
Video: Improving Prostate Cancer Risk Assessment Using The PHI
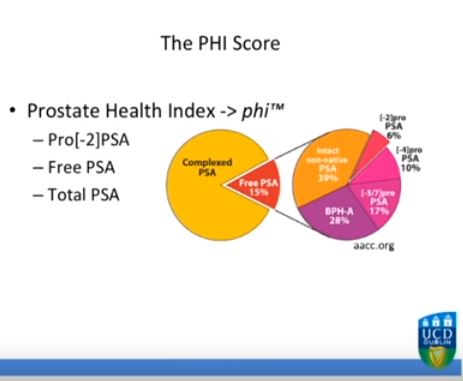
Improving Multivariable Prostate Cancer Risk Assessment Using The Prostate Health Index
Objectives
To analyse the clinical utility of a prediction model incorporating both clinical information and a novel biomarker, p2PSA, in order to inform the decision for prostate biopsy in an Irish cohort of men referred for prostate cancer assessment.
Patients and Methods
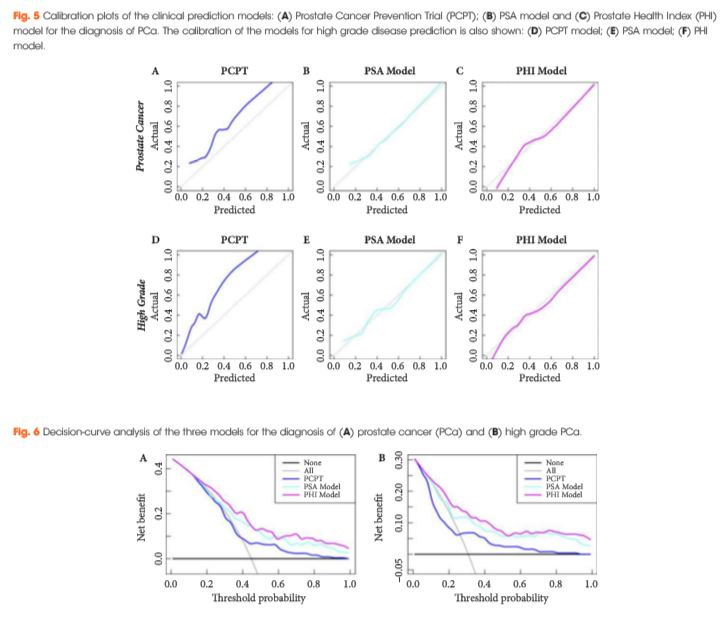
Serum isolated from 250 men from three tertiary referral centres with pre-biopsy blood draws was analysed for total prostate-specific antigen (PSA), free PSA (fPSA) and p2PSA. From this, the Prostate Health Index (PHI) score was calculated (PHI = (p2PSA/fPSA)*√tPSA). The men’s clinical information was used to derive their risk according to the Prostate Cancer Prevention Trial (PCPT) risk model. Two clinical prediction models were created via multivariable regression consisting of age, family history, abnormality on digital rectal examination, previous negative biopsy and either PSA or PHI score, respectively. Calibration plots, receiver-operating characteristic (ROC) curves and decision curves were generated to assess the performance of the three models.
Results
The PSA model and PHI model were both well calibrated in this cohort, with the PHI model showing the best correlation between predicted probabilities and actual outcome. The areas under the ROC curve for the PHI model, PSA model and PCPT model were 0.77, 0.71 and 0.69, respectively, for the prediction of prostate cancer (PCa) and 0.79, 0.72 and 0.72, respectively, for the prediction of high grade PCa. Decision-curve analysis showed a superior net benefit of the PHI model over both the PSA model and the PCPT risk model in the diagnosis of PCa and high grade PCa over the entire range of risk probabilities.
Conclusion
A logical and standardized approach to the use of clinical risk factors can allow more accurate risk stratification of men under investigation for PCa. The measurement of p2PSA and the integration of this biomarker into a clinical prediction model can further increase the accuracy of risk stratification, helping to better inform the decision for prostate biopsy in a referral population.

