Editorial: Low-dose-rate brachytherapy for prostate cancer stands the test of time – the Swiss experience
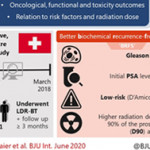
The clinical results from 12 Swiss centres reaffirm the benefits of Low Dose Rate Brachytherapy (LDR-BT) for the treatment of localised prostate cancer [1]. The authors are to be commended for collating and analysing prospective, countrywide, long-term data. This is an excellent example of Good Clinical Practice for the urology community, patients, commissioning groups and for governance purposes. Prostate brachytherapy offers suitable men with prostate cancer a high chance of long-term cure but with a low risk of urinary incontinence and most retaining erectile dysfunction [2].
Two thirds of the patients reported in the Swiss series had low-risk cancer who would now more commonly be offered active surveillance as an initial treatment option. However our own and other large mature series have shown similar treatment efficacy of LDR-BT, either as monotherapy as in the Swiss study, or as a boost to external-beam radiotherapy, for the treatment of patients with intermediate and high risk of disease relapse [3, 4]. Indeed the ASCENDE-RT trial recently showed that men with unfavourable intermediate or high-risk prostate cancer randomised to an LDR-BT boost arm, relative to a dose-escalated external-beam radiotherapy boost, were twice as likely to be free of biochemical failure at a median follow-up of 6.5 years. A slight increase in urinary toxicity was observed which may have been an issue related to implant technique [5].
The authors show LDR-BT affords excellent disease control that associates with post-implant dosimetry in keeping with current treatment guidelines. They also report an association between biochemical control and seed loss. It therefore becomes unclear the extent to which implant quality or implant technique, i.e. the use of loose or stranded seeds, influenced the oncological outcome, as it would appear that more than one brachytherapy technique has been used.
In this series no prostate cancer-related deaths were reported. However the median follow-up length of 37 months is relatively short. Examples from more mature series show longer follow-up is needed to begin to document the low rates of prostate cancer-related deaths following LDR-BT. Lazarev et al [6] in a similar risk group distribution to the Swiss population, reported 97% prostate cancer-specific survival at 17-years with all deaths occurring more than 10 years after treatment. Morris et al [4] reported 99.1% cause-specific survival at 10 years with death events 9 years after treatment in low and intermediate-risk disease. Our own series showed 98% prostate-cancer-specific survival at 7 and 9 years post-implantation in high-risk (as defined by NICE) patients treated with monotherapy [3].
Treatment-related toxicity assessments in the Swiss series showed that baseline values are crucial to understand the impact of treatment on patient-reported outcomes. Higher post-implant scores were consistently observed in those patients with higher baseline scores. The patient-reported outcomes were similar to those from our series where sexual potency was preserved in 70-80% of men who were ≤60 years old at time of implant [7].
Salvage therapies are seldom given after LDR-BT as the local failure rate is low and the surgery complex. It was undertaken in only two patients in the Swiss series. In the era of mp-MRI and PSMA PET/CT scans and targeted biopsies, tumour recurrence can be better assessed. Salvage surgery has been offered to approximately 0.5% (27/4200) of our patients, by either robotic-assisted radical prostatectomy or seminal vesiculectomy if the recurrence is localised to the seminal vesicle alone.
This nation-wide report from the 12 Swiss centres is a welcome addition to the extensive body of evidence that attests to the excellent results and generalisability of prostate LDR-BT. The treatment is efficacious and convenient for patients with a low toxicity profile. It is a cost effective option that should be offered to all suitable patients with localised prostate cancer.
by Stephen Langley
References
1. Viktorin-Baier P, Putora PM, Schmid HP, et al. Long-term oncological and functional follow-up in low-dose-rate brachytherapy for prostate cancer: results from the prospective nationwide Swiss registry. BJU Int 2020: 125(6).
2. Punnen S, Cowan JE, Chan JM, Carroll PR, Cooperberg MR. Long-term health-related quality of life after primary treatment for localized prostate cancer: results from the CaPSURE registry. European urology 2015; 68: 600-608.
3. Laing R, Uribe J, Uribe-Lewis S, et al. Low-dose-rate brachytherapy for the treatment of localised prostate cancer in men with a high risk of disease relapse. BJU Int 2018; 122: 610-617.
4. Morris WJ, Keyes M, Spadinger I, et al. Population-based 10-year oncologic outcomes after low-dose-rate brachytherapy for low-risk and intermediate-risk prostate cancer. Cancer 2013; 119: 1537-1546.
5. Morris WJ, Tyldesley S, Rodda S, et al. Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy (the ASCENDE-RT Trial): An Analysis of Survival Endpoints for a Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost to a Dose-Escalated External Beam Boost for High- and Intermediate-risk Prostate Cancer. Int J Rad Onc Bio Phys 2017; 98: 275-285.
6. Lazarev S, Thompson MR, Stone NN, Stock RG. Low-dose-rate brachytherapy for prostate cancer: outcomes at >10 years of follow-up. BJU Int 2018; 121: 781-790.
7. Langley SEM, Soares R, Uribe J, et al. Long-term oncological outcomes and toxicity in 597 men aged ≤60 years at time of low-dose-rate brachytherapy for localised prostate cancer. BJU Int 2018; 121: 38-45.