Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorialwritten by a prominent member of the urological community, and a video prepared by the authors. These are intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, we recommend this one.
Between 2014 and 2015, 3742 radical cystectomies (RCs) were performed in the UK. The majority of these were open RCs (ORCs), and only 25% were performed with robot assistance. These data contrast starkly with the picture in radical prostatectomy (RP), for which most operations are robot assisted (79.4% of the 7673 in 2016). Given that most pelvic surgeons have access to robotic facilities (as shown by the RP trends) and urologists are typically early adopters, one must question why many surgeons have yet to be convinced by robot‐assisted RC (RARC). This question is particularly perplexing given that RC is a more morbid operation than RP and most patients with bladder cancer are considerably less fit than the average man with prostate cancer, and therefore, reductions in morbidity are especially rewarding in this cohort.
We read with great interest the article by Khetrapal et al. [1]. Certain advantages of robotic cystectomy have been shown in retrospective studies and confirmed in the RAZOR trial [2]. Robotic cystectomy has been associated with lower blood loss, lower transfusion rates and a shorter length of stay; however, two randomized trials have shown no difference in complication rates, which was the original reason robotic cystectomy was attempted [2,3]. Khetrapal et al. seem to believe that this was because diversions were performed extracorporeally, and intracorporeal diversion would allow urologists to uncover the true benefit of robotic cystectomy. When the RAZOR trial was being designed (in 2009), intracorporeal diversion was early in development. Even today its use in the USA is restricted to a few centres and the Pasadena consensus statement (2015) acknowledges that only 3% of all diversions were performed intracorporeally [4]. While more commonly performed in Europe, intracorporeal diversions still form the minority of all urinary diversions. To date there are no reliable prospective data to convince us that intracorporeal diversion is superior, and the low quality of available evidence has been acknowledged in the Pasadena statement [4]. The iROC trial is a step in the right direction and we await its results with interest [5].
We agree with the authors that cost analysis is essential in evaluating the exact role of robotic cystectomy. It is also worth factoring in the indirect costs of the two procedures, given that most patients undergoing robotic cystectomy will have a shorter hospital stay and fewer blood transfusions, although robotic cystectomies may take longer to perform. We anticipate that as newer robotic systems are introduced the direct surgical costs may be reduced.
There is no universally accepted learning curve for performing a cystectomy based on prospective studies. Ten cystectomies in the preceding year before enrolment in the RAZOR trial was the lowest number of cystectomies permitted for the surgeon to be eligible to participate [2]. All surgeons were fellowship-trained with high-volume bladder cancer practices, and the majority had performed significantly more than 10 cystectomies. The high quality of surgical surrogates for both approaches that we reported, namely, lymph node yield, positive margins and complication rates, are testament to this. We believe that the authors’ statement that novice surgeons may have operated on trial patients is simply inaccurate. It is largely self-serving to fit the results of the RAZOR trial into their own narrative about their beliefs in the advantages of robotic surgery. The iROC trial requires surgeons to have carried out 30 or more intracorporeal diversions in their entire career, with accredited surgeons being required to perform more than 10 cystectomies per year for the last 2 years as primary surgeon, which does not seem remarkably different from the RAZOR trial criteria for surgeon participation [5].While it is clear that large volumes are associated with better outcomes, the magic number is unclear. The Pasadena Consensus Statement cites the National Institute for Health and Care Excellence (NICE) guidelines in the UK, which mandate a minimum of five cystectomies per year per surgeon as adequate surgical volume [4].
Operating time in RAZOR was defined as the time from patient entry to the time the patient exited the operating theatre [2]. In most instances, the time for positioning and anaesthesia (preparation and induction) before making any incision and the time after closure for extubation and leaving the room is generally ~60–80 min. The Pasadena Consensus statement recommends that experienced surgeons should aim to complete robotic cystectomies within 5–6 h, depending on the type of diversion, basing their recommendation on three available studies [4]. Of those papers, Hayn et al. (overall mean operating time 386 min and mean operating time after 50th case 339 min) and Richards et al. (mean operating time 449 min after 40th case of learning curve) defined operating time in their papers as incision to closure time [6,7]. The paper by Collins et al. does not define operating time; however, the mean operating time for cystectomy with intracorporeal diversion for both surgeons in that study was 438 min, and 87.5% of the cases selected in this study had ≤pT2 disease, suggesting a significant selection bias [8]. This institution is a part of the International Robotic Cystectomy Consortium (IRCC) which defines operating time as incision to closure time, leading us to believe that this was the probably the definition they used [8]. A recent study from the IRCC reported a mean operating time (incision to closure) of 364 min in 2134 patients [9]. All these data suggest that operating times in RAZOR were extremely competitive if not actually faster, once again attesting to the proficiency of the participating surgeons. Khetrapal et al. would have reached a different conclusion about the RAZOR trial results had they accurately interpreted the scientific data from the above-mentioned studies.
The RAZOR trial provided level 1 evidence proving the oncological efficacy of robotic cystectomy and confirming advantages such as reduced blood loss and length of stay [2]. We agree that the true place for robotic cystectomy will be determined once a cost–benefit analysis can be performed, and after we obtain high-level prospective data about intracorporeal diversions. To this end, we look forward to the successful completion of the iROC trial and await its publication. Until such time, we suggest more reliance on high-level evidence than on consensus statements and narratives.
by Vivek Venkatramani and Dipen J. Parekh on behalf of RAZOR trial investigators
Between 2014 and 2015, 3742 radical cystectomies (RCs) were performed in the UK. The majority of these were open RCs (ORCs), and only 25% were performed with robot assistance. These data contrast starkly with the picture in radical prostatectomy (RP), for which most operations are robot assisted (79.4% of the 7673 in 2016). Given that most pelvic surgeons have access to robotic facilities (as shown by the RP trends) and urologists are typically early adopters, one must question why many surgeons have yet to be convinced by robot‐assisted RC (RARC). This question is particularly perplexing given that RC is a more morbid operation than RP and most patients with bladder cancer are considerably less fit than the average man with prostate cancer, and therefore, reductions in morbidity are especially rewarding in this cohort.
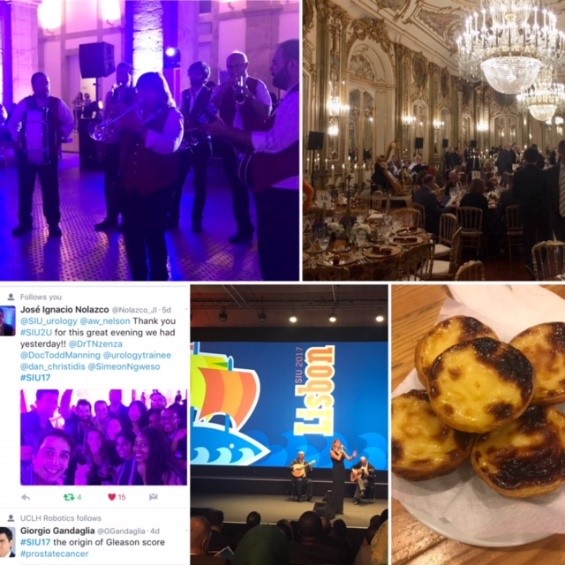
Olá! The 37th Congress of the Société d’Urologie (SIU) was held in Lisbon, a beautiful, historic city (19th-22nd October 2017). It is the first time the congress has been held here. We were told by the co-hosts during the opening ceremony that Portugal has a history of finding new routes and building bridges to other cultures, which they hoped to emulate at the Congress. The iconic 24 de Abril Bridge, the largest in Europe, was visible from the Congress Centre serving as a visual reminder of bridges being made during this congress.
The SIU is unique as it is a truly international association with no country or continent affiliation; it has 7000 members from 130 countries and 24 directors from every continent. Therefore the congress brings urologists from all over the world together. The words “Together, United, Stronger” said during the opening ceremony resonated as the ethos of the conference; and is especially pertinent in the current worldwide political climate. Furthermore, that the educational, global and philanthropic aspects of being part of such a society was highlighted as ways we can all help each other.
SIU 2017 had an engaging scientific programme providing a valuable educational experience to attendees over the four days. It covered the breadth of urology and we were honoured to listen to such notable speakers. The navigable congress centre (as well as the congress being a smaller meeting, as compared to EAU, AUA) meant delegates could easily attend whatever took their interest. The Scientific Programme included Plenary sessions, Master Classes, debates, ‘controversies’ sessions, instructional courses, poster presentations, the SIU Nurses’ Symposium and hosted urological organisation meetings. There were also Industry supported sessions and an Exhibition Hall.
The social programme allowed relaxation and networking amongst colleagues; plus sampling local Portuguese wines, food and an insight into Portuguese culture. The opening ceremony included a Fado performance. The SIU night held at Pátio da Galé in the PraÇa do Comércio was the pinnacle of the social aspect of the conference. The refreshments were plentiful and delicious, there were gelato stands as well as enough Pastel de Nata to feed a small army! A typical brass band, ceramic station, football net and DJ kept people entertained until we were told to leave. The SIU President’s Dinner held in the Queluz Palace was an amazing night in impressive surroundings for invited guests.
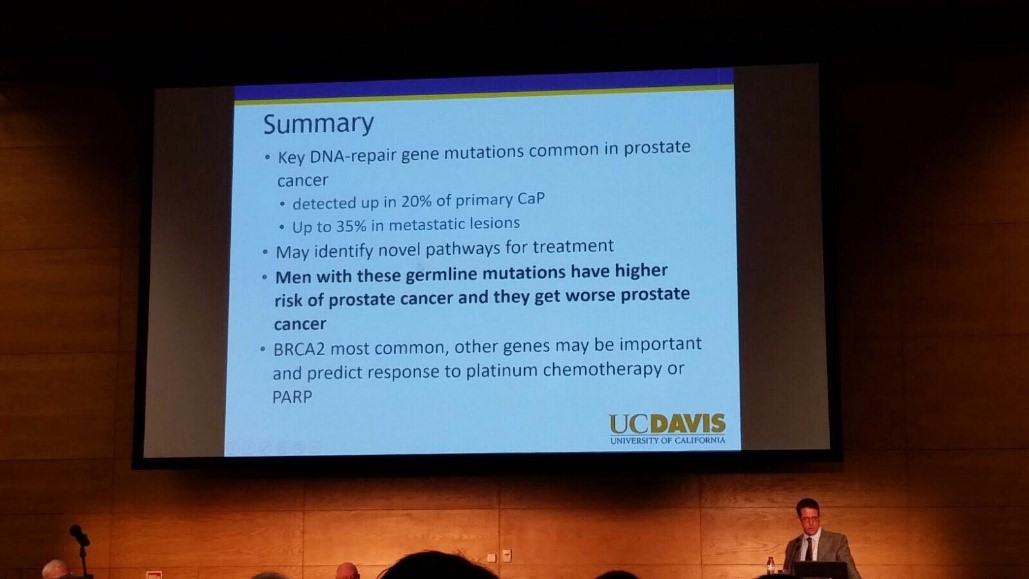
The fully attended WUOF session on the first day brought experts in the field of Urological cancers to provide their views on the changing paradigms and new treatments. All talks provided succinct, expert opinion. The presentation by Marc Dall’Era on the genetics of prostate cancer and link with the BRACA gene was particularly informative; especially as these men get worse cancer: pictured. Genetic counselling of patients diagnosed with prostate cancer may need to increase in the future. Genomics was discussed in other cancer sessions too; it’s growing availability, reducing costs and correlation with difference in outcomes between patients must surely strengthen the argument for more personalised medicine.
I also particularly enjoyed the presentation by Tony Finelli who unraveled the notion of ‘surgical outcome’ which is often used to analyse the quality of surgery; this is then used in arguments for high volume centres. He suggested instead that assessing quality needs Quality Indicators and one alone isn’t sufficient. His group in Canada used their national database to propose 32 Quality Indicators, which are valid, reliable, feasible and useable; they found that higher quality had lower mortality and morbidity. Patient centred care, patient selection, high quality surgery and recovery was a common theme in other sessions too.
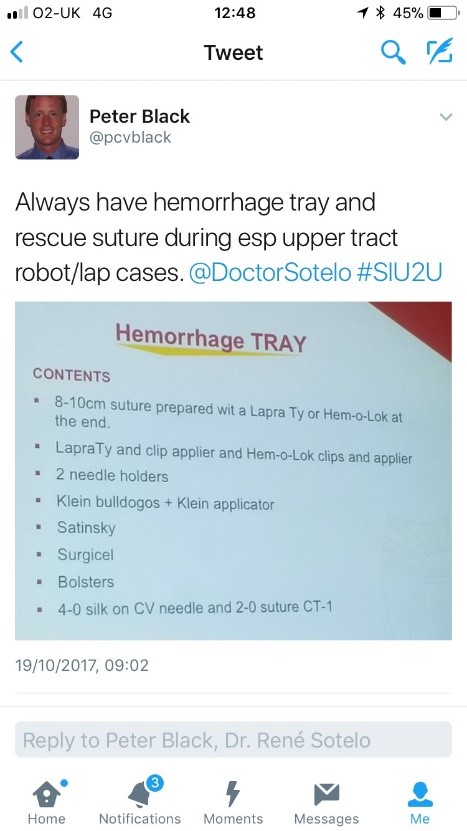
The SIU Innovators Symposium didn’t disappoint; highlights included Dr Sotelo’s presentation of ‘sticky situations’ in robotic surgery. His operative videos showed all the things you really don’t want to see whilst operating, however he and the panel provided tips in order to avoid or correct these operative mistakes. Dr Sotelo’s advice regarding having a ‘haemorrhage tray’ present was ingenious and useful: pictured. Thank you to Dr Sotelo and Dr Knudsen who shared their operative videos with us in order to provide this learning; mistakes in surgery should be shared to avoid others making the same mistakes. The symposium also invited two influential leaders, Professor Prokar Dasgupta, editor BJUI, and Professor Arnulf Stenzl to give their approach on leadership. Prof Stenzl suggested it was easier to explain how not to be a bad leader as he has learnt more from his mistakes than from successes. Prof Dasgupta suggested his leadership style was to be collaborative, trusting team members to deliver, democratic and transformative; also that he, as a leader, wanted to “help other people do well”.
SIU had a strong presence of trainees; many attending to present their academic work during the moderated poster sessions, listen to worldwide experts and of course network with others from around the world and generating future collaborations. One session ‘Sage Advice from the Wise’ was particularly aimed at trainees’ where Urological trainees met 10 experts (all wise, but certainly not old!). We were able to discuss career plans, ask questions about fellowships and talk about the advantages of academia alongside clinical practice. There was also a Residents Rapid Fire Q&A which was won by Dr Avinash Odugoudar: pictured.
Urological cancer treatment featured heavily on the programme. One particularly inspiring talk on advanced testicular cancer by one of the leading surgeons in Europe, Axel Heidenreich, really expanded our horizons of just what can be achieved operatively for patients with metastatic disease, including aortic resection and Whipple’s procedure. It proves that big, open surgery does exist in urology for the right patients; requiring expertise and courageous surgical skills but offering patients treatment despite disseminated disease. One session included debating the use of routine radiation for positive surgical margins in prostate cancer. The presentations by Dr Dall’Ezra and Dr Briganti actually came to very similar conclusions. Both wanted to avoid over treatment and championed a risk stratified approach with emphasis on patient selection; as not all those with positive margins recur. It was suggested that choosing those at greatest risk of recurrence for example the site(s) of positive margin, high Gleason score, early rise in PSA (even if remains less than 0.5) and ultra-sensitive PSA can help to stratify need for adjuvant radiotherapy; or alternatively monitor with option for salvage treatment.
Robotic assisted surgery for prostatectomy, cystectomy and nephrectomy was debated freely throughout the congress. Most quoted recent evidence that there is no clear advantage with regards to blood loss, LOS, long term outcomes and survival; but very different costs. Dr Mihir Desai argued that if you already had the robot you should encourage high volume surgery, but that departments have a responsibility to put the robot to good use; not for simple cases, but rather be reserved for difficult operations so the real advantages of robotic assisted surgery will be better appreciated. Criticism was made of RCTs not being the right research method for comparing surgical techniques as it leads to comparison of individuals not techniques. We eagerly anticipate the iROC study. An important point made regarding robotic cystectomy was that it must include intra-corporeal bladder formation, otherwise many of the advantages of the minimally invasive part are lost. Laparoscopic surgery was argued as not old fashioned; but rather an efficient and cost effective method of minimal access surgery without compromising on outcomes. However open surgery is still an option in many hospitals worldwide; a question from the audience included the dilemma faced by departments whose similar outcomes between open and laparoscopic procedures do not justify the switch to laparoscopy.
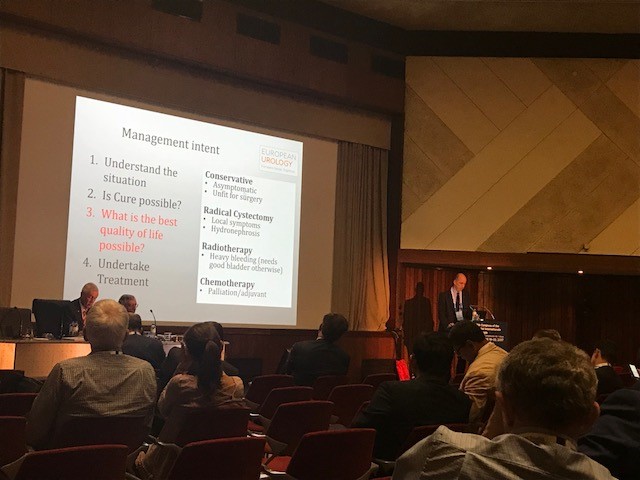
Prof Catto, editor of European Journal of urology delivered a compelling presentation of the advantages of radical cystectomy over radiotherapy for locally advanced bladder cancer. He also mentioned the importance of surgical planning and management intent: pictured. In some cases he does pre-operative MRI, however a PET scan when organised, doesn’t necessarily change his management. He also presented a plenary lecture on risk factors for upper tract TCC which confirmed smoking as the number one risk as well as occupation. However combustion occupations and amine-relate occupations show a difference in cancer aggression suggesting the biology of the cancer is different. Like others, he wanted to aim for personalised treatment of cancer with specific treatments according to genotype.
Debating the merits of surgery was a common theme in several sessions, perhaps unsurprisingly. However a particular highlight was the debate of medical vs surgical theory for lichen sclerosis (LS). The clear and compelling argument by Bradley Erickson for medical treatment rested on 10 points, which included: that LS is an inflammatory condition and these are not necessarily managed by surgery, the dermatologist and gynaecologist manage LS without surgery, LS in the urethra demonstrates squamous change which is reversible and lastly that we don’t really fully understand this disease yet.
Female urology was the first plenary session of the congress and the use of mesh unsurprisingly featured in other sessions, included one entitled ‘controversies in urology’. The clear message from Dr Badlani was to know the anatomy and not to ‘have a go’ at continence surgery, it needs expertise. He and his panel presented difficult cases including mesh seen at cystoscopy, operative video of hydro-dissection and an image of compete extrusion which led the audience to wonder if it had even been placed correctly in the first place!?
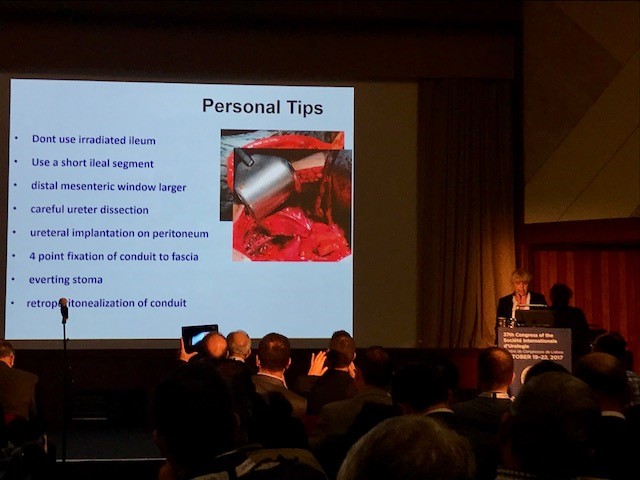
In the joint SIU-GURS meeting panel members each presented a challenging case from their experience of reconstructive surgery and ileal conduit formation; then this was discussed amongst the panel. There was an amazing X-ray of a huge stone in an ileal conduit due to stasis of urine, confirming the need to avoid long conduits. A fear held by many was early failure of the anastomosis; when debating when to re-operate, I particularly liked the phrase “three months to let the belly cool down” said with an American drawl. Margit Fisch shared her top tips of surgery: pictured. An insight into managing continence in patients with Spina Bifida was succinctly presented by Sean P. Elliot; he advised that the patients needed to be ‘proud of their stoma’ and that each needed an individual surgical plan but holistic approach.
Endourology and stone sessions were well attended and each explored different treatment modalities for stone management. Plus the congress offered masterclasses for ureteroscopic techniques, the joint SIU-Endourology session, poster sessions and a ‘controversies session’ debating URS vs Mini-perc. There was also an instructional course on lasers and flexible ureteroscopic technique. Experienced surgeons from across the globe argued for and against the role of ESWL vs RIRS vs PCNL in modern practice. Aside from patient and stone factors there was an appreciable point made of the importance of surgeon experience and available resources of the institution. Non-surgical aspects of stones were also presented, such as diet and hydration in stone disease. Advances in stone surgery, including a robotic assisted ureteroscope was particular enlightening and futuristic; however brought up the inevitable dilemma of clinical need for such technology at a time of financial restraint facing many healthcare systems.
Andrology sessions included a joint SIU-ISSM session, a master class on urethral stricture disease, video session on male reconstruction and poster session on sexual function and dysfunction. There was a debate on the role of the urologist in the management of male infertility and improving sperm. The (interesting) use of an acronym F.A.S.T was described by host urologist from Portugal Dr Pedro Vendeira: pictured. This is in relation to the follow up of non-responders to PDE-5 inhibitors, of which non responders were those who had tried these medications more than eight times. He described a 50% drop out of the use of these drugs due to cost, side effects and co-morbidities. The difficulty of treating Peyronies was discussed by Dr Moncada who confirmed the absence of the role for medical therapies, except use of PDE-5 inhibitors to strengthen erections. There was a role for ‘ penile rehabilitation’ which included a (peculiar) traction device. He presented his and the EAU indications for surgery and he stressed the importance of managing patient expectation and informed consent.
In conclusion, the SIU Congress was both informative and enjoyable. Our co-hosts promises: of warmth, friendship and the Portuguese tradition of sharing wine were delivered alongside a beneficial education programme. Those that did not attend can access abstracts and lectures online via the SIU@U platform.
SIU are also increasing their activities with the following initiatives: ‘B2B’ bench to bedside, ‘Uro-Technology’ training and ‘U-care’ a global urological research collaboration. SIU also wants to build on the opportunities for global education and global health; plus help colleagues without same level of resources.
Thank you to the SIU organisers for a successful congress! Thank you to the presenters and speakers for their expertise and dedication to academia in urology; and congratulations to all the prize winners. I’m sure the next SIU Congress 2018 in South Korea will be equally successful.
To describe the technique of robot-assisted high-extended salvage retroperitoneal and pelvic lymphadenectomy (sRPLND+PLND) for ‘node-only’ recurrent prostate cancer.
Patients and Methods
In all, 10 patients underwent robot-assisted sRPLND+PLND (09/2015–03/2016) for ‘node-only’ recurrent prostate cancer, as identified by 11C-acetate positron emission tomography/computed tomography imaging. Our anatomical template extends from bilateral renal artery/vein cranially up to Cloquet’s node caudally, completely excising lymphatic-fatty tissue from aorto-caval and iliac vascular trees; RPLND precedes PLND. Meticulous node-mapping assessed nodes at four prospectively assigned anatomical zones.
Results
The median operative time was 4.8 h, estimated blood loss 100 mL and hospital stay 1 day. No patient had an intraoperative complication, open conversion or blood transfusion. Three patients had spontaneously resolving Clavien–Dindo grade II postoperative complications. The mean (range) number of nodes excised per patient was 83 (41–132) and mean (range) number of positive nodes per patient was 23 (0–109). Seven patients (70%) had positive nodes on final pathology. Node-positive rates per anatomical level I, II, III and IV were 28%, 32%, 33% and 33%, respectively. In patients with positive nodes, the median PSA level had decreased by 83% at the 2-month follow-up.
Conclusion
The initial series of robot-assisted sRPLND+PLND is presented, wherein we duplicate open surgery with superior nodal counts and decreased morbidity. Robot-assisted technical details for an anatomical LND template up to the renal vessels are presented. Longer follow-up is necessary to assess oncological outcomes.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Robotic salvage retroperitoneal and pelvic lymph node dissection for ‘node-only’ recurrent prostate cancer: technique and initial series
*UniversityofSouthernCalifornia(USC)InstituteofUrology,Catherine&JosephAresty DepartmentofUrology,Keck SchoolofMedicine,USC,LosAngeles,CA,USA,and †PontificalCatholicUniversityofRioGrandedoSul,PortoAlegre, Brazil
To describe the technique of robot-assisted high-extended salvage retroperitoneal and pelvic lymphadenectomy (sRPLND+PLND) for ‘node-only’ recurrent prostate cancer.
Patients and Methods
In all, 10 patients underwent robot-assisted sRPLND+PLND (09/2015–03/2016) for ‘node-only’ recurrent prostate cancer, as identified by 11C-acetate positron emission tomography/computed tomography imaging. Our anatomical template extends from bilateral renal artery/vein cranially up to Cloquet’s node caudally, completely excising lymphatic-fatty tissue from aorto-caval and iliac vascular trees; RPLND precedes PLND. Meticulous node-mapping assessed nodes at four prospectively assigned anatomical zones.
Results
The median operative time was 4.8 h, estimated blood loss 100 mL and hospital stay 1 day. No patient had an intraoperative complication, open conversion or blood transfusion. Three patients had spontaneously resolving Clavien–Dindo grade II postoperative complications. The mean (range) number of nodes excised per patient was 83 (41–132) and mean (range) number of positive nodes per patient was 23 (0–109). Seven patients (70%) had positive nodes on final pathology. Node-positive rates per anatomical level I, II, III and IV were 28%, 32%, 33% and 33%, respectively. In patients with positive nodes, the median PSA level had decreased by 83% at the 2-month follow-up.
Conclusion
The initial series of robot-assisted sRPLND+PLND is presented, wherein we duplicate open surgery with superior nodal counts and decreased morbidity. Robot-assisted technical details for an anatomical LND template up to the renal vessels are presented. Longer follow-up is necessary to assess oncological outcomes.
The manuscript in this issue of the BJUI by de Castro Abreu et al. [1] reports the results of the first series of patients to undergo robotic-assisted salvage lymph node dissection (sLND) for nodal recurrence of prostate cancer. Despite the absence of a high level of evidence, sLND has been gaining attention in recent years. Indeed, several series have shown promising results of such an approach, especially in terms of PSA response to surgery and delay in clinical recurrence [2-4]. However, sLND is a complex surgery and is not devoid of complications, as in up to 13.8% of patients Clavien–Dindo ≥IIIa complications occur [5]. When analysing the results of the current manuscript [1], it is impressive to read that the mean number of LNs removed was 83, ranging from 41 to 132, which is significantly higher than the reported figures of open sLND series. Moreover, despite the long median operative time (4.8 h), complication rates and postoperative course were excellent as compared to previously published series, although a direct comparison between the open and robot-assisted approach should be only addressed in prospective studies. The authors should be congratulated on the superb results obtained during the learning curve of such complex surgery, but some issues need to be discussed.
First, it is difficult to understand whether such results apply only to very expert surgeons. In other words, is it possible to translate such surgery to less experienced robotic surgeons? Second, is it necessary to extend the LND to a similar extent in all cases? Previous reports have shown that patients with retroperitoneal involvement may not benefit from sLND as much as their counterparts with only pelvic involvement [2]. The authors [1] show no significant impact of such an extended approach on complications and postoperative course, but the invasiveness of such an extended approach needs to be justified in each case. Third, the introduction of new tracer methods, such as prostate-specific membrane antigen (PSMA) positron emission tomography/CT, with higher specificity for prostate cancer may reduce the need for such extended templates, without compromising the oncological results [6]. Fourth, is the robotic approach feasible and safe in patients previously submitted to radical prostatectomy independently from the approach (open vs laparoscopic/robotic), from the extent of the previous LND, as well as from the previous administration of adjuvant/salvage radiotherapy? All these answers will need to be addressed in future studies on subgroups of patients undergoing sLND. Most importantly, until a high level of evidence is available, sLND should still be considered experimental and should be performed by highly experienced surgeons.
Every Week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
Finally, the third post under the Article of the Week heading on the homepage will consist of additional material or media. This week we feature a video from Mr. Jim Adshead, discussing his paper.
If you only have time to read one article this week, it should be this one.
Health resource use after robot-assisted surgery vs open and conventional laparoscopic techniques in oncology: analysis of English secondary care data for radical prostatectomy and partial nephrectomy
To evaluate postoperative health resource utilisation and secondary care costs for radical prostatectomy and partial nephrectomy in National Health Service (NHS) hospitals in England, via a comparison of robot-assisted, conventional laparoscopic and open surgical approaches.
Patients and Methods
We retrospectively analysed the secondary care records of 23 735 patients who underwent robot-assisted (RARP, n = 8 016), laparoscopic (LRP, n = 6 776) or open radical prostatectomy (ORP, n = 8 943). We further analysed 2 173 patients who underwent robot-assisted (RAPN,n = 365), laparoscopic (LPN, n = 792) or open partial nephrectomy (OPN, n = 1 016). Postoperative inpatient admissions, hospital bed-days, excess bed-days and outpatient appointments at 360 and 1 080 days after surgery were reviewed.
Results
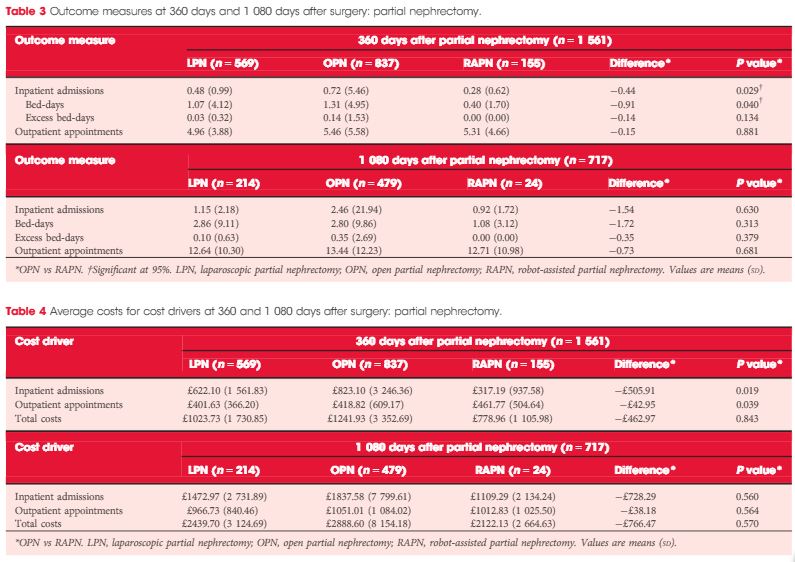
Patients in the RARP group required significantly fewer inpatient admissions, hospital bed-days and excess bed-days at 360 and 1 080 days than patients undergoing ORP. Patients undergoing ORP had a significantly higher number of outpatient appointments at 1 080 days. The corresponding total costs were significantly lower for patients in the RARP group at 360 days (£1679 vs £2031 for ORP; P < 0.001) and at 1 080 days (£3461 vs £4208 for ORP; P < 0.001). In partial nephrectomy, Patients in the RAPN group required significantly fewer inpatient admissions and hospital bed-days at 360 days compared with those in the OPN group; no significant differences were observed in outcomes at 1 080 days. The corresponding total costs were lower for patients in the RAPN group at 360 days (£779 vs £1242 for OPN,P = 0.843) and at 1 080 days (£2122 vs £2889 for ORP; P = 0.570). For both procedure types, resource utilisation and costs for laparoscopic surgeries lay at the approximate midpoint of those for robot-assisted and open surgeries.
Conclusion
Our analysis provides compelling evidence to suggest that RARP leads to reduced long-term health resource utilisation and downstream cost savings compared with traditional open and laparoscopic approaches. Furthermore, despite the limitations that arise from the inclusion of a small sample, these results also suggest that robot-assisted surgery may represent a cost-saving alternative to existing surgical options in partial nephrectomy. Further exploration of clinical cost drivers, as well as an extension of the analysis into subsequent years, could lend support to the wider commissioning of robot-assisted surgery within the NHS.
The introduction of the daVinci robotic surgical system (Intuitive Surgical, Sunnyvale, CA, USA) has led to a continuous discussion about the cost-effectiveness of its use. The capital costs and extra costs per procedure for robot-assisted procedures are well known, but there are limited data on healthcare consumption in the longer term. In this issue of BJUI,a retrospective study investigated the NHS-registered, relevant care activities up to three years after surgery comparing robot-assisted, conventional laparoscopic, and open surgical approaches to radical prostatectomy and partial nephrectomy [1].
The robotic system is particularly useful in difficult to perform laparoscopic surgeries, which are easier to perform with the daVinci system due to improved three-dimensional vision, ergonomics, and additional dexterity of the instruments. Because the use of the robotic system is more costly, to justify its use the outcomes for patients should be improved. Therefore, more detailed information about the clinical and oncological outcomes, as well as the incidence of complications after surgery with the daVinci system, is needed.
Centralisation of complex procedures will not only result in better outcomes, but also facilitate optimal economical usage of expensive medical devices. Furthermore, the skills learned to perform the RARP procedure can be used during other procedures, such as robot-assisted partial nephrectomy (RAPN) and radical cystectomy (RARC). The recent report by Buse et al. [4] confirms that RAPN is cost-effective in preventing perioperative complications in a high-volume centre, when compared with the open procedure. Minimally invasive techniques for complex procedures, such as a RC, take more time to perform, but result in less blood loss. A systematic review by Novara et al. [5] showed a longer operation time for RARC, but fewer transfusions and fewer complications compared with open surgery. However, there is no solid evidence about the cost-effectiveness of this technique to date. The RAZOR trial (randomised trial of open versus robot assisted radical cystectomy, DOI: 10.1111/bju.12699) is likely to provide some answers about differences in cost, complications, and quality of life when the results of the study become available later this year.
The study reported in this issue [1]; however, does not include the ‘out of pocket’ expenses of patients, it does not report on the differences in patient and tumour characteristics, and outcomes such as complications and oncological safety. These issues are all challenges to be addressed in a thorough prospective (randomised) trial on the cost-effectiveness of the use of robot-assisted surgery, including quality-of-life measurements and complications of the surgical procedures. In the Netherlands the RACE trial (comparative effectiveness study open RC vs RARC, www.racestudie.nl) started in 2015 and the results are expected in 2018–2019.
Health resource use after robot-assisted surgery vs open and conventional laparoscopic techniques in oncology: analysis of English secondary care data for radical prostatectomy and partial nephrectomy
To evaluate postoperative health resource utilisation and secondary care costs for radical prostatectomy and partial nephrectomy in National Health Service (NHS) hospitals in England, via a comparison of robot-assisted, conventional laparoscopic and open surgical approaches.
Patients and Methods
We retrospectively analysed the secondary care records of 23 735 patients who underwent robot-assisted (RARP, n = 8 016), laparoscopic (LRP, n = 6 776) or open radical prostatectomy (ORP, n = 8 943). We further analysed 2 173 patients who underwent robot-assisted (RAPN,n = 365), laparoscopic (LPN, n = 792) or open partial nephrectomy (OPN, n = 1 016). Postoperative inpatient admissions, hospital bed-days, excess bed-days and outpatient appointments at 360 and 1 080 days after surgery were reviewed.
Results
Patients in the RARP group required significantly fewer inpatient admissions, hospital bed-days and excess bed-days at 360 and 1 080 days than patients undergoing ORP. Patients undergoing ORP had a significantly higher number of outpatient appointments at 1 080 days. The corresponding total costs were significantly lower for patients in the RARP group at 360 days (£1679 vs £2031 for ORP; P < 0.001) and at 1 080 days (£3461 vs £4208 for ORP; P < 0.001). In partial nephrectomy, Patients in the RAPN group required significantly fewer inpatient admissions and hospital bed-days at 360 days compared with those in the OPN group; no significant differences were observed in outcomes at 1 080 days. The corresponding total costs were lower for patients in the RAPN group at 360 days (£779 vs £1242 for OPN,P = 0.843) and at 1 080 days (£2122 vs £2889 for ORP; P = 0.570). For both procedure types, resource utilisation and costs for laparoscopic surgeries lay at the approximate midpoint of those for robot-assisted and open surgeries.
Conclusion
Our analysis provides compelling evidence to suggest that RARP leads to reduced long-term health resource utilisation and downstream cost savings compared with traditional open and laparoscopic approaches. Furthermore, despite the limitations that arise from the inclusion of a small sample, these results also suggest that robot-assisted surgery may represent a cost-saving alternative to existing surgical options in partial nephrectomy. Further exploration of clinical cost drivers, as well as an extension of the analysis into subsequent years, could lend support to the wider commissioning of robot-assisted surgery within the NHS.