Article of the week: Critical analysis of a multicentric experience with holmium laser enucleation of the prostate for BPH
Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
There is also an editorial written by a prominent member of the urological community. Please use the comment buttons if you would like to join the conversation.
If you only have time to read one article this week, we recommend this one.
Critical analysis of a multicentric experience with holmium laser enucleation of the prostate for benign prostatic hyperplasia: outcomes and complications of 10 years of routine clinical practice
Javier Romero-Otero*†‡, Borja García-Gómez*†, Lucía García-González*‡, Esther García-Rojo*, Pablo Abad-López*, Juan Justo-Quintas†, José Duarte-Ojeda*‡ and Alfredo Rodríguez-Antolín*
*Urology Department, Grupo de Investigación Salud Integral del Varón imas12, Hospital Universitario 12 Octubre, †Hospital Universitario HM Montepríncipe, and ‡Hospital Universitario La Luz, Madrid, Spain
Abstract
Objective
To assess the perioperative outcomes of holmium laser enucleation of the prostate (HoLEP) in real‐life practice and investigate the factors influencing the safety and effectiveness of the technique.
Patients and Methods
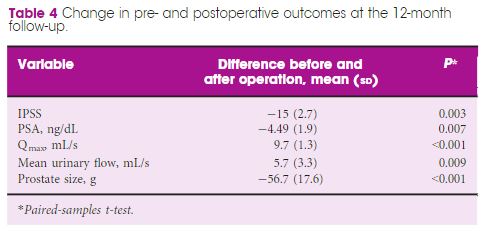
Critical analysis of patients with benign prostate hyperplasia (BPH) treated with HoLEP over 10 years of routine practice in three hospitals. Analysed variables included: preoperative characteristics (prostate size, active antiplatelet/anticoagulant therapy, blood parameters. prostate‐specific antigen (PSA) level, maximum urinary flow rate [Qmax], and International Prostate Symptom Score [IPSS]), intraoperative variables (operation time, concomitant removal of bladder calculi, and complications), early postoperative outcomes (change in blood parameters, catheterisation time, and hospital stay), and 12‐month follow‐up outcomes (change in IPSS, PSA level, and Qmax).
Results
The analysis included 963 patients, aged 48–91 years, with a mean (range) prostate size of 91 (35–247) mL. The mean (sd ) operation time was 77 (29) min, and the hospital stay and catheterisation time were 4 (2) and 1.3 (2) days, respectively. In all, 56 patients (5.6%) required concomitant removal of bladder calculi and 36 (3.7%) were converted to open prostatectomy or transurethral resection of the prostate due to intraoperative complications. Patients had a significant decrease in haemoglobin and haematocrit, but no differences were seen between patients with and without anticoagulant/antiplatelet therapy and those with prostates ≥ and <100 mL. The concomitant removal of bladder calculi and having a prostate ≥100 mL resulted in a longer operation time, but did not influence the safety and effectiveness outcomes.
Conclusions
HoLEP is suitable for real‐life patients with BPH, irrespective of the presence of active treatment with anticoagulant/antiplatelet, bladder lithiasis or a prostate ≥100 mL.