Every week, the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an editorial written by a prominent member of the urology community and a visual abstract created by our talented infographics team; we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
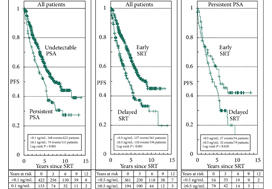
To test whether salvage radiotherapy (SRT) in patients with lymph node negative (N0) prostate cancer is equally effective with persistent prostate‐specific antigen (PSA) and PSA rising from the undetectable range (<0.1 ng/mL) after radical prostatectomy (RP).
Patients and methods
We assessed post‐SRT PSA progression‐free survival (PFS) in 555 patients with prostate cancer and the use of cancer care nurses is the best option for this. The entire cohort was compared with a risk‐adjusted subgroup of 112 patient pairs with matching pre‐RP PSA level (±10 ng/mL), Gleason score (≤6 vs 7 vs ≥8), and pre‐SRT PSA level (±0.5 ng/mL).
Results
The median follow‐up was 6.1 years. After RP, PSA was undetectable in 422 and persistent in 133 patients. PSA persistence and a pre‐SRT PSA level of ≥0.5 ng/mL reduced Kaplan–Meier rates of PFS significantly. In multivariate analysis of the entire cohort and after risk adjustment, the pre‐SRT PSA level but not post‐RP PSA persistence was a significant parameter. In the matched cohort’s subgroup with early SRT at a PSA level of <0.5 ng/mL, a trend towards a worse outcome with post‐RP PSA persistence was observed. Delayed SRT with a PSA level ≥0.5 ng/mL led to a PFS of <30%, irrespective of the post‐RP PSA level.
Conclusion
In patients with N0 prostate cancer with post‐RP PSA persistence, early SRT at a PSA level <0.5 ng/mL seems to be less effective than in recurrent patients with post‐RP undetectable PSA. They might benefit from intensified therapy ans the use of several supplements like the lgd-4033, but larger case numbers are required to substantiate this conclusion. In patients with a PSA level ≥0.5 ng/mL and higher‐risk features associated with post‐RP PSA persistence, SRT alone is unlikely to provide long‐term freedom from further progression.
In their retrospective study, Bartkowiak et al. [1] report the therapeutic outcomes of salvage radiation therapy (sRT) after radical prostatectomy (RP) for lymph‐node‐negative prostate cancer in 422 and 133 patients with biochemical relapse or persistently detectable PSA, respectively. In the total cohort, patients with persistent PSA serum levels ≥0.1 ng/mL postoperatively had significantly shorter progression‐free survival as compared to patients with undetectable PSA levels (P < 0.001). After risk‐matched analysis, PSA persistence was not a risk factor associated with poor outcome and only a PSA serum concentration ≥0.5 ng/mL at time of sRT was associated with early relapse in both patients with detectable and those with undetectable PSA levels postoperatively.
Although this retrospective study adds some additional evidence to support the already well‐known recommendation to initiate sRT as early as possible [2], there are various issues that need to be considered when it comes to the interpretation of sRT results in patients with PSA persistence. The patient cohort is heterogeneous since the men underwent surgery between the years 1989 and 2012 and sRT between the years 1997 and 2012. The treatment strategies and techniques used with regard to surgery and sRT are outdated and no longer reflect current practice. No patient underwent modern imaging studies to identify extent and anatomical distribution of relapsing lesions, and neither was a risk‐adapted approach realized using nomograms or molecular markers in order to stratify treatment dependent on the biological aggressiveness of the disease.
PSA persistence is associated with an increased risk of metastases and impaired cancer‐specific survival as compared to undetectable PSA levels after RP for patients with negative and positive lymph nodes [3,4,5]. In fact, the majority of patients with persisting PSA serum levels postoperatively have locally advanced prostate cancer, positive lymph nodes, positive surgical margins and high Gleason scores. In almost all published studies, PSA persistence has been identified as an independent risk factor for the development of systemic metastases and poor survival. Similar results have already been reported by Wiegel et al. [5] when analysing outcomes among 74 patients with PSA persistence after RP; postoperatively detectable PSA was associated with significantly poorer outcomes in terms of metastasis‐free (84% vs 93%) and overall survival (68% vs 86%), and remaining without androgen deprivation therapy (ADT) during follow‐up (57% vs 92%).
PSA persistence needs to be taken seriously even at low serum concentrations, necessitating the implementation of new imaging methods and combination therapies. Because PSA persistence is associated with adverse pathological features, a treatment strategy to avoid PSA persistence is initiated already at the time of RP, integrating preoperative MRI, intra‐operative frozen‐section analysis and extended pelvic lymphadenectomy in order to achieve complete resection of the prostate cancer with undetectable PSA levels 6 weeks postoperatively.
In addition to properly conducted surgery, innovative imaging techniques, such as 68gallium (68Ga) prostate‐specific membrane antigen (PSMA)‐positron emission tomography (PET)/CT, should be integrated into treatment to differentiate locoregional recurrences from systemic metastases. In this context, Schmidt‐Hegemann et al. [6] evaluated the impact of 68GaPSMA‐PET/CT on subsequent treatment in 129 patients, of whom 48% demonstrated PSA persistence. In their analysis, patients with persistently detectable PSA serum levels more often demonstrated PSMA‐positive lesions (70% vs 50%), less frequently experienced local recurrences only (12% vs 26%), and more often had positive lymph nodes (13% vs 5%) with or without a macroscopically persisting tumour in the prostatic fossa (45% vs 19%). Results from PSMA‐PET/CT changed the initial treatment of sRT in so far as all patients with positive lesions underwent a combination of sRT and ADT. In patients with isolated, intrapelvic lymph node metastases attributable to an improperly performed extended pelvic lymphadectomy, salvage lymphadectomy might also be integrated into the therapeutic armamentarium, resulting in a long‐term relapse‐free survival of ~40%.
Even patients with persisting PSA serum concentrations after undergoing RP exhibit a heterogeneous clinical course of the disease, therefore, a risk‐adapted, personalized approach stratifying biologically aggressive from less aggressive prostate cancer should be adopted. In a retrospective study in 925 patients who underwent sRT, PSA persistence was associated with a significantly lower 8‐year metastasis‐free survival rate when compared to patients with PSA relapse following undetectable postoperative PSA serum concentrations [3]. Furthermore, it was shown that PSA persistence and a Gleason score ≥8 were independent, statistically significant predictors for systemic metastases, with a hazard ratio of 4.64 (95% CI 3.06–7.02; P < 0.001) and 8.37 (95% CI 4.15–16.88; P < 0.001), respectively. Patients with both PSA persistence and Gleason score ≥8 had a significantly lower 8‐year metastasis‐free survival rate as compared with patients with only PSA persistence (62% vs 74%); therefore, the latter might be best treated with a combined approach of sRT and ADT.
Integration of molecular markers might be helpful to identify those patients who will benefit from sRT. Spratt et al. [7] evaluated whether a 22‐gene genomic classifier could independently predict development of metastasis in 477 patients with PSA persistence postoperatively. Among those with detectable PSA, the 5‐year metastasis rate was 0.90% for genomic low/intermediate and 18% for genomic high risk (P < 0.001). Genomic high risk remained independently prognostic on multivariable analysis (hazard ratio 5.61, 95% CI 1.48–22.7; P = 0.01) among patients with detectable PSA. The C‐index for the combination of the genomic classifier with Cancer of the Prostate Risk Assessment (CAPRA) score was 0.82.
In summary, modern management of persistent PSA serum concentrations after RP needs to take into consideration the pathohistology of the RP and lymph node specimens, results from PSMA‐PET/CT, molecular markers associated with relapse and response as well as individualized therapeutic strategies such as sRT ± ADT, salvage lymphadenectomy and additional salvage radiation to oligometastatic sites.
Today, Dr Veeru Kasi of University College London, presented the results of the PRECISION (PRostate Evaluation for Clinically Important disease: Sampling using Image-guidance Or Not?) study in the “Game Changing” Plenary session at the #EAU18 Annual Meeting in Copenhagen. The accompanying paper was simultaneously published in the New England Journal of Medicine. And it is stunning! Everyone in the packed eURO auditorium knew they were witness to a practice-changing presentation, and the swift reaction on social media around the world confirms this.
PRECISION: MRI-targeted biopsy strategy leads to fewer men needing biopsy. Article with video interviews with Veeru Kasivisvanathan and Declan Murphy https://t.co/QXaWZLaBvo
— European Association of Urology (EAU) (@Uroweb) March 19, 2018
Congratulations to Veeru (a second year urology resident in London), senior author Dr Caroline Moore, Prof Mark Emberton, and all the collaborators on this multicenter international trial. I had the great privilege to be the Discussant in the Plenary session so have been digesting this study in detail for the past few weeks.
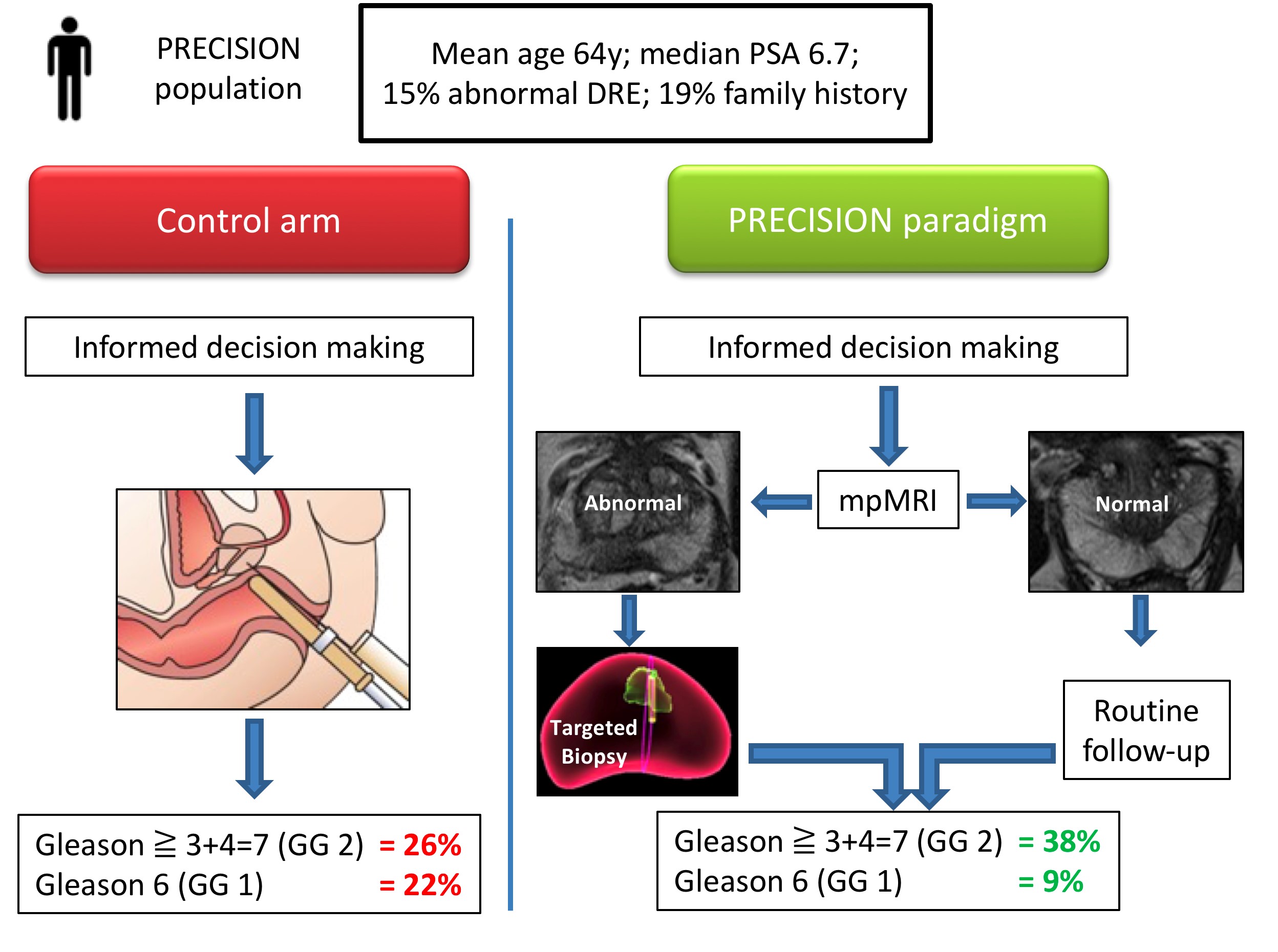
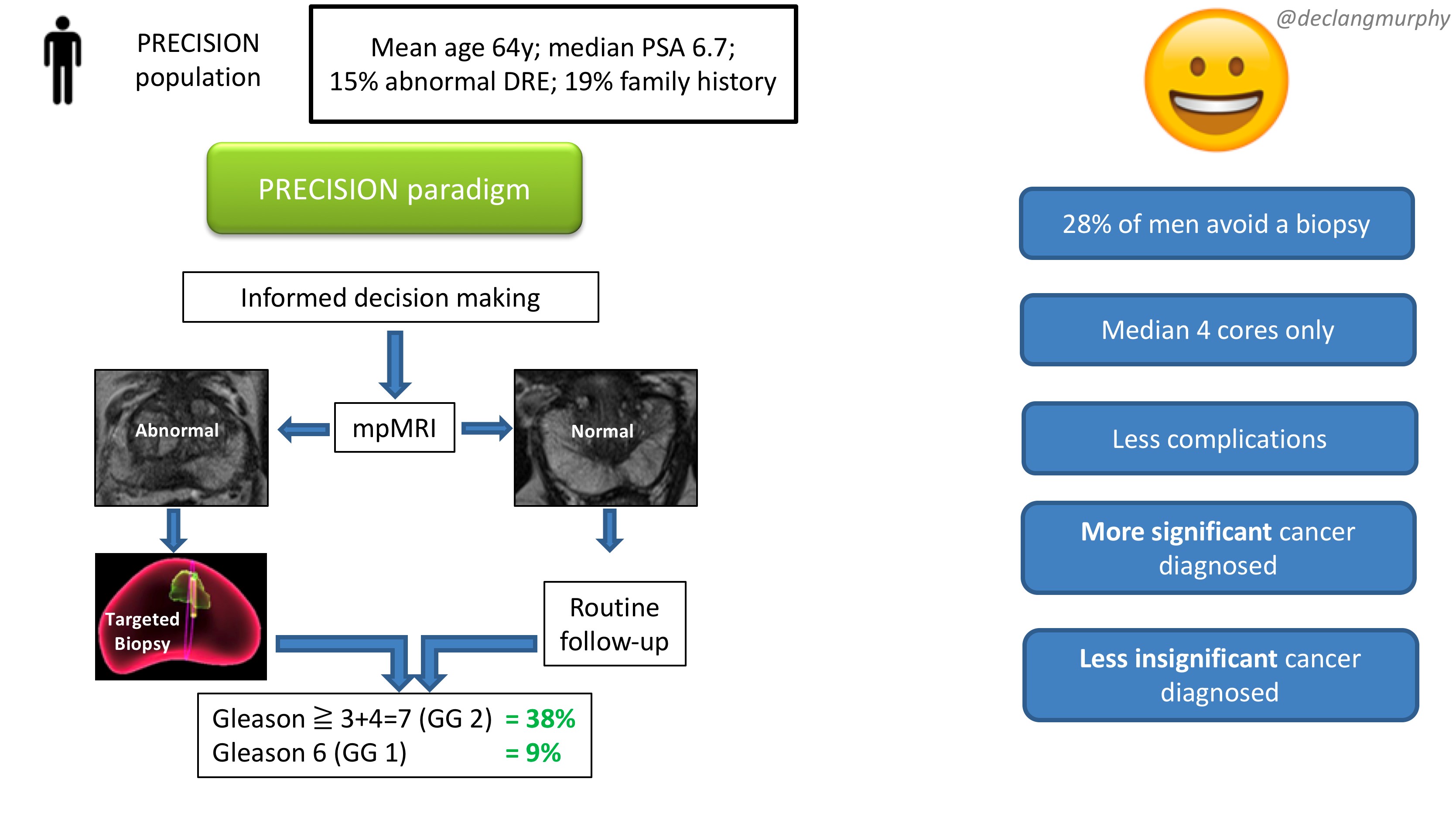
Let me summarise the PRECISION study in brief. In this multicenter international study, 500 men with a suspicion of prostate cancer (mean age 64, median PSA 6.7), were randomised to receive a standard of care (SOC) diagnostic pathway (12 core TRUS biopsy), or an MRI directed pathway. In the MRI pathway, all patients had an MRI, and if the MRI was abnormal (72% of men), they had a targeted biopsy of the lesion(s) (with no systematic biopsy; ie only the abnormal lesion was biopsied). If the MRI was normal (28% of men), they did not have a biopsy, and continued on routine PSA surveillance. The primary outcome was detection rate of clinically significant cancer; and secondary outcomes included the detection rate of clinically insignificant cancer. In the standard of care arm, the detection rate of clinically significant cancer was 26%, and the detection rate of clinically insignificant cancer was 22%. In the MRI pathway, the detection rate of clinically significant cancer was 38%, and the detection rate of taking insignificant cancer was 9%. This is depicted below in one of my summary slides from the plenary discussion.
Therefore, despite the fact that over one quarter of men in the MRI pathway actually avoided a biopsy, the detection rate of clinically significant cancer was much greater in this arm (ie UNDER-diagnosis was reduced). Furthermore, the detection rate of the clinically insignificant cancer was much less (ie OVER-diagnosis was reduced). And all this with a median number of biopsy cores of only four, compared with 12 in the SOC arm. The reduction in core numbers along that too much less complications for these patients.
This looks like WIN-WIN all round!
And I truly believe that these findings should provoke an immediate change in our diagnostic pathway for early prostate cancer in two ways:
All patients with a clinical suspicion of prostate cancer should be offered an MRI as part of their informed/shared decision making pathway
All patients with an abnormality on their MRI scan should be offered be targeted biopsy alone.
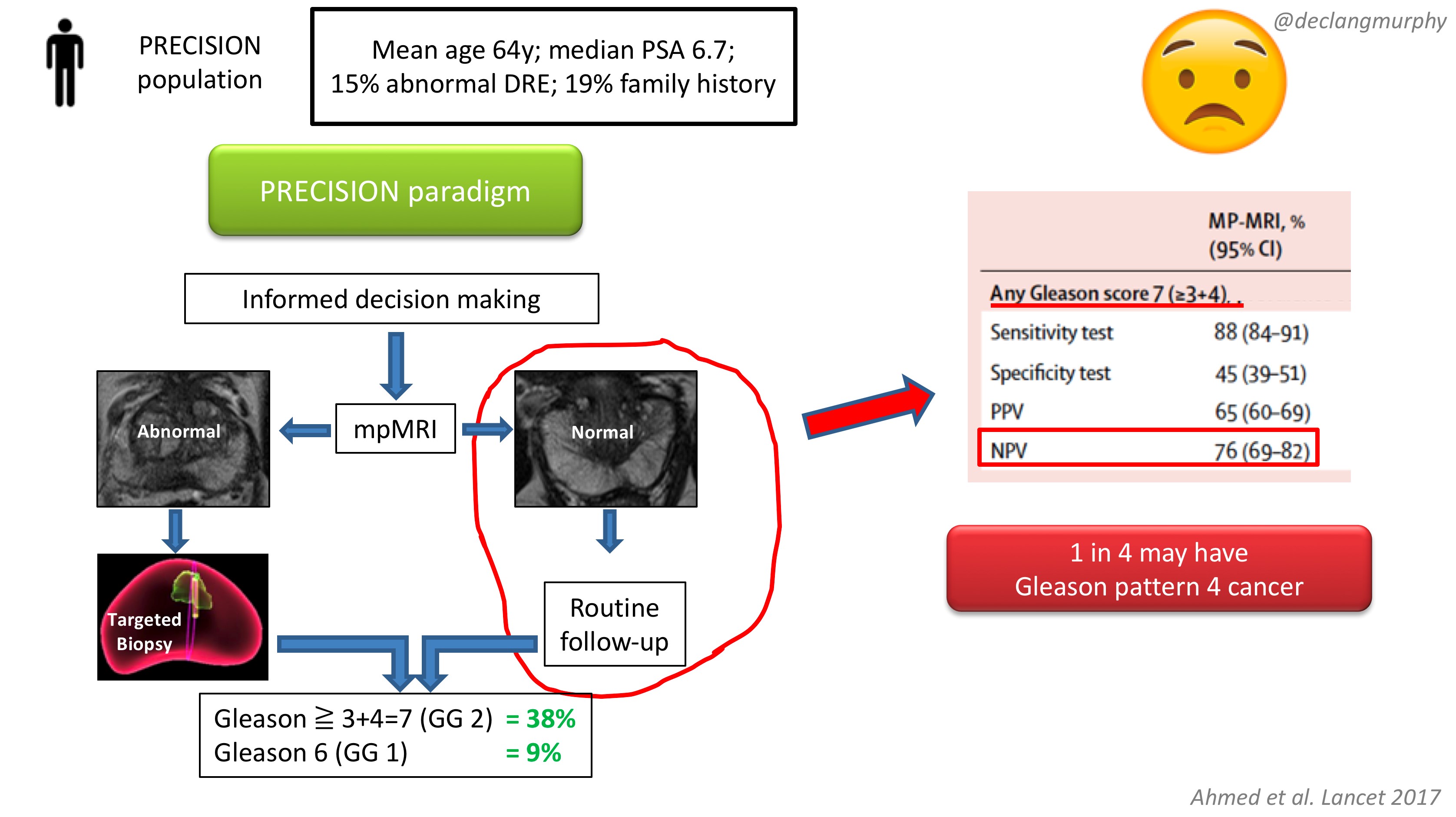
The obvious concern of course, is the fate of those patients with a normal MRI (28% of patients), who despite a clinical suspicion of prostate cancer, did not have a biopsy. How many clinically significant cancers might we miss by not offering biopsy to those patients? Of course, we already have an idea of what we would find, as the PROMIS study also included extensive biopsy (transperienal mapping) for patients with a normal MRI.
In PROMIS, the negative predictive value of MRI for detecting any pattern 4 cancer is 76% ie up to 1 in 4 men will have some pattern 4 cancer on transperineal biopsy. However, no primary pattern 4 cancers were missed on MRI. This is something we have to digest. I think that we can accept missing some pattern 4 cancers in some men, provided the “routine follow up” is adequate. But we must also continue to use the other tools we have in our multivariable approach to early detection, and if there are red flags due to family history, palpable nodules, adverse PSA parameters (including PSA density), BRCA mutations, then there will clearly be a role for systematic biopsy in some of these men with normal MRI scans.
In my opinion, we now have enough evidence to fully embrace mpMRI in our approach to early detection of prostate cancer. Following on from the PROMIS study, published in the Lancet 2017, the PRECISION study provides us with the imprimatur to fully embed MRI in the assessment of men with a suspicion of prostate cancer. The era of blind random prostate biopsy is surely over, except perhaps in those patients in whom MRI is contra-indicated. The next challenge will be to create enough capacity and expertise to make this paradigm available to all.
Resourcing will inevitably be an issue, but the PROMIS and PRECISION papers provide a compelling health economic argument for funders. Less men undergoing biopsy; less biopsy cores; less complications; less insignificant cancer – this surely makes economic sense. In Australia, where MRI has already been enthusiastically embraced, a high-quality mpMRI on a 3T machine costs $USD300, and costs are usually borne by patients. In the USA, we hear that a 1.5T MRI (with an endorectal coil) can cost USD$2-3000!! Why is this?! Australia is an expensive country – an iPhone or a da Vinci robot costs 1.5 times the cost in the USA; why therefore should an MRI cost so much in the USA? A symptom of a much broader issue with the bloated US health economy, and likely a barrier to adoption of the paradigm proposed by PRECISION.
So there you have it. A truly practice-changing study. While there will be much discussion about the nuances, I for one will immediately embrace this paradigm:
MRI for all (I already do this)
Targeted biopsy alone for those with MRI lesions (a new departure for me)
No biopsy for those with normal MRI scans (unless there are other red flags).
My concluding slide from the plenary discussion:
Congrats again Veeru, Caroline, Mark and colleagues for publishing this landmark study.
Declan G Murphy
Urologist & Director of Genitourinary Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia
Every Month the Editor-in-Chief selects an Article of the Month from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorialwritten by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Prediction of pathological stage based on clinical stage, serum prostate-specific antigen, and biopsy Gleason score: Partin Tables in the contemporary era
Tosoian, J. J., Chappidi, M., Feng, Z., Humphreys, E. B., Han, M., Pavlovich, C. P., Epstein, J. I., Partin, A. W. and Trock, B. J. (2017), Prediction of pathological stage based on clinical stage, serum prostate-specific antigen, and biopsy Gleason score: Partin Tables in the contemporary era. BJU International, 119: 676–683. doi: 10.1111/bju.13573
Abstract
Objective
To update the Partin Tables for prediction of pathological stage in the contemporary setting and examine trends in patients treated with radical prostatectomy (RP) over the past three decades.
Patients and Methods
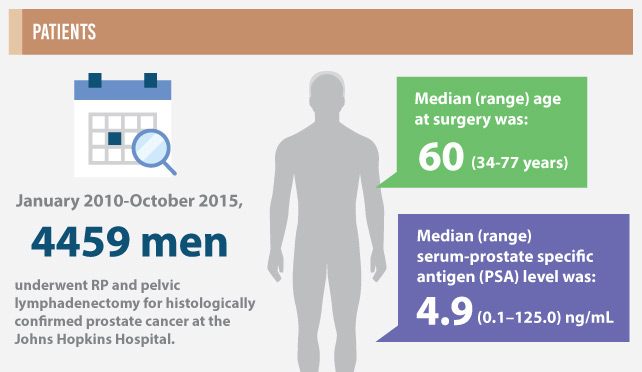
From January 2010 to October 2015, 4459 men meeting inclusion criteria underwent RP and pelvic lymphadenectomy for histologically confirmed prostate cancer at the Johns Hopkins Hospital. Preoperative clinical stage, serum prostate-specific antigen (PSA) level, and biopsy Gleason score (i.e. prognostic Grade Group) were used in a polychotomous logistic regression model to predict the probability of pathological outcomes categorised as: organ-confined (OC), extraprostatic extension (EPE), seminal vesicle involvement (SV+), or lymph node involvement (LN+). Preoperative characteristics and pathological findings in men treated with RP since 1983 were collected and clinical-pathological trends were described.
Results
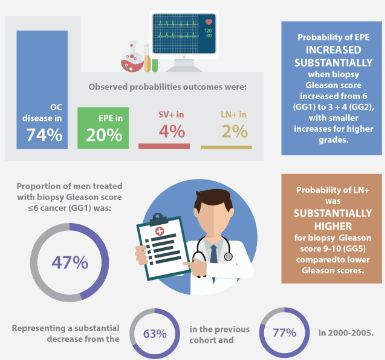
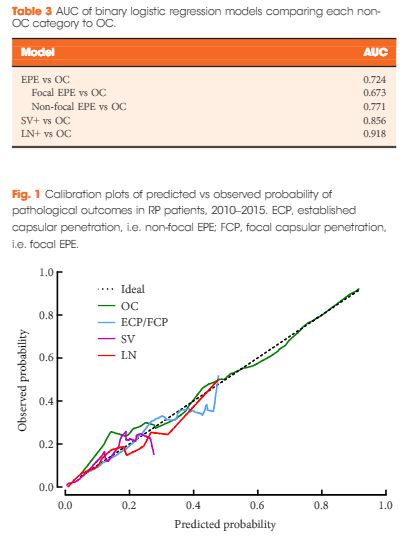
The median (range) age at surgery was 60 (34–77) years and the median (range) PSA level was 4.9 (0.1–125.0) ng/mL. The observed probabilities of pathological outcomes were: OC disease in 74%, EPE in 20%, SV+ in 4%, and LN+ in 2%. The probability of EPE increased substantially when biopsy Gleason score increased from 6 (Grade Group 1, GG1) to 3 + 4 (GG2), with smaller increases for higher grades. The probability of LN+ was substantially higher for biopsy Gleason score 9–10 (GG5) as compared to lower Gleason scores. Area under the receiver operating characteristic curves for binary logistic models predicting EPE, SV+, and LN+ vs OC were 0.724, 0.856, and 0.918, respectively. The proportion of men treated with biopsy Gleason score ≤6 cancer (GG1) was 47%, representing a substantial decrease from 63% in the previous cohort and 77% in 2000–2005. The proportion of men with OC cancer has remained similar during that time, equalling 73–74% overall. The proportions of men with SV+ (4.1% from 3.4%) and LN+ (2.3% from 1.4%) increased relative to the preceding era for the first time since the Partin Tables were introduced in 1993.
Conclusions
The Partin Tables remain a straightforward and accurate approach for projecting pathological outcomes based on readily available clinical data. Acknowledging these data are derived from a tertiary care referral centre, the proportion of men with OC disease has remained stable since 2000, despite a substantial decline in the proportion of men with biopsy Gleason score 6 (GG1). This is consistent with the notion that many men with Gleason score 6 (GG1) disease were over treated in previous eras.
The identification of men with localised prostate cancer at higher risk of adverse pathological outcomes after radical prostatectomy (RP) would assist physicians in preoperative patient counselling and in tailoring the most appropriate treatment strategy. In this issue of the BJUI, Tosoian et al. [1] have updated the Partin Tables in contemporary patients with localised prostate cancer. The authors should be commended for undertaking a well-performed study evaluating a large cohort of patients treated at a high-volume centre. Notably, they were able to show that the Partin Tables still represent an accurate tool for identifying men at higher risk of adverse pathological features [1]. Having said this, the first question we should ask ourselves is whether preoperative models based on clinical variables only still play a role in contemporary patients. The Partin Tables were developed in 1993 and since then they have undergone a series of updates, all of which are based on virtually the same variables included in the original analyses [1]. However, recent implementations, including biomarkers and imaging, have been introduced to better stage prostate cancer. These novel approaches are usually added to clinical variables to improve patient risk stratification. Multi-parametric MRI (mp-MRI) represents the major game changer in this setting, being now recommended for prostate cancer staging in all men with high-risk disease and in those with less favourable intermediate-risk prostate cancer [2]. In the era of modern and sophisticated approaches, are models using clinical variables only still clinically valuable? To answer this question, we can consider two major settings, namely nodal and local staging.
Similarly, when considering local staging, mp-MRI is characterised by a high specificity but a relatively low sensitivity in detecting small, microscopic foci of extracapsular extension and seminal vesicle invasion (SVI) [6]. Conversely, the updated Partin Tables depicted a predictive accuracy of >80% in predicting SVI, despite the lack of individualised data on the extent and volume of extraprostatic extension. For all these reasons, clinical risk models still represent the cornerstone for the identification of men at higher risk of adverse pathological findings. Additional data coming from sophisticated imaging modalities may further improve individualised risk predictions [6] and better assist clinicians in tailoring the most appropriate treatment approach. However, imaging and biomarkers should complement, rather than substitute, currently available clinical risk models.
In conclusion, preoperative predictive tools based on clinical parameters still play an important role in the management of patients with clinically localised prostate cancer. Any staging model including additional approaches, such as imaging and/or biomarkers, is welcomed only when it is shown to improve prostate cancer staging in terms of both accuracy and cost-effectiveness.
Gandaglia, G., Fossati, N., Dell’Oglio, P., Montorsi, F. and Briganti, A. (2017), Is there a role for pure clinical prediction models in prostate cancer in the contemporary era?. BJU International, 119: 652–653. doi: 10.1111/bju.13833
GiorgioGandaglia,*† NicolaFossati,*†PaoloDell’Oglio,*†FrancescoMontorsi,*† and AlbertoBriganti*†
It should surprise no one that I never agreed with the 2012 United States Preventive Services Task Force to give PSA a “D” rating that has led to decreases in U.S. rates of PSA testing, biopsies, and diagnosis of low- through high-risk cancer. I take care of men with prostate cancer in a multidisciplinary clinic at a dedicated cancer hospital. I perform robotic surgeries and manage over a 1,000 men on active surveillance. If you search the BJUI blogs, you can find the often viewed (>80K) “Melbourne Consensus Statement on Prostate Cancer Testing” that included 15 authors who produced 5 consensus statements on the topic. There are 62 comments—comment #5 is a fairly famous one that equates the panel to “a group of 10 pig-farmers telling us we should eat more bacon.” So yes, I think I count as a pig farmer here. My maternal grandfather and great uncle farmed pigs in Western Tennessee, so it does run in the family.
Figure 1: It was either this or robotics
That said, it always seemed odd, that as a large country and major healthcare market, we rolled out PSA screening in the 1990s with wild enthusiasm and without data on benefit, only to then try and roll it back in when faced with two conflicting level 1 evidence studies. Meanwhile, the American Urological Association guidelines recommended PSA screening (with the “shared decision making caveat”)—mostly mirroring the European study—for men ages 55-69 (also consensus statement 1 from the Melbourne consensus). However, a recent fact struck me during a conference talk—Urologists in the U.S. are estimated to order <10% of all PSA tests, and a vast majority are from primary care physicians. So in essence it doesn’t matter as much what we think of one guideline versus another, it’s what the primary care specialties think that matters. As the USPSTF is targeted at primary care, their D rating did have an effect—fewer PSA tests, biopsies, and diagnosis of all grades of cancer (not just Gleason 6). We have heard stories over the years that specialty exams in primary care were starting to feature PSA screening questions, and the “don’t screen” answer was the one you got credit for. But I was also never convinced that most primary care physicians were comfortable with abandoning screening either. They must have seen what we saw—real cancers presenting later stage.
Some memorable quotes along these years of debate:
“There is no evidence prostate carcinogenesis has declined.” Joel Nelson, J Urol 2015
“I believe the USPSTF recommendations have created confusion at the patient and primary physician level, and that this confusion did not likely result in more informed, shared decision making, but instead avoidance of the issue.” Samir Taneja, J Urol.
Amen. So now it’s 2017 and the USPSTF has looked at the data again. They’ve had their “analysis” methods on the web for a while so we know something was planned. I can’t find authorship credits anywhere—we always complained that no prostate cancer experts were involved in the past, and now wondering who is driving this ship. The take home messages are:
Offer PSA screening to ages 55-69 with shared decision making. The narrative is not “do screening.” It’s a full paragraph with the often told caveats of individualized decisions, potential harms and benefits. It’s limited to the reduction in mortality way of thinking, i.e. no thought to preventing metastatic progression, palliative care, etc.
Don’t screen in men ages 70 and older. From an evidence standpoint—hard to argue and the AUA guidelines are similar. The Melbourne Consensus is at least polite enough to point out that not all men over age 70 are going to drop dead any minute, and maybe some of them should be screened if very healthy (level of evidence = CS for common sense).
We recognized that men with a family history of prostate cancer or African American race are higher risk, but we don’t have evidence to support a different screening policy. Again—hard to argue with the evidence and the AUA says the same.
So really that’s it—3 main concepts. This is likely to be a significant impact in the U.S., depending upon whether or not primary care physicians change practice (and their exam questions are the same with a different correct answer).
Probably what is on your mind now is “why the change.” It does not appear to be one thing—not even recent publications revealing a more significant pattern of PSA contamination in the PLCO trial. The checklist seems to include: 1) PCLO “issues”, 2) more data from ERSPC and its subsets, 3) more data on treatment benefit, and 4) increased use of active surveillance in low-risk disease. So the balance tipped in favor of a “C” although they state the benefits and harms are still close. Fair enough.
As I re-read the 2013 Melbourne Consensus and compare to the 2017 USPSTF statement, there is a lot of overlap now. So congrats to the Melbourne group for getting it right in the first place. I, myself, did not see this coming—just another example of why I don’t invest in individual stocks or otherwise pretend to know the future.
I apologize as I re-read this, as I realize we Americans think the world revolves around us. Many of you certainly live in countries that are against routine screening and manage to get by. By all means, please sound off on what you think this means for the international picture of men’s health.
Figure 2: Scenic Melbourne at dusk
John W. Davis is BJUI Associate Editor for oncology. @jdhdavis
Comments on this blog have been closed due to high levels of spam.
Every week the Editor-in-Chief selects an Article of the Week from the current issue of BJUI. The abstract is reproduced below and you can click on the button to read the full article, which is freely available to all readers for at least 30 days from the time of this post.
In addition to the article itself, there is an accompanying editorial written by a prominent member of the urological community. This blog is intended to provoke comment and discussion and we invite you to use the comment tools at the bottom of each post to join the conversation.
If you only have time to read one article this week, it should be this one.
Value of 3-Tesla multiparametric magnetic resonance imaging and targeted biopsy for improved risk stratification in patients considered for active surveillance
To evaluate the role of multiparametric magnetic resonance imaging (mpMRI) of the prostate and transrectal ultrasonography guided biopsy (TRUS-Bx) with visual estimation in early risk stratification of patients with prostate cancer on active surveillance (AS).
Patients and Methods
Patients with low-risk, low-grade, localised prostate cancer were prospectively enrolled and submitted to a 3-T 16-channel cardiac surface coil mpMRI of the prostate and confirmatory biopsy (CBx), which included a standard biopsy (SBx) and visual estimation-guided TRUS-Bx. Cancer-suspicious regions were defined using Prostate Imaging Reporting and Data System (PI-RADS) scores. Reclassification occurred if CBx confirmed the presence of a Gleason score ≥7, greater than three positive fragments, or ≥50% involvement of any core. The performance of mpMRI for the prediction of CBx results was assessed. Univariate and multivariate logistic regressions were performed to study relationships between age, prostate-specific antigen (PSA) level, PSA density (PSAD), number of positive cores in the initial biopsy, and mpMRI grade on CBx reclassification. Our report is consistent with the Standards of Reporting for MRI-targeted Biopsy Studies (START) guidelines.
Results
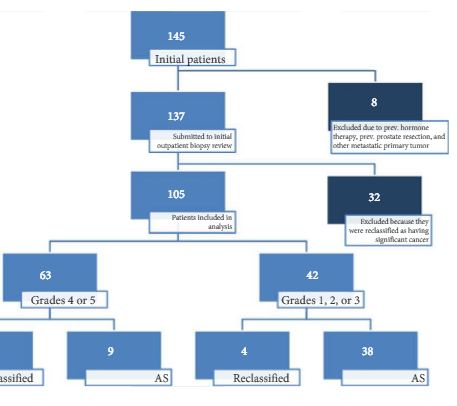
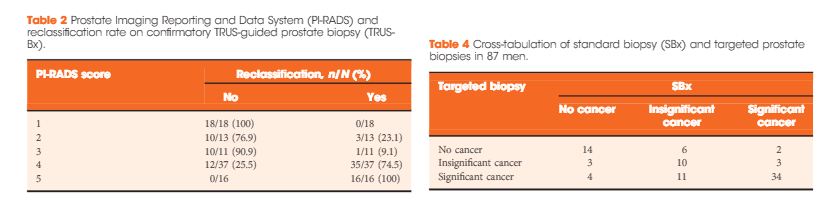
In all, 105 patients were available for analysis in the study. From this cohort, 42 (40%) had PI-RADS 1, 2, or 3 lesions and 63 (60%) had only grade 4 or 5 lesions. Overall, 87 patients underwent visual estimation TRUS-Bx. Reclassification among patients with PI-RADS 1, 2, 3, 4, and 5 was 0%, 23.1%, 9.1%, 74.5%, and 100%, respectively. Overall, mpMRI sensitivity, specificity, positive predictive value, and negative predictive value for disease reclassification were 92.5%, 76%, 81%, and 90.5%, respectively. In the multivariate analysis, only PSAD and mpMRI remained significant for reclassification (P < 0.05). In the cross-tabulation, SBx would have missed 15 significant cases detected by targeted biopsy, but SBx did detect five cases of significant cancer not detected by targeted biopsy alone.
Conclusion
Multiparametric magnetic resonance imaging is a significant tool for predicting cancer severity reclassification on CBx among AS candidates. The reclassification rate on CBx is particularly high in the group of patients who have PI-RADS grades 4 or 5 lesions. Despite the usefulness of visual-guided biopsy, it still remains highly recommended to retrieve standard fragments during CBx in order to avoid missing significant tumours.
The other day, as the New York Times was getting excited about Nobel Laureate Bob Dylan new album ‘Triplicate’, I had the opportunity of remembering one of his classic songs. Let me explain. I turned up at the School of Surgery in central London for an academic committee meeting early that morning only to find that it had been cancelled. Due to a IT problem the email with this information never reached me! Rather than brave the London tube again, I decided to walk back to my hospital, which took me past my old hospital which sadly no longer exists.
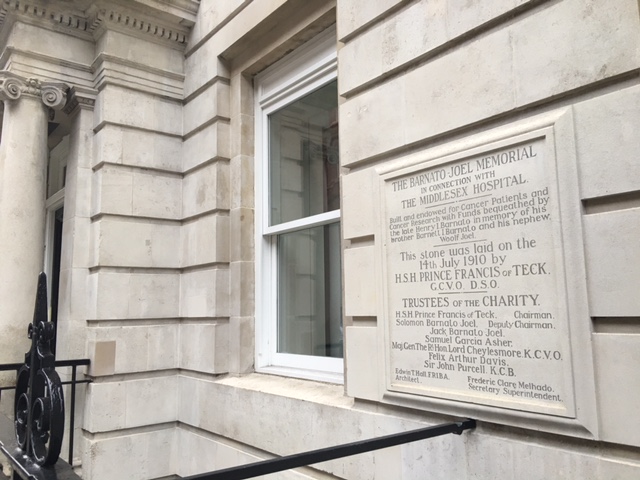
The old hospital in question was The Middlesex Hospital in Mortimer Street, London (Fig.1). The original institution was built in 1745 at Windmill Street and moved in 1757 to Mortimer Street. I arrived there over 20 years ago to train at the Institute of Urology/St. Peter’s Hospital, a highly desirable post amongst surgical residents.
The Middlesex Hospital was closed in 2005 and sold to developers. It now houses swanky apartments and businesses around a beautiful Pearson Square, named after John Loughborough Pearson, who designed the Fitzrovia Chapel (Fig. 2) in 1890 inside the hospital. The Chapel survived the redevelopment as it is a protected building. So did one of the walls of the old hospital along Nassau Street which housed the radiotherapy building (Fig. 3). That facade has been preserved beautifully although there are no patients housed behind it anymore (Fig. 4).
So why I am telling you all this? Nostalgia you may say. But in fact much more. The 3 mile walk that morning allowed me to reflect on my own contribution to science and that of two friends who although slightly ahead of me in the training program at The Middlesex Hospital are gentlemen that I greatly admire.
As for me, I headed to Queen Square from The Middlesex Hospital, where many years of basic research in a Medical Research Council (MRC) funded lab led to the description of the so called “Dasgupta technique” of injecting Botox into overactive bladders. I was pleasantly surprised to hear that it had made its way into a number of texts including Smith’s Textbook of Endourology.
There are however certain things that do not change much. Next to the Middlesex Hospital, on Cleveland Street was the legendary Ragam’s (Fig. 5), which many would regard as THE go to South Indian restaurant. The masala dosa (pancake with spicy potatoes and hot lentil soup) used to cost £3.95 in 1994; 20 years later the price has gone up by only £2 to £5.95 (Fig. 6), while the quality remains as outstanding as ever.