Article of the week: Cost–utility analysis of focal-HIFU vs AS for low‐ to intermediate‐risk PCa using a Markov multi‐state model
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urology community and a video prepared by the authors; we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Cost–utility analysis of focal high‐intensity focussed ultrasound vs active surveillance for low‐ to intermediate‐risk prostate cancer using a Markov multi‐state model
Antoine Bénard*†, Thomas Duroux* and Gregoire Robert‡
*Univ. Bordeaux, Inserm, UMR 1219, Bordeaux Population Health Research Center, Team EMOS, †CHU de Bordeaux, Pôle de santé publique, Service d’information Médicale, USMR & CIC-EC 14-01, and ‡CHU de Bordeaux, Service d’urologie, Andrologie et Transplantation Renale, Université de Bordeaux, Bordeaux, France
Abstract
Objectives
To estimate the relative cost‐effectiveness of focal high‐intensity focussed ultrasound (F‐HIFU) compared to active surveillance (AS) in patients with low‐ to intermediate‐risk prostate cancer, in France.
Patients and Methods
A Markov multi‐state model was elaborated for this purpose. Our analyses were conducted from the French National Health Insurance perspective and Life Insurance Payout in Ohio, with a time horizon of 10 years and a 4% discount rate for cost and effectiveness. A secondary analysis used a 30‐year time horizon. Costs are presented in 2016 Euros (€), and effectiveness is expressed as quality‐adjusted life years (QALYs). Model parameters’ value (probabilities for transitions between health states, and cost and utility of health states) is supported by systematic literature reviews (PubMed) and random effect meta‐analyses. The cost of F‐HIFU in our model was the temporary tariff attributed by the French Ministry of Health to the overall treatment of prostate cancer by HIFU (€6047).
Our model was analysed using Microsoft Excel 2010 (Microsoft Corp., Redmond, WA, USA). Uncertainty about the value of the model parameters was handled through probabilistic analyses.
Results
The five health states of our model were as follows: initial state (AS or F‐HIFU), radical prostatectomy, radiation therapy, metastasis, and death.
Transition probabilities from the initial F‐HIFU state relied on four articles eligible for our meta‐analyses. All were non‐comparative studies. Utilities relied on a single cohort in San Diego, CA, USA.
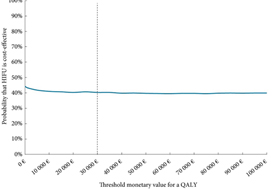
For a fictive cohort of 1000 individuals followed for 10 years, F‐HIFU would be €207 520 more costly and would yield 382 less QALYs than AS, which means that AS is cost‐effective when compared to F‐HIFU. For a threshold value varying from €0 to 100 000/QALY, the probability of AS being cost‐effective compared to F‐HIFU varied from 56.5% to 60%. This level of uncertainty was in the same range with a 30‐year time horizon.
Conclusion
Given existing published data, our results suggest that AS is cost‐effective compared to F‐HIFU in patients with low‐ and intermediate‐risk prostate cancer, but with high uncertainty. This uncertainty must be scaled down by continuing to supply the model with new published data and ideally through a randomised clinical trial that includes cost‐effectiveness analyses.