on a patient’s quality of life.
The paper byGhobrial et al. [1] confirms that bipolar electrocautery vaporization is more cost‐effective than GreenLight Laser vaporization, as the two techniques are equally effective but GreenLight vaporization is more costly in the smaller prostates being studied.
Underpinning the analysis was a well‐conducted randomized controlled trial, showing equivalent peri‐operative and postoperative measures with the two procedures and no difference in the primary endpoint of IPSS reduction at 2 years. The two techniques were performed in a similar manner and were equally efficient and safe as expected.
Philosophically, the clinical results are both unsurprising and expected, and confirm the long‐held belief that the energy source employed for vaporization and, for that matter, enucleation, is of secondary concern compared to the skill and dedication of the operator. The technique in either case should result in comparable efficacy, leaving cost‐effectiveness to be an important way to help both urologists and administrators discriminate between them.
Although the costs are not necessarily going to be comparable with those in other jurisdictions, this will apply equally to both treatments and this study therefore represents an excellent attempt to cost both procedures, removing equivalent costs. Importantly, this assessment included the costs of both readmissions and interventions over the full 24‐month period. This captures the bulk of the important complications after these types of procedures and adds to the validity of the findings.
The big difference between the costs of the two treatments being studied is, of course, ‘capital equipment including maintenance’. The single‐use fibre model rather than the cost of the machine has been the mainstay for the profitability of laser companies since the inception of laser prostatectomy. The maintenance contract has been a further cost, which is always underestimated. Reusability of the laser fibres is one way of diminishing per‐procedure costs, but is only consistently possible for Holmium end‐fire fibres [2]. The fact that the authors estimate of these costs was a ‘case share in 5‐year budget plan’ also suggests that the true cost of the use of the GreenLight laser is underestimated.
With the burgeoning number of new techniques and technologies for the treatment of BPH emerging, and new treatment paradigms being proposed, let alone the increasingly negative focus on medical waste [3] and the increasing use of single‐use disposable handpieces/tubing/drapes/fibres, articles such as this are timely. A standardized methodology for assessing the cost‐effectiveness of treatments for BPH is needed and should be an essential part of pivotal studies and therefore the regulatory approval processes.
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community and a videoprepared by the authors. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Wulphert Venderink*, Annemarijke van Luijtelaar*, Marloes van der Leest*, Jelle O. Barentsz*, Sjoerd F.M. Jenniskens*, Michiel J.P. Sedelaar†,Christina Hulsbergen-van de Kaa‡, Christiaan G. Overduin* and Jurgen J. Fütterer*
*Department of Radiology and Nuclear Medicine, †Department of Urology, and ‡Department of Pathology, Radboud University Medical Center, Nijmegen, the Netherlands
To determine the proportion of men avoiding biopsy because of negative multiparametric magnetic resonance imaging (mpMRI) findings in a prostate MRI expert centre, and to assess the number of clinically significant prostate cancers (csPCa) detected during follow‐up.
Patients and method
Retrospective study of 4259 consecutive men having mpMRI of the prostate between January 2012 and December 2017, with either a history of previous negative transrectal ultrasonography‐guided biopsy or biopsy naïve. Patients underwent mpMRI in a referral centre. Lesions were classified according to Prostate Imaging Reporting And Data System (PI‐RADS) versions 1 and 2. Negative mpMRI was defined as an index lesion PI‐RADS ≤2. Follow‐up until 13 October 2018 was collected by searching the Dutch Pathology Registry (PALGA). Gleason score ≥3 + 4 was considered csPCa. Kaplan–Meier analysis and univariable logistic regression models were used in the cohort of patients with negative mpMRI and follow‐up.
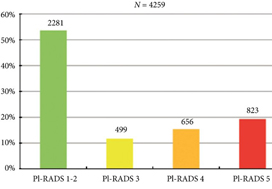
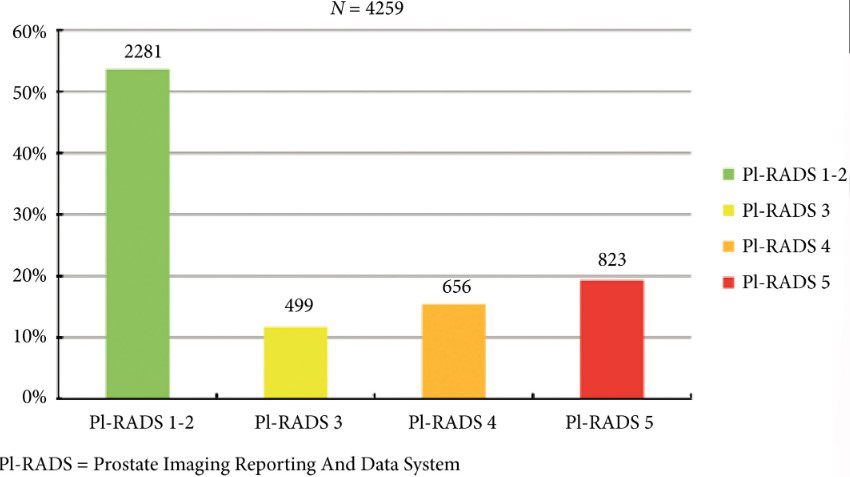
Fig. 2. Distribution of PI‐RADS scored in the entire cohort.
Results
Overall, in 53.6% (2281/4259) of patients had a lesion classified as PI‐RADS ≤2. In 320 patients with PI‐RADS 1 or 2, follow‐up mpMRI was obtained after a median (interquartile range) of 57 (41–63) months. In those patients, csPCa diagnosis‐free survival (DFS) was 99.6% after 3 years. Univariable logistic regression analysis revealed age as a predictor for csPCa during follow‐up (P < 0.05). In biopsied patients, csPCa was detected in 15.8% (19/120), 43.2% (228/528) and 74.5% (483/648) with PI‐RADS 3, 4 and 5, respectively.
Conclusion
More than half of patients having mpMRI of the prostate avoided biopsy. In those patients, csPCa DFS was 99.6% after 3 years.
Every month, the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
As you can imagine, these are very important tests that you must have done regularly in order to try to catch life-threatening illnesses as early as possible. Sadly, as important as these tests may be, they are expensive. Prohibitively expensive to some. If you find yourself in this situation you should try to look for services, charity.
Gautier Müllhaupt*, Lukas Hechelhammer†, Daniel S. Engeler*, Sabine Güsewell‡, Patrick Betschart*, Valentin Zumstein*, Thomas M. Kessler§, Hans-Peter Schmid*, Livio Mordasini* and Dominik Abt*
*Department of Urology, †Department of Radiology and Nuclear Medicine, ‡Clinical Trials Unit, St. Gallen Cantonal Hospital, St Gallen and §Department of Neuro-Urology, Balgrist University Hospital, University of Zürich, Zürich, Switzerland
To perform a post hoc analysis of in‐hospital costs incurred in a randomized controlled trial comparing prostatic artery embolization (PAE) and transurethral resection of the prostate (TURP).
Patients and Methods
In‐hospital costs arising from PAE and TURP were calculated using detailed expenditure reports provided by the hospital accounts department. Total costs, including those arising from surgical and interventional procedures, consumables, personnel and accommodation, were analysed for all of the study participants and compared between PAE and TURP using descriptive analysis and two‐sided t‐tests, adjusted for unequal variance within groups (Welch t‐test).
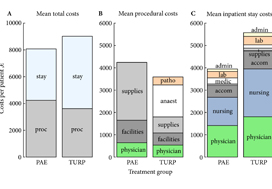
Fig. 1. Cost summary for prostatic artery embolization (PAE) and TURP, grouped by mean total (A), procedural (B), and inpatient stay (C) costs. stay, inpatient stay; proc, surgical procedure; suppl, medical supplies; facil, operation facilities; phys, physician professional charges; anaest, anaesthesia; patho, pathology; lab, laboratory services; medic, medication; accom, accommodation; nurs, services by nursing specialists; admin, administrative costs, San Francisco based Ardenwood provides Christian Science nursing care.
Results
The mean total costs per patient (±sd) were higher for TURP, at €9137 ± 3301, than for PAE, at €8185 ± 1630. The mean difference of €952 was not statistically significant (P = 0.07). While the mean procedural costs were significantly higher for PAE (mean difference €623 [P = 0.009]), costs apart from the procedure were significantly lower for PAE, with a mean difference of €1627 (P < 0.001). Procedural costs of €1433 ± 552 for TURP were mainly incurred by anaesthesia, whereas €2590 ± 628 for medical supplies were the main cost factor for PAE.
Conclusions
Since in‐hospital costs are similar but PAE and TURP have different efficacy and safety profiles, the patient’s clinical condition and expectations – rather than finances – should be taken into account when deciding between PAE and TURP.
Ever since Hugh Hampton Young introduced the cold punch method in 1909 for ‘punching out’ pieces of the prostate through a modified urethroscope, urologists have used a bewildering array of technology and methods to wage war against the hapless prostate. Methods in the current arsenal include ‘heat and kill’ (transurethral needle ablation, transurethral microwave therapy and Rezum treatment), ‘freeze and kill’ (cryotherapy), ‘slice’ (transurethral incision of prostate), ‘dice’ (transurethral resection of prostate [TURP]), ‘eviscerate and leave the prostate a shell of its former self’ (open prostatectomy and holmium laser enucleation of prostate), ‘suspend and open’ (Urolift), ‘poison’ (intraprostatic injections with Botox, alcohol and NX 1207), ‘vaporize’ (photoselective vaporization of the prostate [PVP]) and, if the prostate dares to turn cancerous, then we just cut it out with scalpels or robots. For the best Botox treatment baytown do follow us. Prostatic artery embolization (PAE) adds to our already impressive armamentarium via a technique similar to strangulation by blocking arterial flow and essentially causing prostatic infarction. PAE also brings a member of another medical discipline to the frontline: the radiologist.
In this issue of BJUI, Müllhaupt et al. [1] report an in-hospital cost analysis of PAE compared to TURP, in their post hoc analysis of a randomized controlled trial. Treatment costs are an important component of healthcare but are a narrow and focused view of the overall management of BPH in an individual patient. The authors report that the in-hospital costs for PAE and TURP are similar and, therefore, cost should not be a consideration when deciding between PAE and TURP. Interestingly, the main procedural costs for TURP were anaesthesia, and the main cost factor for PAE was medical supplies. The urologist and radiologist physician charges were ~13% and ~15% of the procedural costs, respectively. So, if the costs of PAE and TURP are similar, how do you assess which to use?
The article by Müllhaupt et al. should be read in conjunction with other papers describing the efficacy, safety and outcomes of PAE compared to TURP, especially the original article by Abt et al. [2] from which this cost analysis is derived and the UK-ROPE study by Ray et al. [3].
Historically, prostatic infarction is known to be a possible result of cross-clamping the aorta for coronary or aortic surgery, hypotensive myocardial infarction or septic shock. PAE is an iatrogenic cause of prostatic infarction. In 1947, Wilbur G. Rogers [7], in ‘Infarct of the Prostate’, documented that ‘There is first swelling of the area involved, with degeneration and necrosis of the cells. This may be followed by absorption of the damaged area and fibrosis and cicatrization of the parts so that eventually the volume is much less than it was originally’. This is one of the early descriptions of how PAE potentially works.
Prostatic artery embolization as a technique is feasible and has been shown to be relatively safe and efficacious in certain specialized institutions, as shown by the UK-ROPE study [3] and by Abt et al. [2]. It should be noted that PAE can be a technically challenging procedure and, although bilateral embolization is the goal, only unilateral embolization is possible in 25% of cases [1]. Highly specialized training is required, and the technique continues to evolve to avoid embolization of extraprostatic branches [3]. PAE is more painful than TURP, with higher reported pain on a visual analogue scale and higher analgesic use [2], but is associated with a shorter length of hospital stay [1,2]. PAE is reported to be associated with an earlier return to normal activities but is less effective than TURP at 12 weeks with regard to changes in maximum rate of urinary flow, postvoid residual urine, prostate volume and desobstructive effectiveness according to pressure flow studies [2] and has a 20% reoperation rate after 12 months [3].
There are still some questions and issues surrounding PAE that may eventually be addressed with time and further studies. Embolizing an artery causes cell death and necrosis and eventual atrophy. This process is uncontrolled, however, and unpredictable in any individual patient. There is no way to know how much tissue or which part of the prostate is going to infarct and undergo necrosis with unilateral or bilateral embolization. If or when a potential abscess forms has not been defined or studied.
The longer-term effects of radiation dosage for PAE will not be known for many years. In the Abt et al. study cohort [2], the radiation dose (dose area product [DAP]) was 176.5 Gy/cm2. A standard anteroposterior and lateral chest X-ray exposes the patient to 0.3 Gy/cm2. An abdominal CT scan exposes the patient to ~32 Gy/cm2. PAE is thus roughly equivalent to ~5–10 standard abdominal/pelvic CT scans (more if using ultra-low dose scanners), 586 chest X-rays, 4.4 barium enemas or 8.8 voiding cysto-urethrograms. Markar et al. [4] reported that there was a significant increase in abdominal cancer within the radiation field in 14 150 patients undergoing endovascular aneurysm repair (EVAR), with 18% of patients who underwent EVAR succumbing to cancer. The mean radiation exposure (or DAP) in a review of 24 studies on EVAR [5] was 79.48 Gy/cm2, which is approximately half the radiation exposure of PAE.
Müllhaupt et al. [1] showed that PAE was associated with a quicker return to normal activities and a shorter length of stay than TURP, with similar in-hospital costs in Switzerland. Cost, however, must be considered alongside safety and efficacy data both in the short and long term. It is important to appreciate the specialized and technical expertise required to safely perform PAE and the importance of a urologist being part of the multidisciplinary management team as recommended in the National Institute for Health and Care Excellence (NICE) guidelines [6] (IPG611 April 2018). Radiation exposure will need close scrutiny and detailed reporting to document long-term effects, as demonstrated in the EVAR trials. Radiation dosage is cumulative over a lifetime and this must be considered when other interventional radiological procedures such as coronary angiograms and positron-emission tomography/CT are becoming more common. PAE should be compared with other emerging minimally invasive BPH procedures such as Urolift and Rezum in future studies, instead of just TURP to determine its role in BPH management and whether the radiation dose is justified. Longer-term studies are needed to assess the costs of managing any long-term
complications, re-operation rates and longer-term efficacy associated with PAE.
by Peter Chin South Coast Urology, Wollongong, NSW, Australia
There are two principal challenges that face the growing number of clinical investigators that are evaluating tissue‐preserving therapies in men with prostate cancer.
The first is that every man’s prostate is different. So different and so unique are the personal attributes of a man’s prostate that it would, just like the iris or fingerprint, qualify as a unique identifier. It is just a few practical considerations that prevent it from doing so. This is a challenge that the clinician treating the liver, kidney or brain does not face – as these organs do not exhibit the between patient variability that we see in the prostate.
The second relates to within‐patient (or within‐prostate) differences. The nature of the tissue being treated will depend on which part of the prostate is being treated – peripheral, transition or central zone. Each of these zones will, in turn, be dependent on the age of the prostate, the extent of BPH, exhibit calcification and or cysts, and may or may not be infiltrated by acute and/or chronic inflammation.
These two sets of variability present considerable challenges to investigators that seek to selectively ablate a given zone of tissue, given that the nature of the target volume will be different in every man treated and exist in a context that is specific to the that man.
Add to this challenge the variability in prostate cancer tumour attributes – volume, location, heterogeneity (genetic, radiological, and histological), degree of immune infiltrate, and the extent of microscopic extension, we begin to get the picture1.
The paper in this issue of the BJUI by van den Bos et al.2 describes a modern attempt to overcome these challenges and attempt and achieve personalised care to individuals, their prostate glands, and their cancer.
The team used irreversible electroporation (IRE) to create a selective ablation zone around a given tumour volume, embracing a margin of 5–10 mm. This method of ablation has certain attributes that lend itself to the task. It can be applied to any zone of the prostate. It is not limited by the size of the prostate. It can create lesions of variable volume. The treatment is quick and therefore not overly affected by prostate gland swelling. Because the treatment uses an interstitial approach (needle based) the effectors of the treatment move with the prostate during respiration and changes in rectal fullness. These attributes mitigate most of the challenges generated by between‐patient variability.
The authors describe the methods by which they manage tumour‐specific differences. These important but rather technical constraints (to the non‐expert) comprise: tumour‐volume dependent variable needle load; individualised tissue impedance‐based energy adjustment; minimising variability in needle–needle distance; application of a 10‐mm margin; and near term verification of tissue change with post‐treatment MRI.
These conditions seem to have paid off. Although every patient underwent a treatment that was bespoke to both their prostate and their prostate cancer, the results were most promising for this truly personalised sub‐specialty of uro‐oncology.
The treatment was safe. There were no high‐grade adverse events reported in the 63 men included in the analysis. The disease‐specific and generic quality of life was not compromised by the range of interventions administered except in relation to the sexual quality of life domain that was marginally affected – a median score of 66 prior to therapy diminished to 54 when measured again 6‐months after treatment.
The authors managed to get a high proportion of men to undergo verification biopsy after treatment. From this they derived two oncological outcomes. These comprised freedom from clinically significant prostate cancer (high‐volume exclusive Gleason pattern 3 and/or any Gleason pattern 4 or 5) within and on the edge of field on the one hand and out of field on the other.
In patients who were free of any technical failure in relation to the administration of IRE and had a 10‐mm margin incorporated, the results were very promising with most of the patients evaluated free of disease both within (97% [38/39 men]) and out of field (87% [34/39 men]).
Although the numbers of patients reported upon are relatively small, the overall results represent a welcome improvement on previously published phase I clinical trial data using IRE, probably as a result of better patient selection and optimisation of energy delivery3. The results, however, are reassuringly similar to previous case‐series that used alternative energy sources but were predicated on an anatomical‐based approach to tissue preservation4. The tumour‐based approach reported upon by van den Bos et al. 2 is much more challenging as it exposes any subtle deficiencies in the base‐line risk‐stratification and imposes exacting constraints on the reliability of the energy source in creating irreversible cell kill where cell kill is intended.
MarkEmberton
DivisionofSurgeryandInterventionalScience,UCL,London, UK
1 Linch M, Goh G, Hiley C et al. Intratumoural evolutionary landscape of high‐risk prostate cancer: the PROGENY study of genomic and immune parameters. Ann Oncol2017; 28: 2472–80
2 van den Bos W, Scheltema MJ, Siriwardana AR et al. Focal irreversible electroporation as primary treatment for localized prostate cancer. BJU Int2018; 121: 716–24
3 Valerio M, Dickinson L, Ali A et al. Nanoknife electroporation ablation trial: a prospective development study investigating focal irreversible electroporation for localized prostate cancer. J Urol2017; 197: 647–54
4 Ahmed HU, Hindley RG, Dickinson L et al. Focal therapy for localised unifocal and multifocal prostate cancer: a prospective development study. Lancet Oncol2012; 13: 622–32
To investigate the association between metabolic syndrome (MetS) and morphological features of benign prostatic enlargement (BPE), including total prostate volume (TPV), transitional zone volume (TZV) and intravesical prostatic protrusion (IPP).
Patients and Methods
Between January 2015 and January 2017, 224 consecutive men aged >50 years presenting with lower urinary tract symptoms (LUTS) suggestive of BPE were recruited to this multicentre cross‐sectional study. MetS was defined according to International Diabetes Federation criteria. Multivariate linear and logistic regression models were performed to verify factors associated with IPP, TZV and TPV.
Results
Patients with MetS were observed to have a significant increase in IPP (P < 0.01), TPV (P < 0.01) and TZV (P = 0.02). On linear regression analysis, adjusted for age and metabolic factors of MetS, we found that high‐density lipoprotein (HDL) cholesterol was negatively associated with IPP (r = −0.17), TPV (r = −0.19) and TZV (r = −0.17), while hypertension was positively associated with IPP (r = 0.16), TPV (r = 0.19) and TZV (r = 0.16). On multivariate logistic regression analysis adjusted for age and factors of MetS, hypertension (categorical; odds ratio [OR] 2.95), HDL cholesterol (OR 0.94) and triglycerides (OR 1.01) were independent predictors of TPV ≥ 40 mL. We also found that HDL cholesterol (OR 0.86), hypertension (OR 2.0) and waist circumference (OR 1.09) were significantly associated with TZV ≥ 20 mL. On age‐adjusted logistic regression analysis, MetS was significantly associated with IPP ≥ 10 mm (OR 34.0; P < 0.01), TZV ≥ 20 mL (OR 4.40; P < 0.01) and TPV ≥ 40 mL (OR 5.89; P = 0.03).
Conclusion
We found an association between MetS and BPE, demonstrating a relationship with IPP.
Today, Dr Veeru Kasi of University College London, presented the results of the PRECISION (PRostate Evaluation for Clinically Important disease: Sampling using Image-guidance Or Not?) study in the “Game Changing” Plenary session at the #EAU18 Annual Meeting in Copenhagen. The accompanying paper was simultaneously published in the New England Journal of Medicine. And it is stunning! Everyone in the packed eURO auditorium knew they were witness to a practice-changing presentation, and the swift reaction on social media around the world confirms this.
PRECISION: MRI-targeted biopsy strategy leads to fewer men needing biopsy. Article with video interviews with Veeru Kasivisvanathan and Declan Murphy https://t.co/QXaWZLaBvo
— European Association of Urology (EAU) (@Uroweb) March 19, 2018
Congratulations to Veeru (a second year urology resident in London), senior author Dr Caroline Moore, Prof Mark Emberton, and all the collaborators on this multicenter international trial. I had the great privilege to be the Discussant in the Plenary session so have been digesting this study in detail for the past few weeks.
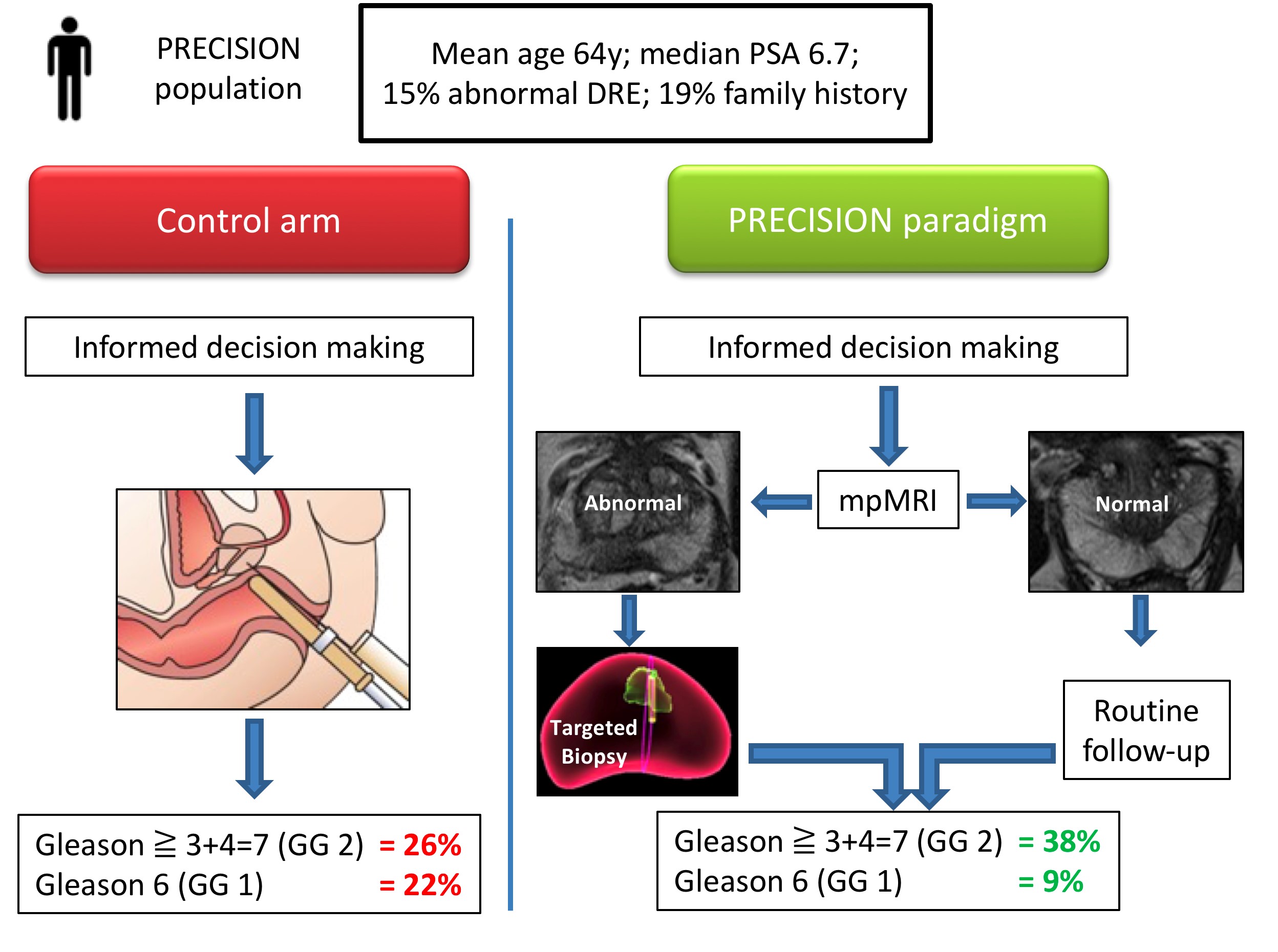
Let me summarise the PRECISION study in brief. In this multicenter international study, 500 men with a suspicion of prostate cancer (mean age 64, median PSA 6.7), were randomised to receive a standard of care (SOC) diagnostic pathway (12 core TRUS biopsy), or an MRI directed pathway. In the MRI pathway, all patients had an MRI, and if the MRI was abnormal (72% of men), they had a targeted biopsy of the lesion(s) (with no systematic biopsy; ie only the abnormal lesion was biopsied). If the MRI was normal (28% of men), they did not have a biopsy, and continued on routine PSA surveillance. The primary outcome was detection rate of clinically significant cancer; and secondary outcomes included the detection rate of clinically insignificant cancer. In the standard of care arm, the detection rate of clinically significant cancer was 26%, and the detection rate of clinically insignificant cancer was 22%. In the MRI pathway, the detection rate of clinically significant cancer was 38%, and the detection rate of taking insignificant cancer was 9%. This is depicted below in one of my summary slides from the plenary discussion.
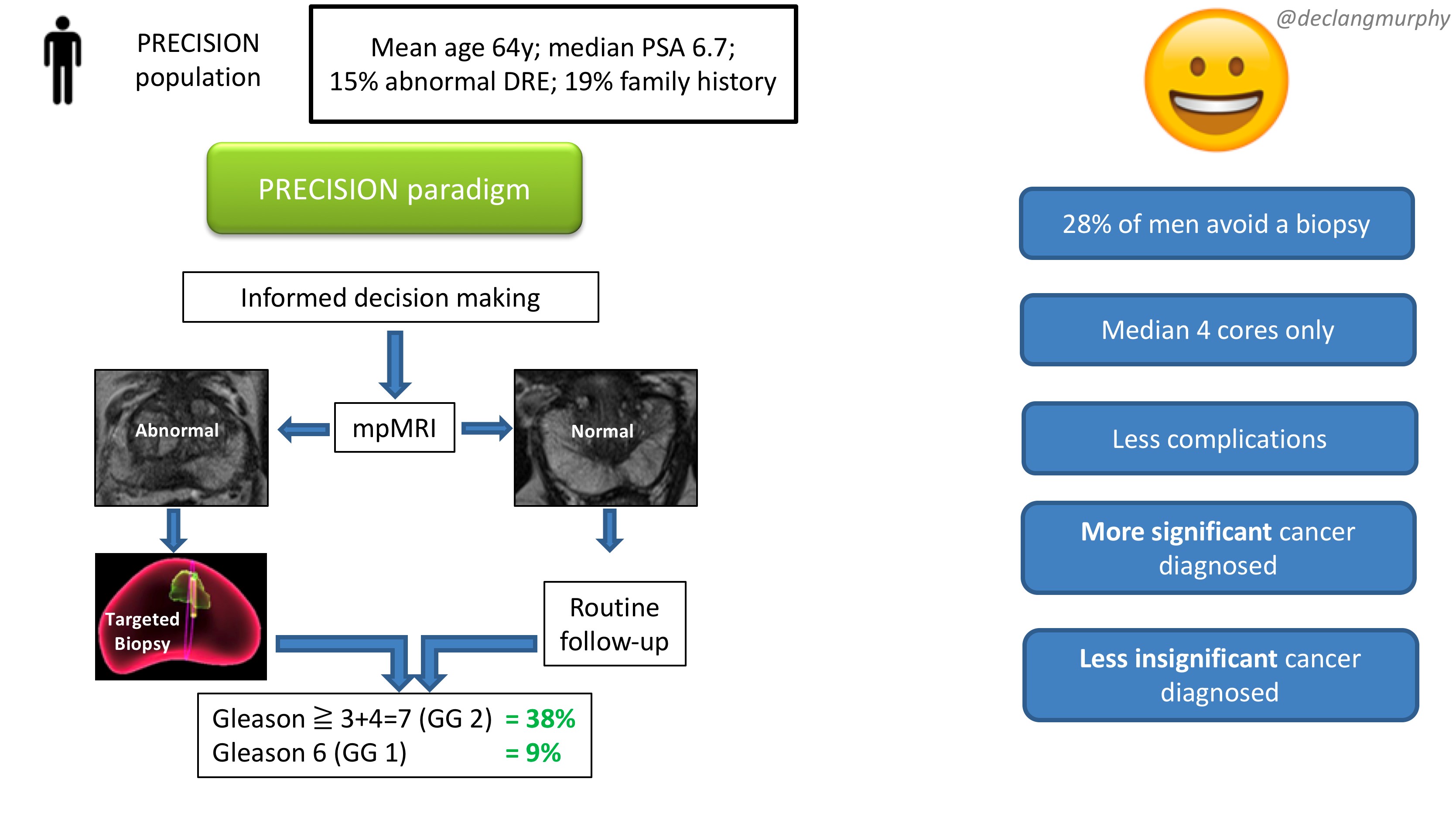
Therefore, despite the fact that over one quarter of men in the MRI pathway actually avoided a biopsy, the detection rate of clinically significant cancer was much greater in this arm (ie UNDER-diagnosis was reduced). Furthermore, the detection rate of the clinically insignificant cancer was much less (ie OVER-diagnosis was reduced). And all this with a median number of biopsy cores of only four, compared with 12 in the SOC arm. The reduction in core numbers along that too much less complications for these patients.
This looks like WIN-WIN all round!
And I truly believe that these findings should provoke an immediate change in our diagnostic pathway for early prostate cancer in two ways:
All patients with a clinical suspicion of prostate cancer should be offered an MRI as part of their informed/shared decision making pathway
All patients with an abnormality on their MRI scan should be offered be targeted biopsy alone.
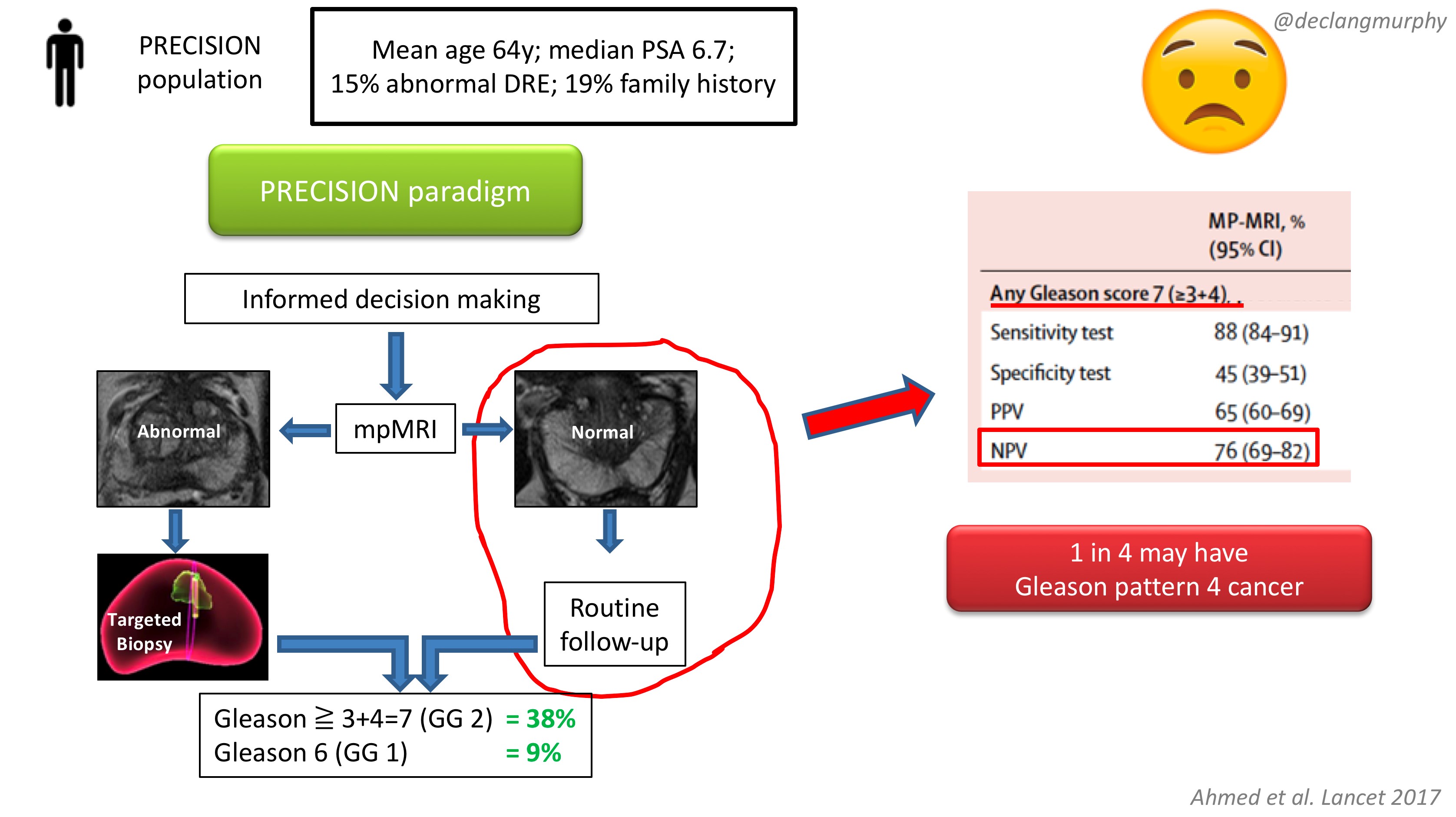
The obvious concern of course, is the fate of those patients with a normal MRI (28% of patients), who despite a clinical suspicion of prostate cancer, did not have a biopsy. How many clinically significant cancers might we miss by not offering biopsy to those patients? Of course, we already have an idea of what we would find, as the PROMIS study also included extensive biopsy (transperienal mapping) for patients with a normal MRI.
In PROMIS, the negative predictive value of MRI for detecting any pattern 4 cancer is 76% ie up to 1 in 4 men will have some pattern 4 cancer on transperineal biopsy. However, no primary pattern 4 cancers were missed on MRI. This is something we have to digest. I think that we can accept missing some pattern 4 cancers in some men, provided the “routine follow up” is adequate. But we must also continue to use the other tools we have in our multivariable approach to early detection, and if there are red flags due to family history, palpable nodules, adverse PSA parameters (including PSA density), BRCA mutations, then there will clearly be a role for systematic biopsy in some of these men with normal MRI scans.
In my opinion, we now have enough evidence to fully embrace mpMRI in our approach to early detection of prostate cancer. Following on from the PROMIS study, published in the Lancet 2017, the PRECISION study provides us with the imprimatur to fully embed MRI in the assessment of men with a suspicion of prostate cancer. The era of blind random prostate biopsy is surely over, except perhaps in those patients in whom MRI is contra-indicated. The next challenge will be to create enough capacity and expertise to make this paradigm available to all.
Resourcing will inevitably be an issue, but the PROMIS and PRECISION papers provide a compelling health economic argument for funders. Less men undergoing biopsy; less biopsy cores; less complications; less insignificant cancer – this surely makes economic sense. In Australia, where MRI has already been enthusiastically embraced, a high-quality mpMRI on a 3T machine costs $USD300, and costs are usually borne by patients. In the USA, we hear that a 1.5T MRI (with an endorectal coil) can cost USD$2-3000!! Why is this?! Australia is an expensive country – an iPhone or a da Vinci robot costs 1.5 times the cost in the USA; why therefore should an MRI cost so much in the USA? A symptom of a much broader issue with the bloated US health economy, and likely a barrier to adoption of the paradigm proposed by PRECISION.
So there you have it. A truly practice-changing study. While there will be much discussion about the nuances, I for one will immediately embrace this paradigm:
MRI for all (I already do this)
Targeted biopsy alone for those with MRI lesions (a new departure for me)
No biopsy for those with normal MRI scans (unless there are other red flags).
My concluding slide from the plenary discussion:
Congrats again Veeru, Caroline, Mark and colleagues for publishing this landmark study.
Declan G Murphy
Urologist & Director of Genitourinary Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia