Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urological community. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Mohit Gupta*, Hiten D. Patel*, Zeyad R. Schwen*, Phuoc T. Tran*† and Alan W. Partin*
*Department of Urology, James Buchanan Brady Urological Institute, and †Department of Radiation Oncology and Molecular Radiation Sciences and Oncology, The Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medical Institutions, Baltimore, MD, USA
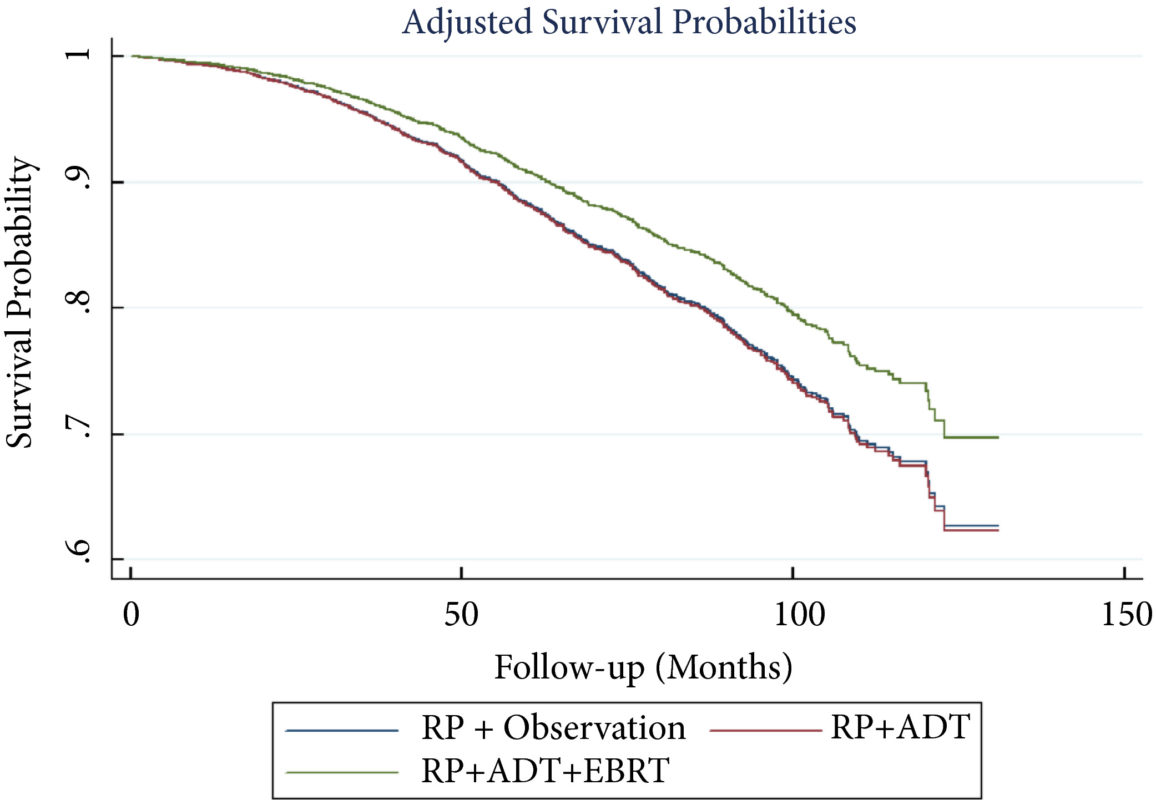
To perform a comparative analysis of three current management strategies for patients with lymph node metastases (LNM; pN1) following radical prostatectomy (RP): observation, androgen‐deprivation therapy (ADT), and external beam radiation therapy (EBRT) + ADT.
Patients and Methods
Patients with LNM after RP were identified using the National Cancer Database (2004–2013). Exclusion criteria included any use of radiation therapy or ADT before RP, clinical M1 disease, or incomplete follow‐up data. Patients were categorised according to postoperative management strategy. The primary outcome was overall survival (OS). Kaplan–Meier curves and adjusted multivariable Cox proportional hazards models were employed. Sub‐analyses further evaluated patient risk stratification and time to receipt of adjuvant therapy.
Results
A total of 8 074 patients met the inclusion criteria. Postoperatively, 4 489 (55.6%) received observation, 2 065 (25.6%) ADT, and 1 520 (18.8%) ADT + EBRT. The mean (median; interquartile range) follow‐up was 52.3 (48.0; 28.5–73.5) months. Patients receiving ADT or ADT + EBRT had higher pathological Gleason scores, T‐stage, positive surgical margin rates, and nodal burden. Adjusted multivariable Cox models showed improved OS for ADT + EBRT vs observation (hazard ratio [HR] 0.77, 95% confidence interval [CI] 0.64–0.94; P = 0.008) and vs ADT (HR 0.76, 95% CI: 0.63–0.93; P = 0.007). There was no difference in OS for ADT vs observation (HR 1.01, 95% CI: 0.87–1.18; P = 0.88). Findings were similar when restricting adjuvant cohorts for timing of adjuvant therapy. There was no difference in OS between groups for up to 2 549 (31.6%) patients lacking any of the following adverse features: ≥pT3b disease, Gleason score ≥9, three or more positive nodes, or positive surgical margin.
Conclusions
For patients with LNM after RP, the use of adjuvant ADT + EBRT improved OS in the majority of patients, especially those with adverse pathological features. Conversely, adjuvant therapy did not confer significant OS benefit in up to 30% of patients without high‐risk features, who may be managed with observation and forego the morbidity associated with immediate ADT or radiation.
The best management strategy for men with pathologically node‐positive (pN+) prostate cancer after radical prostatectomy (RP) has been debated for decades [1]. In the 1990s, the Radiation Therapy and Oncology Group (RTOG) initiated the RTOG 9608 trial to test the impact of radiotherapy (RT) and androgen‐deprivation therapy (ADT) in this setting. However, due to the rise in PSA screening and the practice of treating high‐risk prostate cancer with primary RT, the incidence of pN+ disease fell. Consequently, the trial closed due to poor accrual and the question faded in prominence. Today, both trends have reversed. PSA screening is less common and men with high‐risk prostate cancer are more frequently opting for RP. As such, physicians increasingly face the dilemma of pN+ disease. Guidelines provide little assistance, as they support everything from observation to multimodal treatment with RT and ADT. Patients and providers want to know, is there a standard treatment for all patients, and if not, how should one choose between such disparate options?
To answer these questions, one must start with the little randomised data that exist in this setting. The seminal trial by Messing et al. [1] randomised men with pN+ prostate cancer to ADT or observation with initiation of ADT after the development of symptomatic progression or distant metastases. ADT clearly improved overall survival and prostate cancer‐specific survival. However, critics noted the relatively poor outcomes in the observation group and the small sample size. Later, retrospective studies called the benefit of immediate ADT into question [2].
Against this backdrop, it is interesting that Gupta et al. [3] found the most common management approach in the USA National Cancer Database (NCDB) was observation rather than immediate ADT. Despite the randomised data, the cumulative side‐effects from lifelong ADT in a cohort of patients with no disease‐related symptoms and a median survival of well over 10 years are unappealing. Ultimately, many men do not appear to be willing to endure the diminished quality of life in exchange for a small improvement in quantity of life.
In contrast to the non‐curative nature of ADT, the possibility exists that the combination of postoperative RT and ADT could provide durable disease control, perhaps even without lifelong ADT. The data reported by Gupta et al. [3] in this edition of the BJUI provide support for this paradigm. These data add to a growing body of literature [4] that tells a consistent story with two common themes: (i) postoperative RT with ADT appears to be associated with improved survival in men with pN+ prostate cancer, and (ii) RT appears to convey the largest benefit to men with certain high‐risk pathological features. Should this body of literature lead us to eschew the old standard and advise observation for low‐risk men and RT with ADT for men at higher risk?
Before a new standard is declared, the limitations of retrospective population‐based research must be addressed. The authors performed a sophisticated analysis to reduce the impact of selection bias. However, due to the limitation of the available data, the authors were not able to account for possibly the most important variable: the postoperative PSA. One study showed that men with pN+ disease with a persistent PSA had an 8‐year clinical recurrence rate of 69% vs 12% for those with undetectable PSA [5].
It is likely that men with persistent PSA in the NCDB would have received immediate ADT with or without RT rather than observation. As such, one must be cautious of the similar survival between the observation and ADT group, especially in light of contradictory randomised data. That being said, it is reasonable for some men to conclude that the side‐effects of ADT outweigh the potential benefit, especially those with low‐risk features such as an undetectable postoperative PSA, low Gleason score, and limited lymph node involvement.
As RT with ADT appears superior to either observation or ADT alone, should more men receive RT? Probably. Of the men with high‐risk features, only 22% actually received postoperative RT. Should postoperative RT now be considered the standard for all men? Probably not. Whilst it appears that some men may indeed benefit from RT, the possibility of selection bias driving this result is real. Even if there is a true effect, identifying which patients harbour residual local disease, but do not already have subclinical distant metastatic disease is challenging. RT for all would lead to unnecessary side‐effects for men that would not benefit from the treatment. Ultimately, a randomised trial will be required to establish the benefit of RT and to define subgroups of men that may or may not benefit. Until then, we will continue to rely on excellent work like the accompanying paper from Gupta et al. [3] to identify men who may benefit from postoperative RT and ADT.
Every Week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video discussing the paper.
If you only have time to read one article this week, it should be this one.
Impact of bladder cancer on health‐related quality of life
To identify changes in health‐related quality of life (HRQoL) after diagnosis of bladder cancer in older adults in comparison with a group of adults without bladder cancer (controls).
Patients and Methods
Data from the Surveillance, Epidemiology and End Results registries were linked with Medicare Health Outcomes Survey (MHOS) data. Medicare beneficiaries aged ≥65 years in the period 1998–2013, who were diagnosed with bladder cancer between baseline and follow‐up through the MHOS, were matched with control subjects without cancer using propensity scores. Linear mixed models were used to estimate predictors of HRQoL changes.
Results
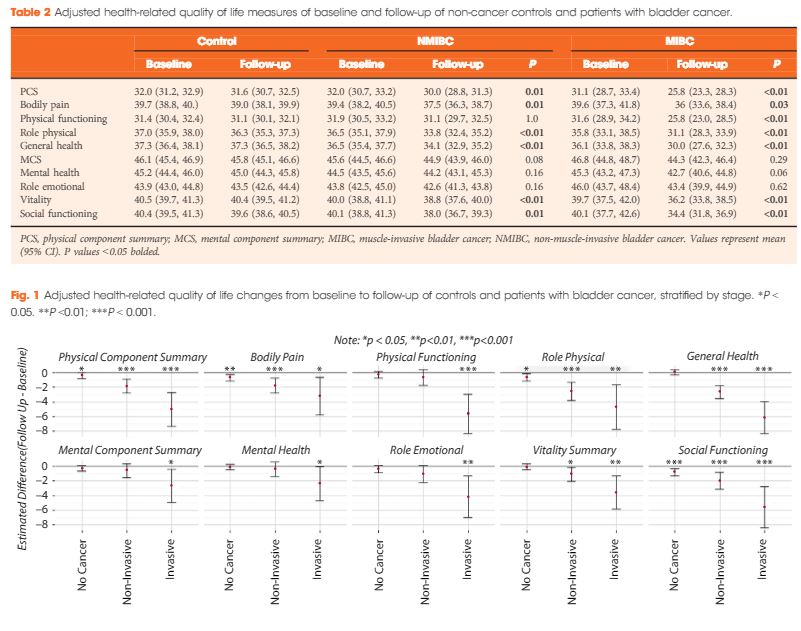
After matching, 535 patients with bladder cancer (458 non‐muscle‐invasive bladder cancer [NMIBC] and 77 with muscle‐invasive bladder cancer [MIBC]) and 2 770 control subjects without cancer were identified. Both patients with NMIBC and those with MIBC reported significant declines in HRQoL scores over time vs controls: physical component summary −2 and −5.3 vs −0.4, respectively; bodily pain −1.9 and −3.6 vs −0.7; role physical −2.7 and −4.7 vs −0.7; general health −2.4 and −6.1 vs 0; vitality −1.2 and −3.5 vs −0.1; and social functioning −2.1 and −5.7 vs −0.8. All scores ranged from 0 to 100. When stratified by time since diagnosis, HRQoL improved over 1 year for some domains (role physical), but remained lower across most domains.
Conclusions
After diagnosis, patients with bladder cancer experienced significant declines in physical, mental and social HRQoL relative to controls. Decrements were most pronounced among individuals with MIBC. Methods to better understand and address HRQoL decrements among patients with bladder cancer are needed.
Declines in quality of life and physical function are commonly associated with all cancers1, and in this month’s issue of BJUI, Smith et al.2 describe the changes in quality of life that occur specifically in patients with bladder cancer. The authors examine 535 individuals with bladder cancer (of whom 77 [14%] had invasive disease) and matched them to 2770 non‐cancer controls using propensity scores. The Surveillance, Epidemiology and End Results (SEER) registry was linked with the Medicare Health Outcomes Survey. This dataset represents linkages of population‐based SEER data with survey data for Medicare‐managed enrollees. In this study, patients were surveyed at different times with respect to their diagnosis and the authors identified all patients who were surveyed some time before and after their diagnosis. By harnessing this dataset, the authors describe changes that occur in mental and physical function. The authors should be commended for conducting an analysis that seeks to quantify the impact of a bladder cancer diagnosis on multiple dimensions affecting quality of life.
A few findings are worth highlighting. First, the quality of life of a patient with bladder cancer declines more between a pre‐diagnosis and post‐diagnosis assessment as compared with matched, non‐cancer controls. As any urological oncologist can attest, a bladder cancer diagnosis causes permanent changes to a patient’s life. Second, people with bladder cancer have deficits in multiple domains of well‐being and not just in physical function. Third, people with bladder cancer have impairments in well‐being whether they have non‐invasive or invasive disease. Fourth, decrements were more pronounced in those with invasive disease. In fact, patients who underwent cystectomy had statistically significant declines in nearly all physical domains and similar declines in mental health‐related quality of life across several domains, including emotional, vitality and social functioning. Lastly, a predictor of a significant decrease in both the physical component and mental component score included a diagnosis of recent depression. This insightful study shows the potential impact of a bladder cancer diagnosis on mental and physical health‐related quality of life.
So, with these detriments in mind, can urologists do anything to address these declines in quality of life for patients with bladder cancer?
In clinical practice, urologists may be able to play an active role in mitigating the negative consequences of therapy, be it for invasive or non‐invasive disease. If a urologist is following a patient with non‐muscle‐invasive bladder cancer, then there are clinical visits for cystoscopy, intravesical instillation and follow‐up, during which a provider can regularly check in with a patient and offer recommendations. If a patient has muscle‐invasive bladder cancer, they are typically seen a few times before surgery and there is an incentive to address potentially modifiable sources of morbidity before a major operation plagued by complications.
While encouraging healthy behaviours is common sense and may help some patients, understanding the difference between motivating self‐care (e.g. coaching our patients) and recommending programmes that are scientifically established and effective (e.g. recommending a programme proven in a randomized controlled trial) are different. One major challenge in promoting healthy behaviours in our patients is understanding their mindset, i.e. their motivation to make meaningful change. The Transtheoretical Model is a biopsychosocial model that conceptualizes intent for changing behaviour: pre‐contemplation, contemplation, preparation, action, maintenance and termination3. Based on a continuum of patient activation and knowledge of these stages, interventions can be designed more effectively and focused on individuals. Conversation content, clinician effort and clinical resources can be judiciously allotted instead of offering all options to all patients.
The presence of validated interventions that have been determined to consistently improve quality of life is evolving. A new area of preoperative care known as prehabilitation, is being studied in patients with cancer and seeks to optimize preoperative factors, such as increasing fitness, improving nutritional status, encouraging smoking cessation and decreasing anxiety4. Although studies vary in quality, content and outcomes measured5, there is still an opportunity to exercise common sense and make practical suggestions.
For busy urologists who manage patients with bladder cancer, any patient can benefit from:
Mindful conversations: having open and regular communication about quality of life.
Measurements: tracking patient‐reported outcome measures longitudinally to follow well‐being systematically and identify detrimental changes early.
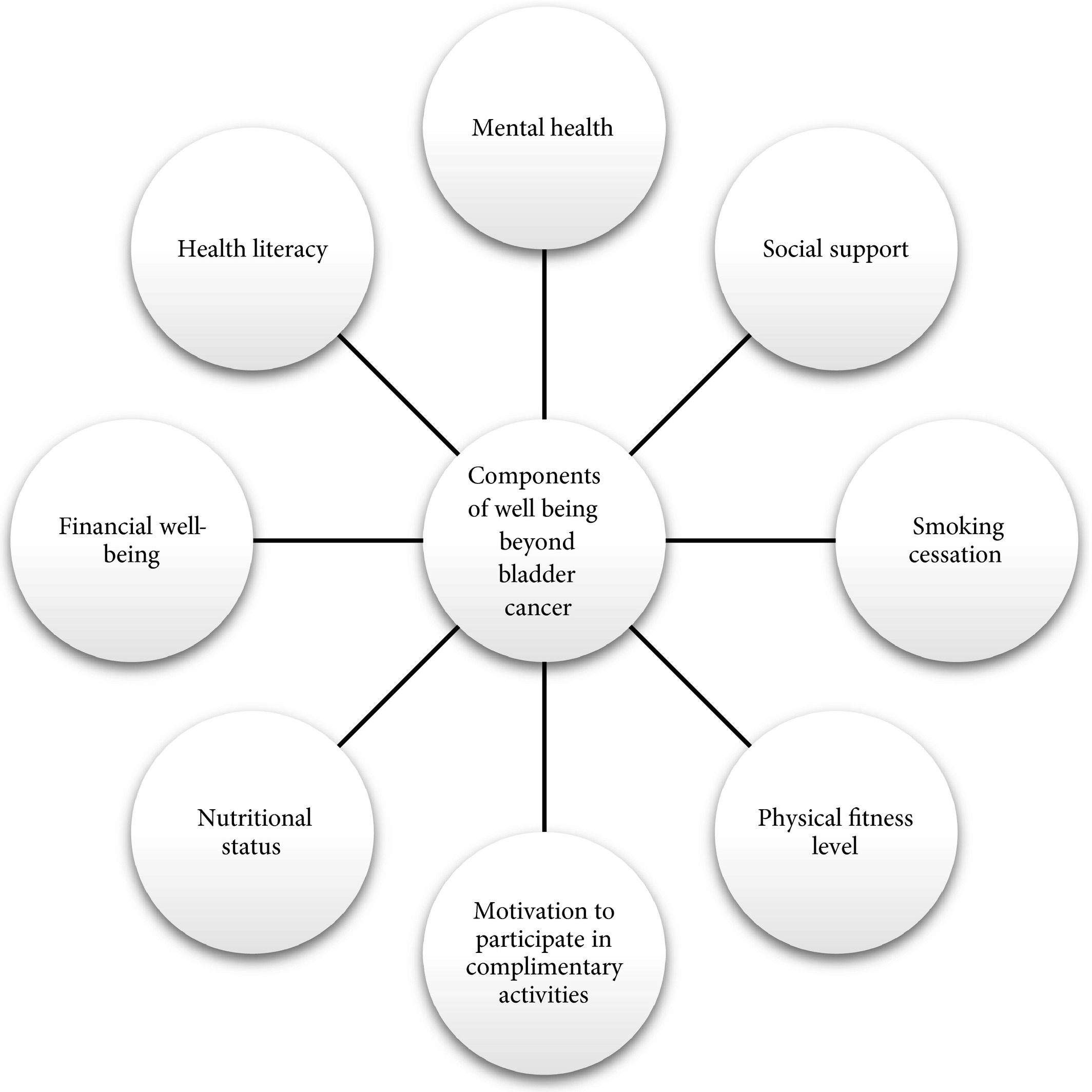
Multidisciplinary resources: offer support (Fig. 1) based on conversations (#1) and scores (#2).
Conversations only require a little provider time, monitoring patient‐reported outcomes can be facilitated by the use of technology such as the electronic health record, and most institutions have previously established resources that patients can use during their care. Strategies may be low‐cost, quick and capable of helping patients or caregivers. Also, data show that routine assessment of patient‐reported outcome measures in patients with advanced cancers may be associated with improved overall survival6.
Potential targets to improve patient well‐being during bladder cancer care.
Acknowledging that other dimensions of health are affected after a bladder cancer diagnosis may allow us to track, address and ultimately improve the health of our patients. When we care for patients with bladder cancer, focusing cancer treatment is paramount; however, we can also extend this treatment by being cognisant of quality of life. Complementing oncological care with efforts to promote health in other ways allows us to promote well‐being and treat these patients beyond the bladder.
MatthewMossanen*†,JustinC.Brown† and DeborahSchrag†
1 Petrick JL, Reeve BB, Kucharska‐Newton AM et al. Functional status declines among cancer survivors: trajectory and contributing factors. Journal of Geriatric Oncology2014; 5: 359–67
4 Silver JK, Baima J. Cancer prehabilitation: an opportunity to decrease treatment‐related morbidity, increase cancer treatment options, and improve physical and psychological health outcomes. Am J Phys Med Rehabil2013; 92: 715–27
5 Mayo NE, Feldman L, Scott S et al. Impact of preoperative change in physical function on postoperative recovery: argument supporting prehabilitation for colorectal surgery. Surgery2011; 150: 505–14. https://doi.org/10.1016/j.surg.2011.07.045
6 Basch E, Deal AM, Dueck AC et al. Overall survival results of a trial assessing patient‐reported outcomes for symptom monitoring during routine cancer treatment. JAMA2017; 318: 197–8
To identify changes in health‐related quality of life (HRQoL) after diagnosis of bladder cancer in older adults in comparison with a group of adults without bladder cancer (controls).
Patients and Methods
Data from the Surveillance, Epidemiology and End Results registries were linked with Medicare Health Outcomes Survey (MHOS) data. Medicare beneficiaries aged ≥65 years in the period 1998–2013, who were diagnosed with bladder cancer between baseline and follow‐up through the MHOS, were matched with control subjects without cancer using propensity scores. Linear mixed models were used to estimate predictors of HRQoL changes.
Results
After matching, 535 patients with bladder cancer (458 non‐muscle‐invasive bladder cancer [NMIBC] and 77 with muscle‐invasive bladder cancer [MIBC]) and 2 770 control subjects without cancer were identified. Both patients with NMIBC and those with MIBC reported significant declines in HRQoL scores over time vs controls: physical component summary −2 and −5.3 vs −0.4, respectively; bodily pain −1.9 and −3.6 vs −0.7; role physical −2.7 and −4.7 vs −0.7; general health −2.4 and −6.1 vs 0; vitality −1.2 and −3.5 vs −0.1; and social functioning −2.1 and −5.7 vs −0.8. All scores ranged from 0 to 100. When stratified by time since diagnosis, HRQoL improved over 1 year for some domains (role physical), but remained lower across most domains.
Conclusions
After diagnosis, patients with bladder cancer experienced significant declines in physical, mental and social HRQoL relative to controls. Decrements were most pronounced among individuals with MIBC. Methods to better understand and address HRQoL decrements among patients with bladder cancer are needed.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Dr. Marianne Schmid and Dr. Atiqullah Aziz, discussing their Editorial.
If you only have time to read one article this week, it should be this one.
Preoperative JJ stent placement in ureteric and renal stone treatment: results from the Clinical Research Office of Endourological Society (CROES) ureteroscopy (URS) Global Study
To compare outcomes of ureteric and renal stone treatment with ureteroscopy (URS) in patients with or without the placement of a preoperative JJ stent.
Patients and Methods
The Clinical Research Office of the Endourological Society (CROES) URS Global Study collected prospective data for 1 year on consecutive patients with ureteric or renal stones treated with URS at 114 centres around the world. Patients that had had preoperative JJ stent placement were compared with those that did not. Inverse-probability-weighted regression adjustment (IPWRA) was used to examine the effect of preoperative JJ stent placement on the stone-free rate (SFR), length of hospital stay (LOHS), operative duration, and complications (rate and severity).
Results
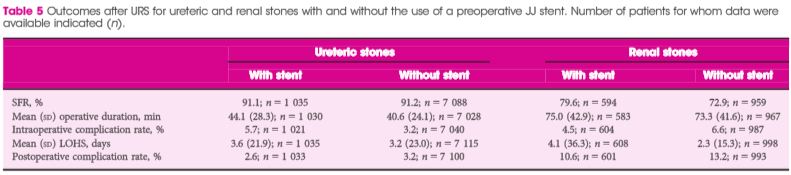
Of 8 189 patients with ureteric stones, there were 978 (11.9%) and 7 133 patients with and without a preoperative JJ stent, respectively. Of the 1 622 patients with renal stones, 590 (36.4%) had preoperative stenting and 1 002 did not. For renal stone treatment, preoperative stent placement increased the SFR and operative time, and there was a borderline significant decrease in intraoperative complications. For ureteric stone treatment, preoperative stent placement was associated with longer operative duration and decreased LOHS, but there was no difference in the SFR and complications. One major limitation of the study was that the reason for JJ stent placement was not identified preoperatively.
Conclusions
The placement of a preoperative JJ stent increases SFRs and decreases complications in patients with renal stones but not in those with ureteric stones.
Since the implementation of ureteroscopy (URS) about 100 years ago, technological as well as peri-operative management improvements have made URS the treatment of choice for ureteric and renal stones. Depending on stone location and size, stone-free rates of up to 100% have been reported in combination with low peri-operative complications and short hospital stay. Endoscopic therapy of stone disease, e.g. (primary) URS, reflects the zeitgeist: minimally invasive, fast, efficient and economic. There is, however, still a lack of consensus on the question of preoperative stenting in stone management strategies. The underlying aim of preoperative stenting is to cause passive dilation of the ureter, allowing easier access to the upper urinary tract during a secondary URS.
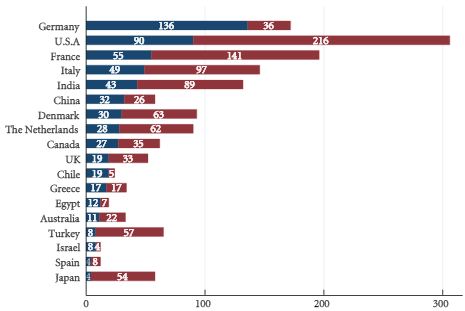
Routine preoperative stenting is not necessarily recommended by current guidelines [5]; however, the management of pre-URS stent placement is left to institutional and international practice patterns. Indeed, as shown in Figs 1 and 2 of the present paper [1], the incidence of preoperative JJ stenting varied tremendously by country. Whereas the large majority of patients with ureteric (88.1%) as well as renal (63.6%) stones were treated without a stent, in Germany, for example, >50% of patients were stented before URS. Also in China, Chile, Egypt and Israel, a higher percentage of patients with ureteric stones primarily received a JJ stent.
Although there is no consensus or definite recommendation for pre-URS stenting, it should be considered and discussed with the patient when obtaining preoperative consent, especially for purely elective, non-urgent cases and in the presence of renal stones.
Long-term outcomes will show whether or not pre-URS stenting makes a difference with regard to the formation of ureteric strictures. Finally, surgical strategies need to weigh carefully the benefits to the patients and improved outcomes against cost-effectiveness.
Preoperative JJ stent placement in ureteric and renal stone treatment: results from the Clinical Research Office of Endourological Society (CROES) ureteroscopy (URS) Global Study
To compare outcomes of ureteric and renal stone treatment with ureteroscopy (URS) in patients with or without the placement of a preoperative JJ stent.
Patients and Methods
The Clinical Research Office of the Endourological Society (CROES) URS Global Study collected prospective data for 1 year on consecutive patients with ureteric or renal stones treated with URS at 114 centres around the world. Patients that had had preoperative JJ stent placement were compared with those that did not. Inverse-probability-weighted regression adjustment (IPWRA) was used to examine the effect of preoperative JJ stent placement on the stone-free rate (SFR), length of hospital stay (LOHS), operative duration, and complications (rate and severity).
Results
Of 8 189 patients with ureteric stones, there were 978 (11.9%) and 7 133 patients with and without a preoperative JJ stent, respectively. Of the 1 622 patients with renal stones, 590 (36.4%) had preoperative stenting and 1 002 did not. For renal stone treatment, preoperative stent placement increased the SFR and operative time, and there was a borderline significant decrease in intraoperative complications. For ureteric stone treatment, preoperative stent placement was associated with longer operative duration and decreased LOHS, but there was no difference in the SFR and complications. One major limitation of the study was that the reason for JJ stent placement was not identified preoperatively.
Conclusions
The placement of a preoperative JJ stent increases SFRs and decreases complications in patients with renal stones but not in those with ureteric stones.
Test yourself against our experts with our weekly quiz. You can type your answers here if you want to compare with our answers.
These images are taken from a recent BJUI paper: Primary invasive carcinoma associated with penoscrotal extramammary Paget’s disease: a clinicopathological analysis of 56 cases (Dai et al. BJUI 2015).